
Abstract
Objective
To describe the development and implementation of a population-based screening programme for sickle cell disease (SCD) implemented in 12 SCD-endemic and tribal-dominated primary/community health centres (PHCs/CHCs) across six districts of India.
Setting
India reports a huge burden of SCD, especially among indigenous (tribal) communities. However, there is no state-led SCD programme in many places, and systematic screening is absent. This situation necessitates developing a model of population screening.
Methods
This programme was meant to screen all people and was carried out in three tiers. The first tier was a symptomatic survey carried out by community health workers. Regular health workers then screened those referred by sickle cell solubility test at sub-health centres as the second tier. The third tier was confirmation by haemoglobin electrophoresis at PHCs/CHCs. Communities were mobilised and prepared to accept the screening. Capacity building of health facilities was ensured through training and supply of equipment and material.
Results
Initial observation based on six months’ data revealed that out of the 110,754 tribal population of 12 PHCs/CHCs, 8418 (7.6%) were identified in the symptomatic survey. Subsequently, 9416 people, including the above 8418, underwent the solubility test, and 2607 (27.7%) were found to be positive. Of these, 1978 (78.9%) underwent electrophoresis. About 64.2% were found to be positive for sickle haemoglobin (233 (18.4%) SCD and 1036 (81.6%) SCD trait).
Conclusions
The study demonstrates the feasibility of establishing a population-based screening programme in the primary health care system. It is easy to implement in tribal habitations as part of the proposed national SCD/haemoglobinopathies programme.
Introduction
Sickle cell disease (SCD) is a hereditary haematological disorder, with about 300,000 children born with SCD every year. 1 India is the second most affected country by SCD births. 2 The public health implications of SCD are enormous. Although SCD has been reported among numerous ethnic groups in India, it is most prevalent among indigenous (tribal) communities, 3 who (104 million) constitute 8.6% of India's total population. Usually, these communities in remote forest areas are deprived of basic amenities, including health care. And their health status and health-seeking behaviour are poor. 4 In addition, SCD prevalence is not monitored in these communities, and screening is almost absent. 5 Despite the high burden of SCD in India, there are no state-led SCD programmes or a public health approach in many places.6,7 As in many developing countries, basic facilities for SCD management are lacking; systematic screening seldom happens, and diagnosis is made late or never happens. 8 In addition, people's knowledge of SCD is poor. 9
This situation necessitates developing and implementing a model of population screening and management of SCD. A community-based screening model through primary health centres (PHCs) was developed. This paper describes the development and implementation of this model of population-based screening, implemented in 12 SCD-endemic and tribal-dominated PHC/ community health centre (CHC) areas spread across six districts of India.
Methodology
In India, there is an excellent infrastructure for delivering health care, including preventive, curative and promotive services, through a network of primary, secondary and tertiary level health institutions. At the primary level are sub-health centres (SHCs) and PHCs. At the secondary level, there are CHCs and sub-district hospitals. Finally, tertiary-level care is provided by the district hospitals and medical college hospitals. An SHC, having at least two health workers, serves a population of 5000 (3000 in tribal areas). Primarily SHCs provide preventive and promotive services in the community. Government is transforming the SHCs into health and wellness centres, to expand the range of services. A PHC would be located in a bigger village and serves a population of 30,000 or more (20,000 in tribal areas), as this larger health clinic is staffed with doctors and paramedics. SHCs function under the PHC. Each PHC serves several villages covering the above-mentioned population distributed across 8–12 SHCs. A CHC, in some places substituting a PHC, serves a population of 120,000 (80,000 in tribal areas). Usually, the CHC is the first referral unit and comprises a few specialists. District hospitals are the final referral or tertiary care centres. At least one such hospital with 75–500 beds exists in each district. In addition, medical college hospitals also provide tertiary care.
The PHC and its SHCs are staffed by health workers and provide primary health care services. There are two categories of health workers: regular health workers and community health workers. Regular health workers include auxiliary nurse-midwives (ANMs) (who have a 2-year diploma in auxiliary nurse-midwifery), nurses (who have a 3.5-year diploma in general nursing and midwifery or a 4-year bachelor's degree in nursing) and other trained personnel like health assistants. The community health workers are accredited social health activists (ASHAs), trained community-level volunteers with eight years of formal education and residents of the village. One ASHA is provided for a population of 1000.
