
Abstract
Objective
To determine the rate of lymphoproliferative disease (LPD) in women undergoing routine breast cancer screening (BCS). BCS can reveal pathologies other than carcinoma that involve the breast and lymph tissue. The few studies that have described cases in which BCS led to the diagnosis of LPD were based on small series and focused on imaging rather than clinical characteristics.
Setting and Methods
A multi-center retrospective study in Israel, investigating LPD rate and characteristics among women diagnosed with LPD via BCS.
Results
Thirty-four patients out of 14,400 consecutive women undergoing BCS at Tel Aviv Sourasky Medical Center during the study period were diagnosed with LPD, suggesting a diagnosis rate of 0.24%. The enlarged cohort (n = 45), including 11 patients that were retrieved from the databases of three other centers, demonstrates a predominant histological diagnosis of non-aggressive LPD (n = 33). Thirty-four (76%) had a suspicious axillary lymph node, and 11 had a breast lesion. The median maximal lesion size was 1.95 cm (range 0.8–6.5). Disease was localized in 60% of patients (stage 1 and 1E). Univariate analysis revealed that lymphocyte count was inversely associated with aggressive histology. At median follow-up of 39 months, all but three patients were alive. These three had been diagnosed with non-aggressive LPD which had never been treated and died from unrelated causes.
Conclusions
The LPD detection rate via BCS was 2.36 per 1000 screens. The majority of LPDs were non-aggressive. Nearly a third were aggressive, most detected at an early stage, and the clinical outcome was generally favorable.
Introduction
The main objective of breast cancer screening (BCS) is to reduce breast cancer mortality through early detection, with mammography as the primary screening tool.1–3 The Israeli national breast cancer screening program invites all women from age 50 to 74 for an annual bi-mammography. The Israeli Health Ministry recommended as of February 2019 to include also in the program women aged between 45 and 49 wishing to undergo screening. Breast imaging can reveal pathologies other than carcinoma that involve the breast and lymph tissue, including lymphoproliferative disease (LPD). LPD cases usually exhibit imaging phenotypes that overlap with those of primary breast carcinoma.4, 5
The few published studies that have described cases in which BCS led to the diagnosis of LPD were based on small series and focused primarily on imaging rather than clinical characteristics6–9 The aim of this study was to determine the rate of LPD in women undergoing routine screening mammography, to describe the characteristics of these patients, the histological subtypes and factors that predict aggressive versus non-aggressive histology.
Methods
This is a retrospective study, which was conducted in four medical centers throughout Israel.
First, in order to assess the rate of incidental detection of LPD in women undergoing BCS, all women undergoing mammography at the Tel Aviv Sourasky Medical Center (TASMC) from January 1, 2010 to September 1, 2021 were reviewed. Cross-matching between BCS records with any diagnosis of LPD (using data from hematology and pathology departments) identified all cases that were reported in both data sets.
The Center for Screening and Preventive Medicine at the TASMC follows the Israeli national guidelines as described in the Introduction, and has further expanded its screening criteria to include women over the age of 40. BCS includes an annual bi-mammography and clinical breast examination. A mammogram with Breast Imaging-Reporting and Data System (BI-RADS) 10 classification 3–4 indicates further screening with breast ultrasound. Histological diagnosis was performed using a core needle biopsy.
With the aim of enlarging the patients’ cohort, 11 additional patients were retrieved from the lymphoma data bases of three other centers: Assuta Ashdod Hospital, Shamir Medical Center and Wolfson Medical Center (from September 1, 2019 to September 1, 2021).
Data were extracted from electronic medical charts and included patients’ demographics, clinical characteristics, imaging factors including the size of pathological lesion, pathological appearance, BI-RADS, 10 treatment if provided, responses to treatment, and survival.
The study was approved by the Institutional Review Boards of the participating centers, and informed consent was waived.
Statistical analysis
Continuous variables were described as medians and ranges. Categorical data were described using contingency tables, including frequency and percent. Categorical variables were compared with Fisher’s exact test or the χ2 test Continuous variables were analyzed with the Mann-Whitney test for independent samples. Univariate Cox regression was used to study the crude association between studied predictors for aggressive versus non-aggressive disease. SPSS software (IBM SPSS Statistics for Windows, version 25, IBM Corp., Armonk, NY, USA, 2017) was used for all statistical analyzes.
