
Abstract
As cancer is overtaking cardiovascular disease as the leading cause of death among diabetics, improved cancer prevention efforts are needed for individuals with diabetes. In this research letter, we used data from the US National Health Interview Survey to examine the use of screening for two major diabetes-related cancers, colorectal cancer, and breast cancer, in individuals with and without diabetes. We found that individuals with diabetes had slightly higher use of colorectal cancer screening and similar use of breast cancer screening compared to those without diabetes in the US. Besides, despite the increasing use of colorectal cancer and breast cancer screening over the past 10 years, screening uptake remains suboptimal. We believe that these findings provide important data to inform policymaking and cancer prevention efforts.
Diabetics and cancer screening prevalence
Type 2 diabetes has been associated with a higher risk of several cancer types, including colorectal cancer (CRC) and postmenopausal breast cancer.1,2 In fact, cancer is overtaking cardiovascular disease as the leading cause of death among patients with diabetes, highlighting the importance of cancer prevention for the clinical management of diabetes. CRC is the third most commonly diagnosed cancer, accounting for 10% of global cancer incidence and 9.4% of cancer deaths. Breast cancer has overtaken lung cancer as the most commonly diagnosed cancer and is also the second leading cause of cancer death among women globally.3,4 Considering the high prevalence of type 2 diabetes, even a moderate association would explain a considerable proportion of the cancer incidence. However, prior findings on the use of cancer screening in individuals with and without diabetes vary from country to country and from time to time, even the studies focused on the United States remain elusive and inconsistent. 