This paper is part of a multicentric study that developed a comprehensive SCD care model in tribal areas through the primary health care system. 10 The health system implemented the screening and management activities of SCD with researchers’ support. Communities were informed and prepared to accept the screening. The care-seeking behaviour of patients (for home-based care) through ASHAs, regular health workers and community members was promoted. A referral system was developed to refer SCD patients from the SHC level onward. Community engagement strategies were used to mobilise the community for the success of the intervention. A web-based registry was established to capture the data of SCD patients on diagnosis, symptoms, triggering events, treatment, and other health-care issues. These interventions are continuing in six districts; namely, Anuppur (in Madhya Pradesh state), Chhotaudepur (in Gujarat state), Kandhamal (in Odisha state), Mysuru (in Karnataka state), Udalguri (in Assam state), and Visakhapatnam (in Andhra Pradesh state) (see Figure 1). In each district, two PHCs/CHCs were selected based on the criterion that tribal populations predominantly inhabit their areas. The population-related details of the selected districts and PHC/CHC areas are given (Table 1). Institutional ethics committees of the six participating institutes where this study was implemented approved the study protocol. Each of these committees approved the protocol for the corresponding study site.
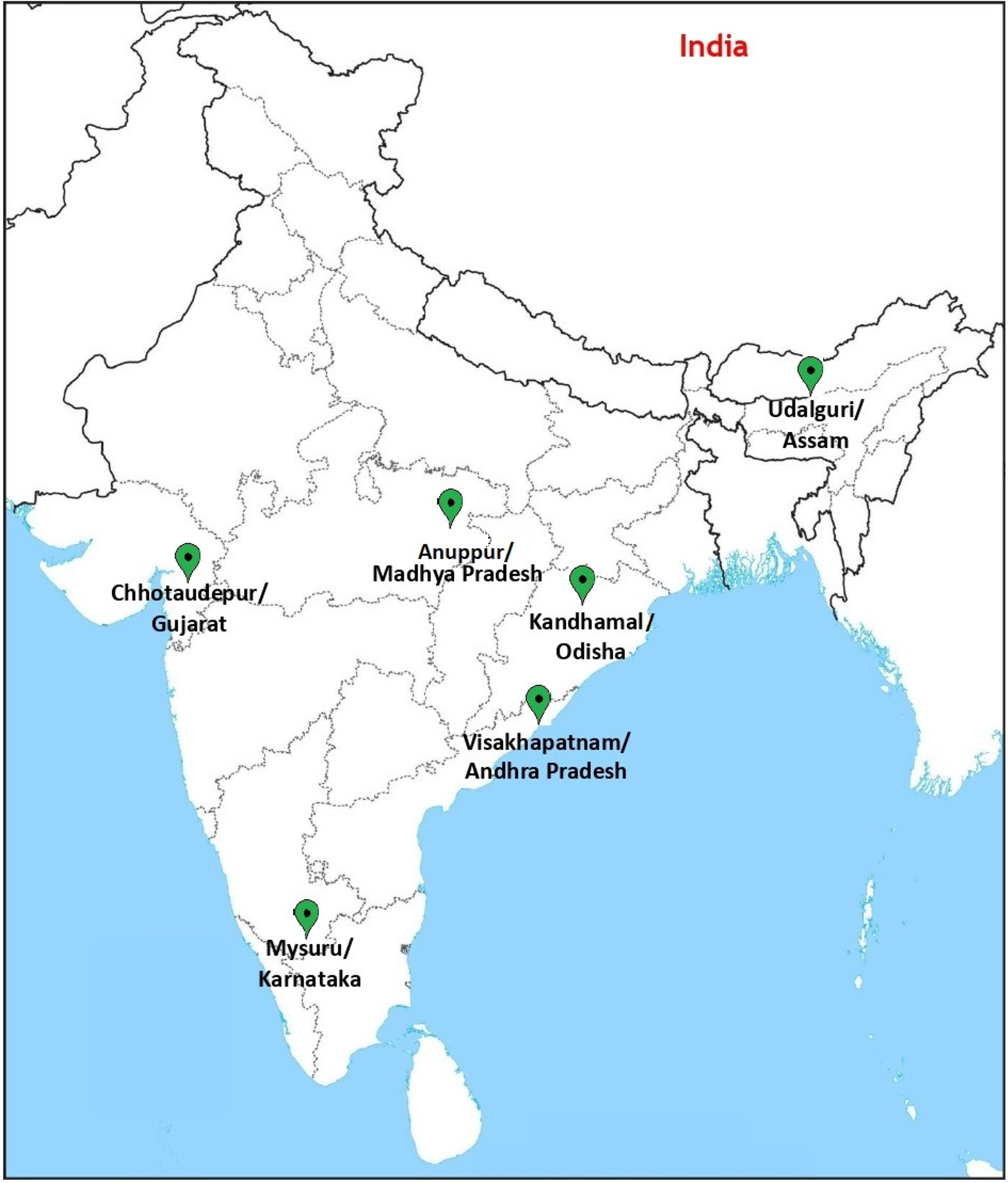
Map showing the location of study sites.
Population details of the study sites.
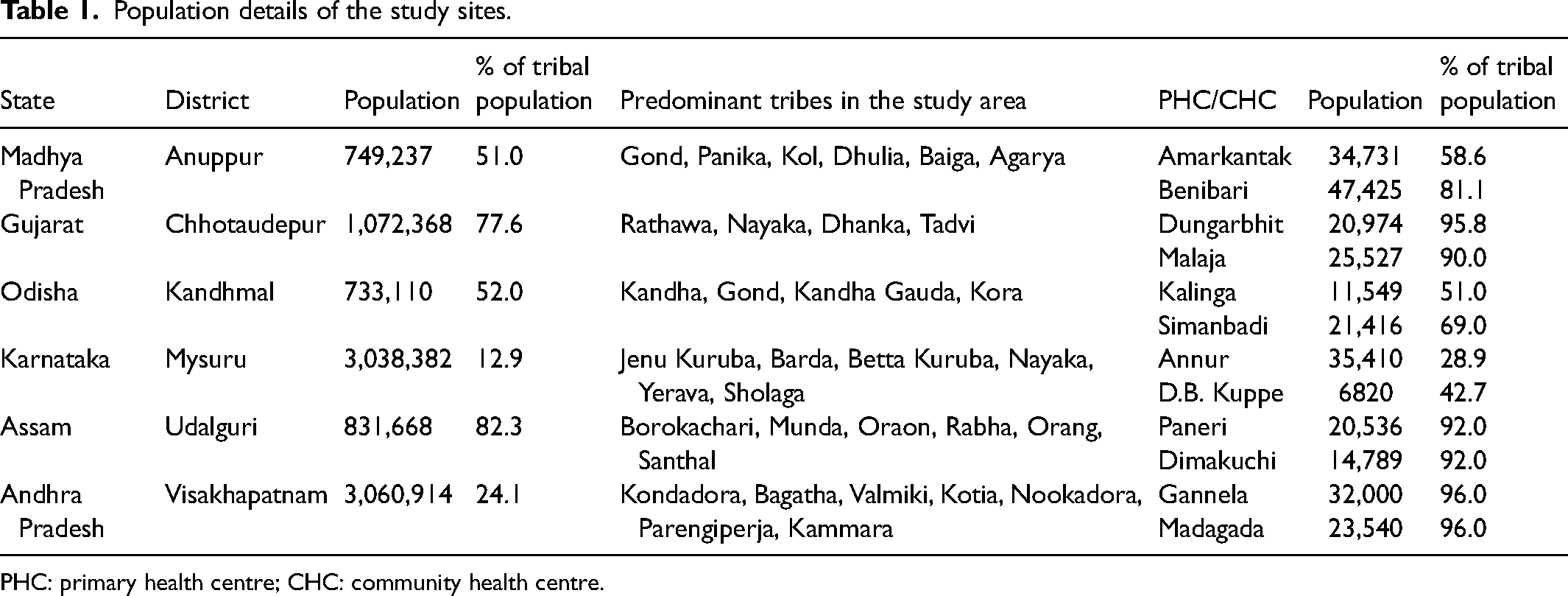
PHC: primary health centre; CHC: community health centre.