Results
Rate of diagnosis of LPD during BCS
In the TASMC cohort, 34 patients were identified as having LPD (0.24%) among 14,400 BCS records, i.e. 2.36 per 1000 screens. The rate of LPD involving only the axilla was 0.16% (23 patients). The rate of LPD diagnosed via BCS in the population without a history of LPD was 0.19%, i.e. 1.87 per 1000 screens.
Patient and imaging characteristics
Forty-five patients were included in this analysis: 34 from the TASMC database and 11 from the three additional centers in Israel (Table 1). Median age was 69 (range 36–87) years. Most of the women underwent BCS as a routine exam (75%), and the others for breast malignancy follow-up (15%), or due to a family history of breast malignancy (10%). A suspicious lesion was detected on mammography only in 35 of the 45 patients (78%) and 10 patients needed further evaluation by ultrasound (n = 9) or magnetic resonance imaging (n = 1) (Figure 1).
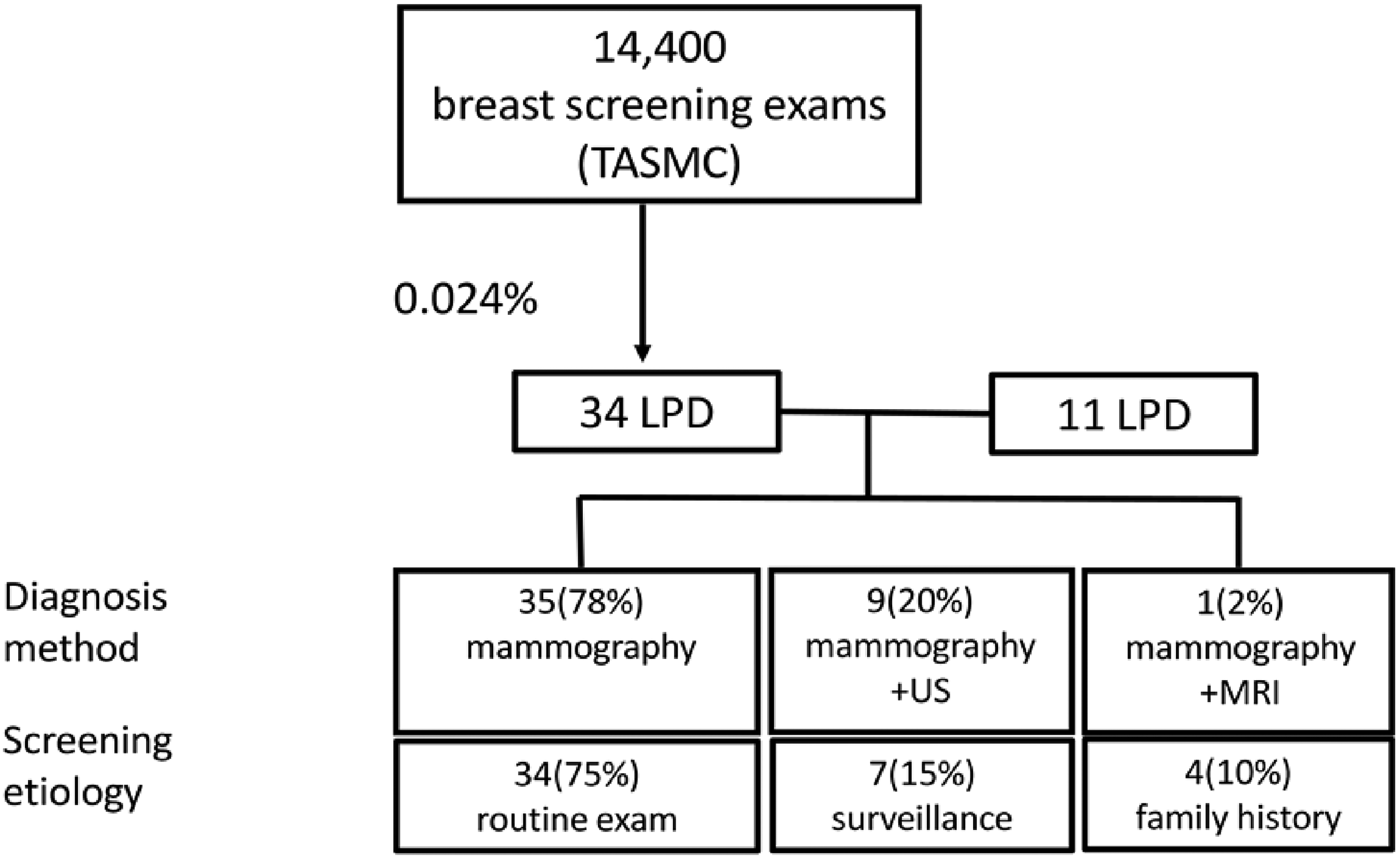
Study flowchart. TASMC: Tel Aviv Sourasky Medical Center; LPD: Lymphoproliferative disease; US, ultrasound; MRI, magnetic resonance imaging.