5 Therefore, an updated assessment was needed to better inform resource allocation and clinical practice.
We examined the age-standardized prevalence of CRC and breast cancer screening among participants with and without diabetes from the National Health Interview Survey (NHIS) between 2010 and 2019. Up-to-date CRC screening and breast cancer screening were defined according to the US Preventive Services Task Force (USPSTF) screening recommendations in effect for each year6,7 (see footnotes to Figure 1 and Table 1).
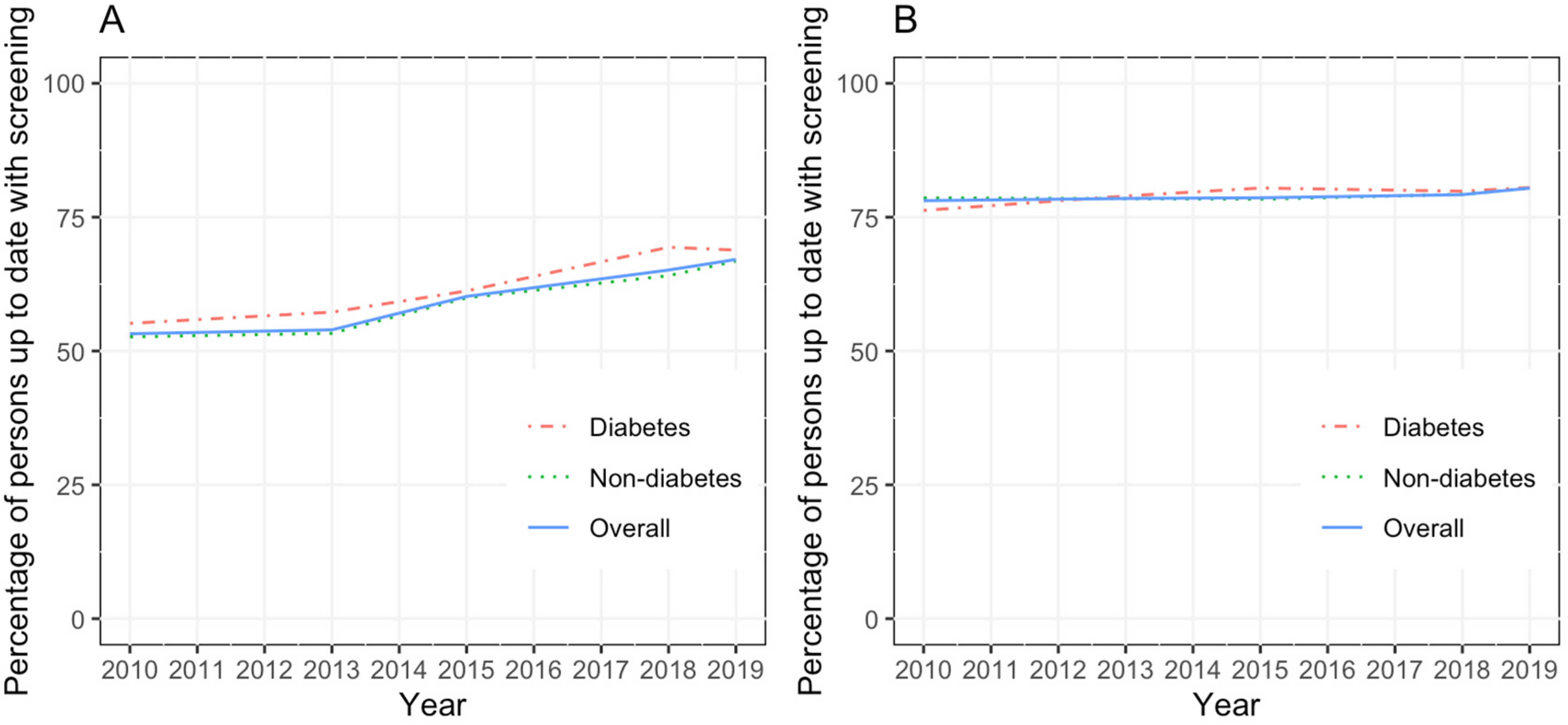
(A) Up-to-date screening prevalence of colorectal cancer (CRC) among people with and without diabetes. (B) Up-to-date screening prevalence of breast cancer among people with and without diabetes. Note. All estimates are age-adjusted to the 2000 standard US population. Up-to-date CRC screening was defined as the use of guaiac fecal occult blood test or fecal immunochemical test within 1 year, sigmoidoscopy or computed tomography colonography within 5 years, colonoscopy within 10 years, or stool DNA test within 3 years among adults aged 50 to 75 years. Up-to-date breast cancer screening was defined as the use of mammography within 2 years among women aged 50 to 74 years.
Association between having diabetes and up-to-date use of colorectal cancer and breast cancer screening according to demographic factors (United States, 2019).
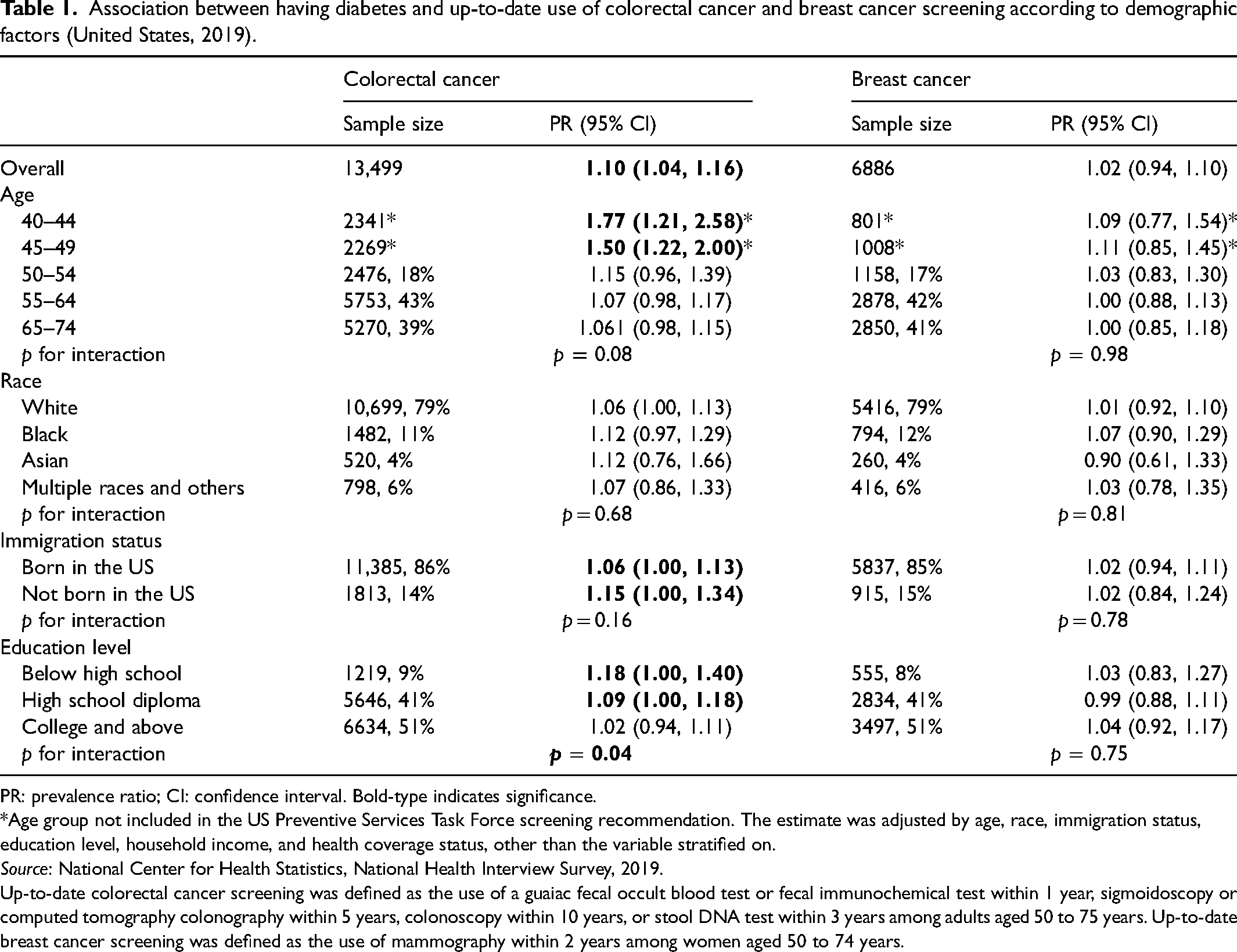
PR: prevalence ratio; CI: confidence interval. Bold-type indicates significance.