Screening
This population-level screening was designed to detect all children and adults who might have SCD. Also, it covered extended family members of known SCD patients and those who specifically wished to get tested. In this context, the extended family is an extension of a nuclear family to include other relatives such as parents, grandparents, siblings, aunts, uncles, cousins, nieces and nephews of the couple. The screening was carried out in three tiers to cover a maximum number of people (Figure 2). In the absence of a state-led screening programme, it was expected that there would be people (both children and adults) living with SCD without being aware of their condition.
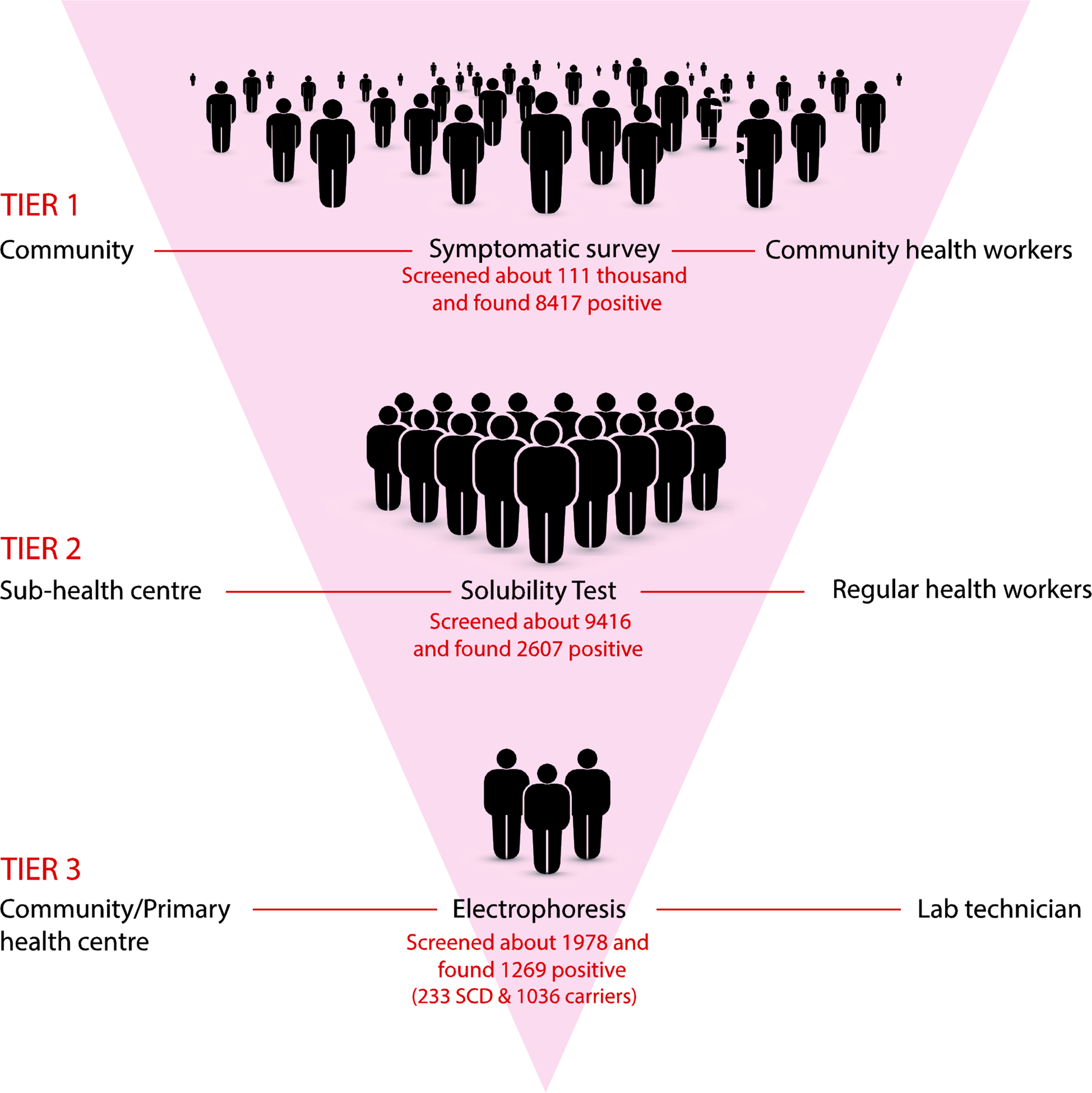
Scheme of population-level screening of sickle cell disease (SCD) in tribal communities of India.