Patients and disease characteristics (n = 45).
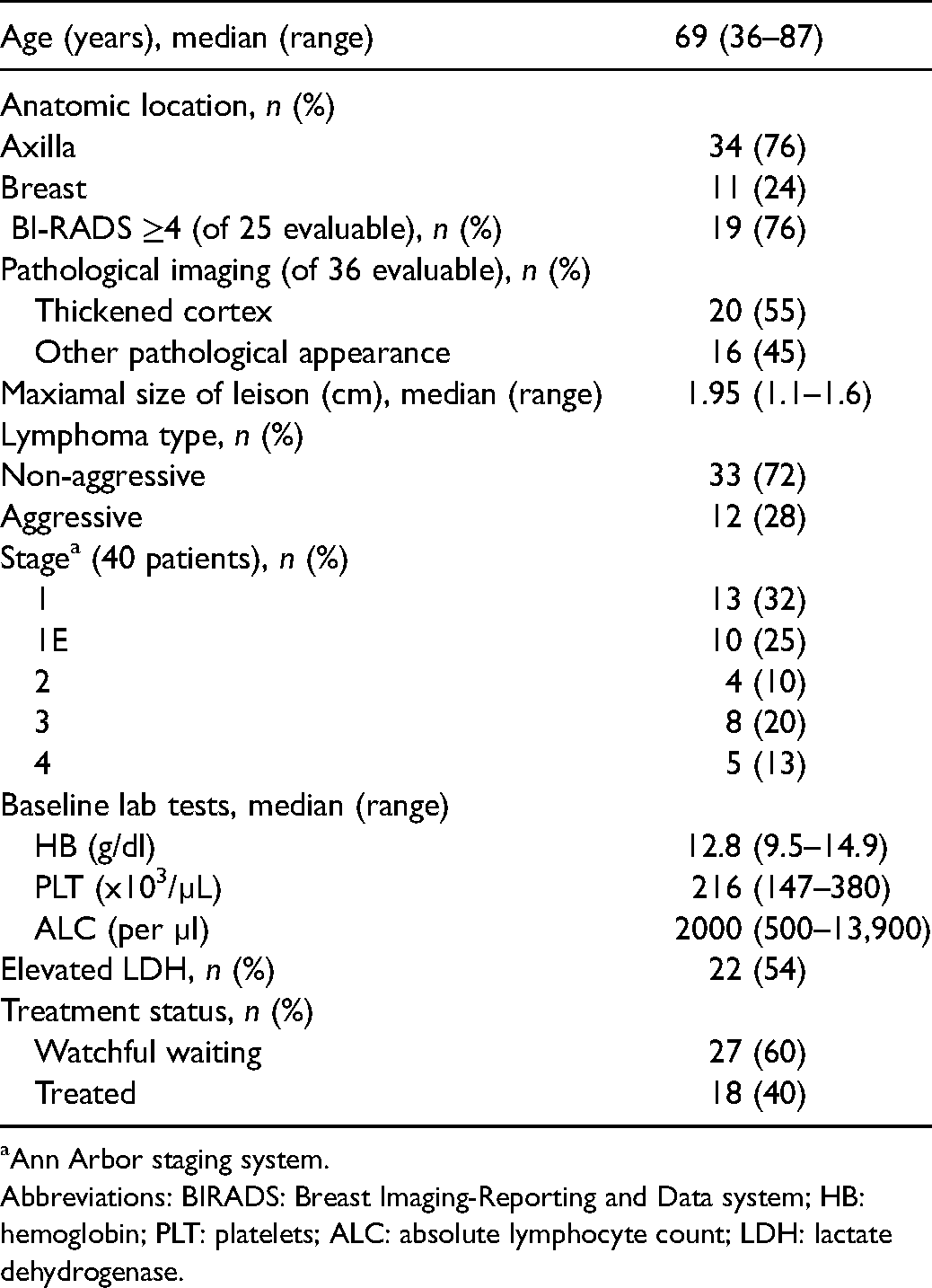
Ann Arbor staging system.