*Age group not included in the US Preventive Services Task Force screening recommendation. The estimate was adjusted by age, race, immigration status, education level, household income, and health coverage status, other than the variable stratified on.
Source: National Center for Health Statistics, National Health Interview Survey, 2019.
Up-to-date colorectal cancer screening was defined as the use of a guaiac fecal occult blood test or fecal immunochemical test within 1 year, sigmoidoscopy or computed tomography colonography within 5 years, colonoscopy within 10 years, or stool DNA test within 3 years among adults aged 50 to 75 years. Up-to-date breast cancer screening was defined as the use of mammography within 2 years among women aged 50 to 74 years.
All estimates were age-standardized using the 2000 US standard population. We also calculated the self-reported prevalence ratio of CRC and breast cancer screening, comparing individuals with and without diabetes using the multivariable-adjusted Poisson model. We further conducted the stratified analysis according to these demographic factors and calculated the P value for interaction using the likelihood ratio test.
We found that the self-reported prevalence of up-to-date screening use increased for both CRC and breast cancer between 2010 and 2019. The overall prevalence of CRC screening increased from 52.3% in 2010 to 67% in 2019, and the prevalence of breast cancer screening increased from 78% to 80% (Figure 1). Individuals with diabetes had a slightly higher CRC screening prevalence than those without diabetes (prevalence ratio (PR) = 1.10; 95% CI, 1.04–1.16), whereas no significant difference was found for breast cancer screening (PR = 1.02; 95% CI, 0.94–1.10). We also noticed that people with diabetes are more likely to initiate CRC screening earlier than people without diabetes. The PR of CRC screening is elevated among younger individuals (see Table 1). In the stratified analysis, we found that the association between a history of diabetes and CRC screening use was stronger among individuals without a college degree (p for interaction = 0.04), while no significant differences were found according to other demographic factors.
To the best of our knowledge, the present study is the first to assess the association between having diabetes and cancer screening using the 2010–2019 NHIS data. Our results are consistent with most previous studies in the United States, but different from those from most other countries, and they are also consistent with our stratified analysis result. The higher use of CRC screening by diabetics than non-diabetics may be explained by the higher frequency of encounters with health services and probably more exposure to medical recommendations. This difference was not found for breast cancer screening, possibly because of the epidemiologic evidence suggesting that a colonoscopy should be done before insulin therapy in diabetics to mitigate the potential pro-CRC effect of insulin, whereas little evidence suggests that a mammogram is necessary before diabetes treatment.8,9 Moreover, our study showed that despite the increasing use of CRC screening over the past 10 years (uptake of breast cancer screening is also increasing but only slightly), screening uptake remains suboptimal and needs improvement. A major limitation of our study is the lack of information about age at the initiation of cancer screening in the NHIS. Also, the screening data in NHIS is self-reported, which may result in overestimation.
In conclusion, our findings show that individuals with diabetes had slightly higher use of CRC screening and similar use of breast cancer screening than those without diabetes in the US. It is worth noting that the USPSTF does not address recommendations for groups with certain diseases who have a higher risk. Given the elevated cancer risk and the higher prevalence of unhealthy behaviors that may increase cancer risk in diabetics, further studies are needed to evaluate what sorts of interventions would be effective to motivate people with diabetes to attend screening regularly and whether a tailored approach to cancer screening is needed.
Footnotes
Authors’ contributions
ZL designed the project, performed the statistical analysis, and drafted the paper. MS designed the project, revised the statistical analysis plan, and revised the draft paper.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.