Tier 1: Community-level symptomatic survey
The community health workers, viz. ASHAs, carried out the symptomatic survey as the first tier of screening. A checklist was developed by brainstorming with principal researchers and haematologists, and later it was pre-tested by the principal researchers. This checklist was translated into the local languages. It included 12 symptoms that ASHAs needed to check before confirming an individual suspected of SCD (Supplementary File). ASHAs examined all the people who belonged to tribal communities under their jurisdiction and prepared a list of suspected SCD cases. These cases were referred to the SHC for further diagnosis.
Tier 2: SHC-level solubility test
The people referred from the symptomatic survey were screened by the solubility test as the second tier. The regular health workers were further instructed that if people visited the SHC without an ASHA's referral they should also be screened. This qualitative test was developed based on the principle of the relatively insoluble nature of sickle haemoglobin when mixed with sodium dithionite, a reducing agent. 11 Finger prick blood samples were used, and regular health workers at the SHC conducted these tests instantly. Those positive for the solubility test were recorded and referred to the PHC for confirmation of SCD.
Tier 3: PHC-level confirmatory electrophoresis
The third and final step was the confirmation of SCD status by haemoglobin electrophoresis using cellulose acetate strips in Tris-EDTA-boric acid (TEB) buffer. 12 For this purpose, 2 mL of intravenous blood was collected from each person. In some places, it was not possible for people to visit the PHC/CHC; hence their blood samples were collected at SHCs and sent to the PHC/CHC. The electrophoresis was performed by the PHC/CHC laboratory technicians.
Training and capacity building
The local health system and the research team imparted training to ASHAs, regular health workers and laboratory technicians. ASHAs were trained to recognise suspected patients at the village level through a set of symptoms, as explained above. Role play was used to help them understand the symptoms in the checklist and identify potential cases of SCD.
The regular health workers were trained to conduct and interpret the solubility test using sickle cell solubility test kits. In training, the preparation of the buffer solution, blood sample collection, mixing of the blood sample with buffer, and reading of the results were explained and demonstrated. Specific information concerning the buffer solution (such as effectiveness of the test, storage in the refrigerator, the total number of tests per unit of buffer solution) and registration of each patient undergoing solubility test at SHC level, etc., was provided to all regular health workers. Initially, a few sessions of testing were conducted under the supervision of the research staff.
The laboratory technicians in the PHCs were trained in conducting electrophoresis. This included buffer preparation, application of haemolysate to the cellulose acetate strips, reading and interpreting the results, etc. These training sessions were repeated until the technicians felt confident performing the test. They were trained for hands-on experience, troubleshooting and problem solving to build technical competency and sustain motivation.
Supplies
All necessary equipment was supplied to ensure continuity of the screening process at all levels. This included solubility test kits, buffer kits, markers, labelling stickers, test tubes, etc., supplied to SHCs to conduct tier 2 screening. Equipment (electrophoresis units and power packs), electrophoresis kits, glassware, reagents, etc., necessary for electrophoresis were made available at all the PHCs/CHCs. The drugs used in the treatment of SCD, including hydroxyurea, analgesics, antibiotics, vaccines, etc., were supplied to PHCs/CHCs, mainly by the health system.