Abbreviations: BIRADS: Breast Imaging-Reporting and Data system; HB: hemoglobin; PLT: platelets; ALC: absolute lymphocyte count; LDH: lactate dehydrogenase.
Thirty-four patients (76%) had a suspicious axillary lymph node, while 11 (24%) presented with a breast lesion (see examples in Figures 2 and 3). All the lesions appeared pathological, with a thick cortex being observed in 20/36 (55%). The lesion was graded ≥4 (BI-RADS) in 19 of the 25 evaluable patients (76%). The median maximal size of the lesion was 1.95 cm (range 0.8–6.5) cm. Eight patients (18.6%) had a known history of LPD (all of them without known nodal involvement), and six of these had chronic lymphocytic leukemia (CLL).
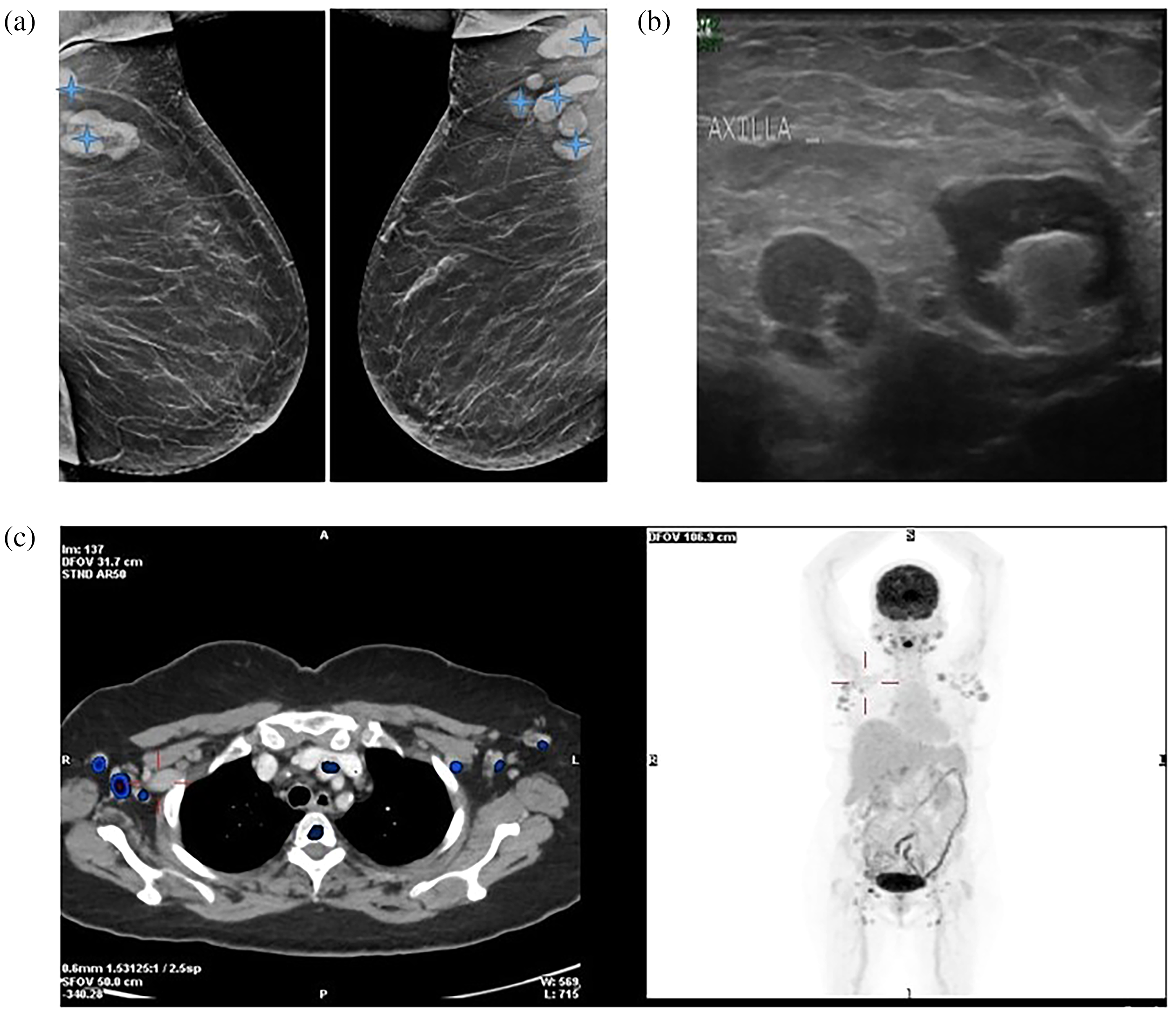
Example of pathological screening result: mammography, breast ultrasound and positron emission tomography (PET) findings. A 69-year-old woman underwent screening mammography, revealing normal breasts and bilateral axillary lymphadenopathy (a, stars). Ultrasound showed bilateral pathological axillary lymphadenopathy with thickened cortex and loss of fatty ileus (b). Pathology revealed diffuse large B cell lymphoma. PET-CT (computed tomography) demonstrated axillary lymphadenopathy with F-fluorodeoxyglucose uptake (c).
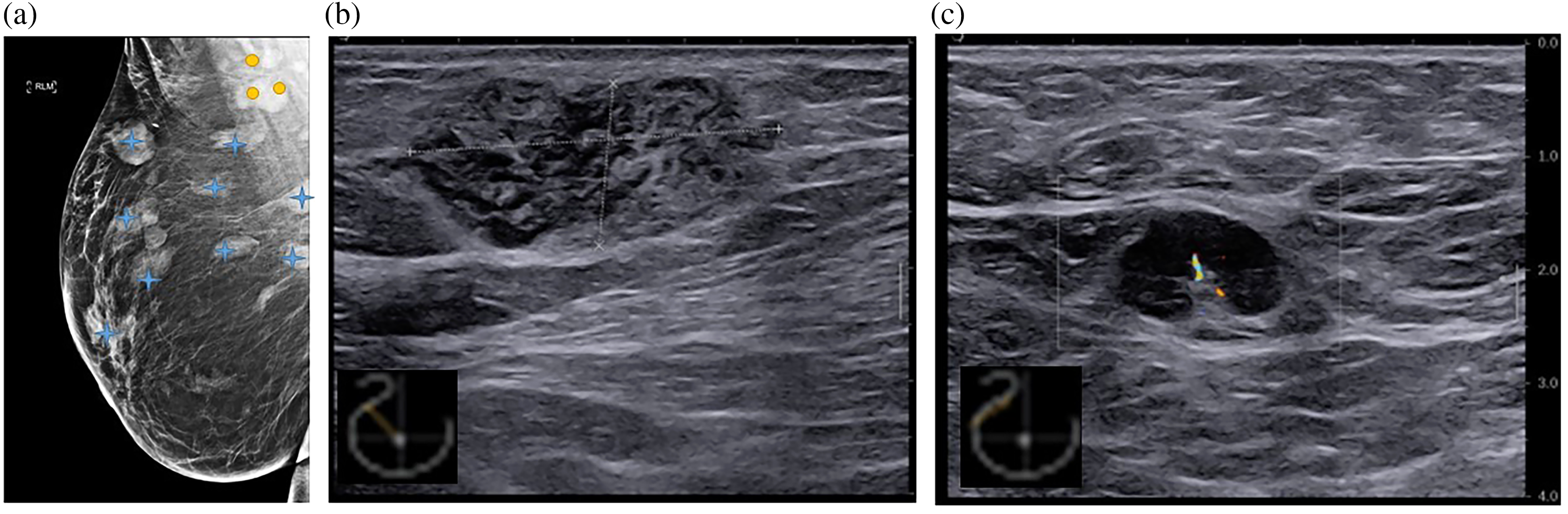
Example of pathological screening result: mammography and breast ultrasound findings. Screening mammography (a) of 78-year-old woman demonstrated multiple breast lesions (stars) and lymphadenopathy (circles). A breast ultrasound revealed a mass of 3.29 × 1.44 cm (b) and right axillary lymphadenopathy with thickened cortex and loss of fatty ileus (c). Pathology of breast mass: Marginal zone lymphoma.
The baseline median hemoglobin level was 12.8 g/dl (range 9.5–14.9), median platelet count was 216 × 103/µL (range 147–380), and median absolute lymphocyte count (ALC) was 2000/µl (range 500–13,900). Eleven patients (24%) had elevated lactate dehydrogenase levels.