Community mobilisation
Community mobilisation, aimed to create awareness of SCD and demand for SCD screening and care, was carried out by extensive information, education and communication activities, including interpersonal communication through health workers. Print materials for this purpose were used widely across the villages. While visiting households, ASHAs explained the symptoms of SCD, nature of the diagnostic tests, benefits of testing, etc. All the ASHAs were instructed to ensure follow-up of the suspected cases, including those who tested positive in the solubility test. Special outreach camps were organised in villages. It was ensured that all those listed as suspected of SCD attended the camp. Despite follow-up by health workers, many patients did not visit the PHC for confirmatory tests. Hence, it was suggested that collecting blood on immunisation day and transporting it in the vaccine carrier would be feasible. Patients were called to the SHC, where regular health workers collected their blood samples and sent them in the vaccine carrier to the PHC/CHC in the cold chain.
Results
Initial observations
The screening programme was initiated for this population in March 2021, and details of the tests at the different tiers for the initial six months (from 1st March 2021 to 31st August 2021) are presented (Table 2). The approximate tribal population living in these 12 PHCs/CHCs of six states is 221,508. Half of this population (110,752) was covered in the first six months. Of this population, 8418 (7.6%) were identified by ASHAs based on symptoms. Additionally, in some places, regular health workers identified individuals who had symptoms of SCD, during immunisation and other routine activities. Also, some people self-reported to SHCs after seeing pamphlets/posters, etc. As a result, 9416 people were tested by regular health workers at SHCs, and out of them 2607 (27.7%) were positive for the solubility test. Of the people who were positive, 1978 (78.9%) underwent haemoglobin electrophoresis. A total of 1269 (64.2%) were found to be positive from this confirmatory test. Of these, 233 (18.4%) had SCD and were added to the registry, and the remaining people (81.6%) were of SCD trait.
Details of population undergoing testing at different tiers during a period of six months.
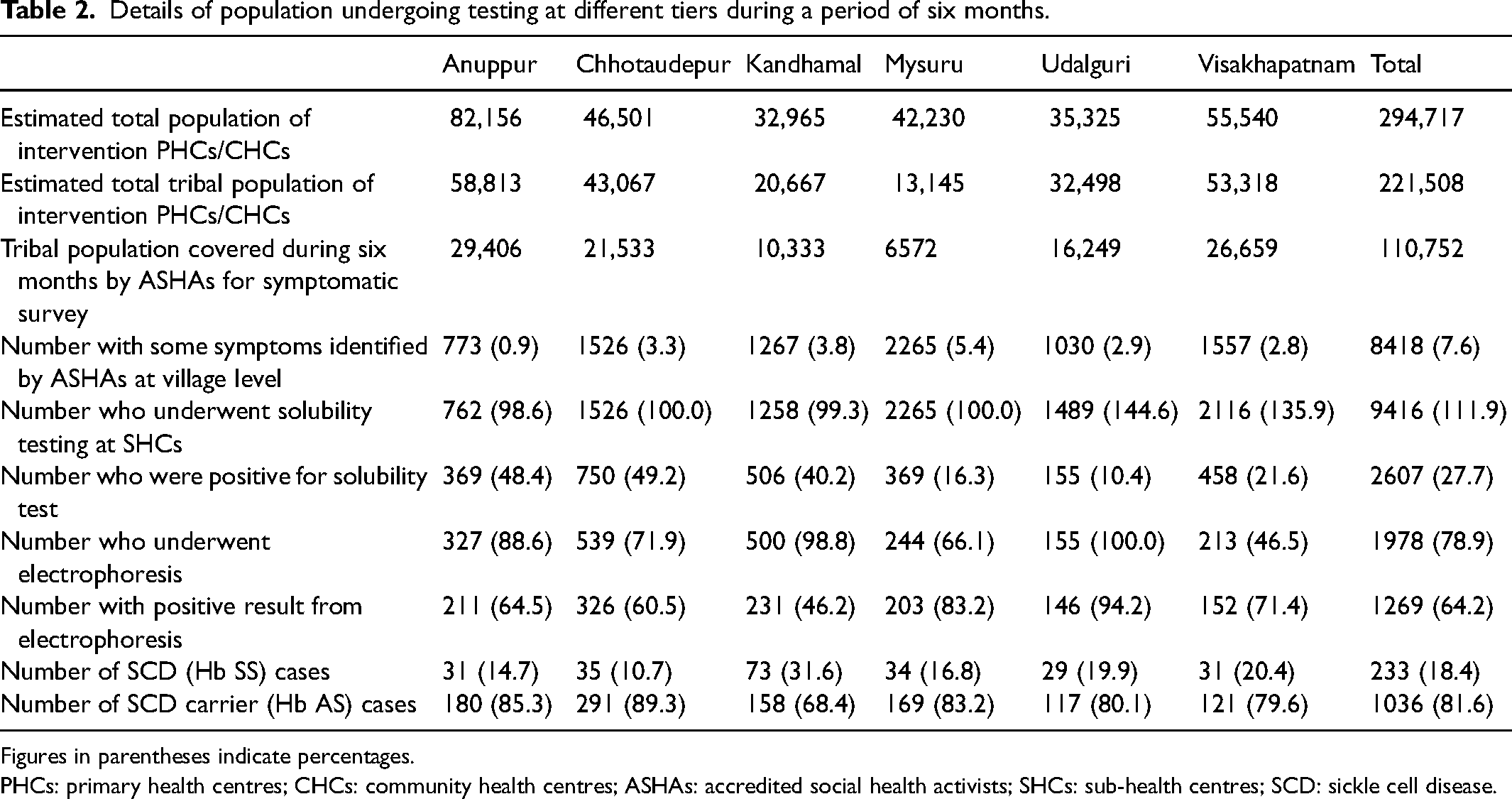
Figures in parentheses indicate percentages.
PHCs: primary health centres; CHCs: community health centres; ASHAs: accredited social health activists; SHCs: sub-health centres; SCD: sickle cell disease.
Expenditure
The total expenditure incurred for this screening process was Indian Rupees (INR) 670,000 (approximately US$9054) per district. Three horizontal electrophoresis units with three power packs costing INR 340,000 (US $4595) were supplied to each district. All other recurring items, such as electrophoresis kits, solubility test kits, glassware, reagents, and other lab consumables, cost about INR 330,000 (US $4460) for one year.
Discussion
This study evidenced the feasibility of SCD screening at the community level using a three-tier system. In the present model, an ASHA identifies potential cases of SCD using a checklist and refers them to the SHC. ASHAs, who are from the same community, are the first point of contact. ASHAs have high credibility and acceptance in the community.13,14 Also, they know about every member of the community. Almost all people who were identified by ASHAs through symptomatic survey went on to undergo the SHC solubility test. In some places, such as Udalguri and Visakhapatnam, regular health workers identified people who directly visited the SHC and underwent the solubility test, due to intense health information at the community level. All solubility test positive patients were sent to the PHC/CHC for confirmatory haemoglobin electrophoresis. SCD-positive patients were then entered into the registry and received treatment, including drugs. However, the visits to PHCs/CHCs depended on several access-related issues, such as distance from home, travel costs, loss of work due to visits, trust in the health facility, etc. Hence, in some places, such as Visakhapatnam, a lower proportion of people accessed the PHC/CHC for confirmatory testing. In these areas, community mobilisation activities were intensified. Also, the results of confirmatory tests varied across the sites. The proportion of SCD cases out of those positive for solubility test and who underwent electrophoresis was higher in Kandhamal compared to other sites. Such differences might be due to variations in the frequency of the sickle haemoglobin gene among these communities.
India's national SCD control programme envisaged screening people, particularly children, for treatment and care. 6 The current model of community-based screening is suitable for India's smaller and scattered distribution of tribal habitations. This model promotes screening at the community level by peripheral health workers. In these communities, the health workers’ visits to households and villages improved their knowledge of SCD. 9 Also, the information given by these health workers may influence the general healthcare-seeking behaviour of the population.15,16 The solubility test is technically easy to conduct and feasible to establish at an SHC or the residence of the health worker (in most cases, SHCs function from regular health workers’ homes). In addition, conducting solubility tests is relatively inexpensive. The sensitivity and specificity of this diagnostic method's positive and negative predictive values are high.17,18 The deployment of electrophoresis units and performance of electrophoresis by technicians at PHCs/CHCs are also feasible and affordable. A similar study in Uganda found that the sickling test followed by electrophoresis was a sensitive and cost-effective method of SCD screening. 19 However, point of care devices may be used in place of electrophoresis if available at an affordable price. It is further observed that following up on screening results is easy and requires minimum effort to bring the patients to care because the screening programme is community-based through health workers.