LPD characteristics
Histopathological studies revealed that 33 patients (73.3%) had a non-aggressive LPD: 14 (31%) patients had CLL, nine (20%) had marginal zone lymphoma, eight (18%) had follicular lymphoma, and two (4%) had nodular lymphocyte-predominant Hodgkin lymphoma. Twelve patients (26.7%) were diagnosed with aggressive lymphoma (none of them had known history of lymphoma): nine of 45 patients (20%) had diffuse large B-cell lymphomas, two (4%) had mantle cell lymphoma and one (2%) had classic Hodgkin lymphoma.
Data on disease stage at diagnosis were available for 40 patients: 10 patients with lymphoma involving the breast were diagnosed at stage IE. Thirteen patients had stage I disease limited to the axilla on one side, four patients had stage II disease, seven patients had stage III disease, and five patients had stage IV disease according to the Ann Arbor classification.
Within a median follow up period of 39 months (range 13–90) since diagnosis, 18 patients (40%) - 6/33 with non-aggressive and 12/12 with aggressive lymphoma - required therapy: four patients were treated with radiotherapy, 14 were treated with chemo-immunotherapy. Eight achieved complete response, six achieved partial response and four achieved stable disease. The remaining 27 patients, all with a non-aggressive lymphoma, were managed with a watchful waiting approach.
At the end of follow up, all but three patients were alive. These three patients had non-aggressive lymphomas that had never been treated, and they died of unrelated causes. Univariate analysis to evaluate predictors for aggressive histology, including stage of disease, size of lymph node, patient's age, hemoglobin count, platelet count, ALC and elevated lactate dehydrogenase at diagnosis, revealed that only ALC was associated with aggressive histology. The median ALC in non-aggressive lymphomas was 3.1 (interquartile range [IQR] 1.1–6.7) versus 1.45 (IQR 1.3–2.1) in patients with aggressive lymphomas (p = 0.041).
Discussion
The findings of our study demonstrate a rate of 0.24% (2.36 per 1000 screens) for LPD detection by BCS, a higher rate than most previous studies. It can be partially explained by the fact that our series reports detection of LPD in both the axilla and breast rather than just the axilla as in previous studies. Indeed, a 0.16% rate of axillary LPD in our cohort is consistent with the rate of 0.14% reported previously by Schwab et al. 9 who evaluated patients whose BCS showed suspicious lymph nodes in the axilla with normal breast studies.
In contrast, three other publications reported lower rates of diagnosed axillary LPD, detected on BCS: Welsh et al. 6 found a rate of 0.048%, Shetty et al. 8 reported a rate of 0.028%, and Patel et al. 7 found a rate of 0.004%. It is possible that the higher incidence of LPD detected by BCS observed in our study can be attributed to the higher incidence of LPD among the Israeli population. 11
Compared to our rate of 2.36 LPD cases diagnosed per 1000 screens, breast cancer detection rates via BCS range between 4.6 and 9.4 12
The majority of patients (76%) in our series had axillary lymph node involvement by LPD, compared to 24% with breast involvement. This can be explained by the fact that breast involvement by lymphoma is rare, accounting for approximately 0.5% of malignant breast neoplasms, 1% of all non-Hodgkin lymphomas, and 2% of all extra-nodal lymphomas.13,14
The majority of patients detected with LPD during BCS in our study had a non-aggressive B cell lymphoma with only about a third were diagnosed with an aggressive lymphoma. The only predictor for aggressive pathology was a lower ALC at diagnosis, most probably reflecting the fact that most of the patients with high ALC were diagnosed as having CLL or marginal zone lymphoma.
To the best of our knowledge, this is the first report to provide detailed information about LPD histology subtypes and clinical characteristics in the setting of incidental finding in BCS. Our study has several limitations: this is a retrospective study and the sample size is small. We included eight patients (8/45, 17.8%) with a known history of LPD. All of these patients presented with leukemic stage, without known nodal involvement. They were diagnosed with nodal disease while having a routine breast screening (performed irrespective of their LPD). However, the inclusion of patients with known LPD may have introduced a bias into our analysis. Therefore, we calculated the rate of LPD diagnosed via BCS in the population without a history of LPD: 0.19%, or 1.87 per 1000 screens.
In conclusion, BCS led to the diagnosis of LPD at a rate of 0.24%. Most LPDs were non-aggressive; however, nearly a third were aggressive, most of them detected in early stage and their clinical outcome is generally favorable. Additional reports from other institutions with a more homogeneous population are warranted to validate our results.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.