Systematic screening for SCD is crucial in management of the condition. Screening newborns and children, with follow-up care utilising appropriate antibiotics and vaccines, drastically reduces morbidity and mortality during infancy and childhood.20,21 In developed countries like the US, screening typically occurs prenatally or at birth (newborn screening). However, symptomatic people who were not screened at birth may get diagnosed later. 22 Although there is no established screening programme as part of SCD management in India, a few attempts to develop this have been made.23–26 Elsewhere, 22 such programmes demonstrate high value in their utility for policy and practice.
A screening programme of the kind described here could be quickly scaled up to cover all SCD-endemic districts in the country. It is feasible to implement with local resources at the PHC level without much investment or delay. As discussed above, this model involves community and local health workers who have high credibility in the community. These health workers are involved in other aspects of SCD care like referral, transport to PHC, psycho-social care, etc., whereas many screening programmes happen in isolation. Also, this programme covers people of all ages, considering the fact that no systematic screening has been held in these tribal-dominated areas, and many people, including children, adolescents and adults, are surviving with SCD. The programme is planned to continue as part of the overall SCD care management, and it finds new SCD cases and includes them in the care system as a continuous process. Further, community-based SCD screening programmes effectively improve the SCD status of people and thereby increase chances of care and counselling. 27 Currently, SCD care seldom happens in tribal areas. There is no routine supply of hydroxyurea to public health facilities, and doctors are not oriented to use it. In the present model, the supply of hydroxyurea and other medicines was ensured, and doctors at PHCs/CHCs were primed to treat SCD patients, including monitoring the hydroxyurea therapy. All patients received the treatment at their PHC/CHC.
The overall limitation of this model is the subjective assessment of symptomatic diagnosis by ASHAs. However, using a structured checklist and thorough training minimises the subjectivity in identifying suspected SCD cases. Also, some people moved to the next stage of screening, i.e. solubility test, without depending on the ASHA's assessment. The solubility test has a limitation in that there is the possibility of false negatives among infants. 11 Hence, all infants may be diagnosed directly through electrophoresis in PHCs/CHCs. This model fails to detect other haemoglobinopathies and haemoglobin variants, which are uncommon in most study districts, except in the Udalguri district, where Hb E is found. By addressing these limitations, this model of screening can be implemented in low-resource settings like the tribal areas of India. Also, it appears to be cost-effective, though a systematic cost analysis has not been carried out.
Conclusions
This study demonstrates the feasibility of establishing a population-based screening programme in the primary health care system of Indian tribal areas. It is relatively inexpensive and easy to implement, to cover all ages. Screening further leads to providing SCD patients with treatment and care. Hence, it can be part of the proposed national SCD/haemoglobinopathies control programme.
Supplemental Material
sj-docx-1-msc-10.1177_09691413221123131 - Supplemental material for Feasibility of population-based screening of sickle cell disease through the primary health care system in tribal areas of India
Supplemental material, sj-docx-1-msc-10.1177_09691413221123131 for Feasibility of population-based screening of sickle cell disease through the primary health care system in tribal areas of India by Bontha V. Babu, Yogita Sharma, Parikipandla Sridevi, Shaily B. Surti, Manoranjan Ranjit, Deepa Bhat, Jatin Sarmah and Godi Sudhakar in Journal of Medical Screening
Footnotes
Acknowledgements
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Indian Council of Medical Research, (grant number NTF/SCD/2019/SBHSR)
Ethics approval
The study protocol was approved by the institutional ethics committees of Indira Gandhi National Tribal University, Parul University, Indian Council of Medical Research-Regional Medical Research Centre, JSS Medical College, Bodoland University and Andhra University.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.