
Abstract
Objectives
To compare attendance, recall and cancer detection as well as histopathological tumor characteristics among women attending BreastScreen Norway after a reminder versus an ordinary invitation.
Setting
This study was conducted on data from a population-based screening program inviting women aged 50–69 to biennial two-view mammography.
Methods
We used de-identified data from 883,020 women invited to BreastScreen Norway, 2004–2020, to analyze invitations, participation, recalls, biopsies, cancer detection, and histopathological tumor characteristics. All results were stratified by reminders and ordinary invitations. Early screening outcomes after reminders versus ordinary invitations were compared using bivariate tests and multivariable logistic regression.
Results
Reminders increased overall participation rate by 5.0%. The recall rate was 4.3% for reminded women and 3.3% for the ordinary invited. For reminded women, the rate of screen-detected cancer was 7.3 per 1000 screening examinations compared to 5.8 per 1000 for ordinary attenders. The interval cancer rates were 1.9 and 1.7 per 1000 for reminded and ordinary invited women, respectively. Median tumor diameter was 14 mm (interquartile range (IQR): 10–16) for screen-detected cancers (SDC) among reminded women and 13 mm (IQR: 10–16) for ordinary invited. A higher percentage of histological grade III cancers was observed among the reminded: 25.2% versus 21.7% for the ordinary invited. We also found a higher proportion of lymph node positive cases in those reminded: 23.6% versus 20.9%.
Conclusions
Postponing screening examinations affects early screening outcomes, including cancer detection and histopathological tumor characteristics. Women should be encouraged to attend screening at regularly intervals to avoid delays in diagnosis.
Introduction
High levels of participation are crucial to achieve a desired mortality reduction from breast cancer in population-based screening programs. 1 The European Commission Initiative on Breast Cancer (ECIBC) recommends using a letter for inviting asymptomatic women aged 50 to 69 with an average risk of breast cancer to attend screening. 2 Further, they suggest this letter should include a fixed appointment and a general practitioner's signature, and that it should ideally be followed by a phone call or written reminder.
Factors affecting women's response to invitations for mammographic screening have been addressed by several studies. In a recent study from Sweden, lower odds of participation were observed among women living without a partner, non-Nordic women born in Sweden, women with low-income, living on social benefits or not owning their own home, and among those with low levels of education. 3 This is supported by studies from BreastScreen Norway.4,5 Further, a systematic review has shown that pain or other discomfort during mammography could affect re-attendance in mammographic screening. 6
Other studies have explored interventions in non-participants to increase participation. Second reminding letters and contacts by phone are both shown to increase attendance.7,8 In a study from Ireland, the participation rate increased from 55% to 85% in response to a postal reminder, 9 while a Norwegian study found an increase from 71% to 76%. 8 Studies from the UK have reported that a reminding letter including a fixed appointment results in higher participation than an open invitation.10,11 However, we have not been able to identify studies describing reasons why women do not attend screening after an ordinary invitation but rather as a response to a reminder. Further, as far as we are aware, there is limited evidence on potential consequences of attendance after a reminder on the outcomes of screening, such as recall and cancer detection rates.8,9
BreastScreen Norway invites women aged 50–69 years for biennial mammographic screening by personal postal or digital letters with pre-scheduled fixed appointments. 12 Non-attenders receive a reminder 4–6 weeks after the original scheduled appointment. This reminder is an open invitation suggesting women to contact the local screening unit to make an appointment.
In this study, we took advantage of the large dataset collected by BreastScreen Norway where the screening outcomes can be matched with the individual screening history of every participating woman. We compared attendance, recall and cancer detection rates, as well as histopathological tumor characteristics among those who attended the program after a reminder versus an ordinary invitation.
Materials and methods
We received de-identified data about women invited to BreastScreen Norway, 2004–2020, from the Cancer Registry of Norway, which administers the program and collects information about invitations and screening examinations, recalls and diagnostic assessments, treatment, and surveillance. The data protection officer for research at Oslo University Hospital approved the study (2020/12,601).
BreastScreen Norway is a population-based screening program started in 1996 inviting all women aged 50–69 to biennial two-view mammography. 12 During the first 20 years, the average participation rate was 75% with a recall rate of 3.8%. The rate of screen-detected cancer was 5.9 per 1000 screening examinations and the interval cancer rate was 1.8 per 1000 examinations. 12
In this study, we included examinations performed with digital mammography. BreastScreen Norway implemented digital mammography stepwise during the period between 2004 and 2011. 12 This means that the start of the study period varied between breast centers. All screening invitations among women without a previous history of breast cancer until 2021 were included, resulting in 3,460,976 ordinary invitations sent to 883,020 women.
Ordinary invitations and reminders
All women targeted by BreastScreen Norway receive an ordinary invitation, unless they have opted out of the program. An ordinary invitation includes a scheduled time and place for the examination and a leaflet about the screening procedure, and potential benefits and harms of mammographic screening. The invitations are sent to the women about three weeks prior to the scheduled appointment. A reminder is sent to non-participating women 4–6 weeks after the originally scheduled appointment as an open invitation letter encouraging the woman to call her local screening unit to schedule a new appointment. Ordinary invitations and reminders are sent electronically (digital mail) or by postal service. Digital mail was made available for BreastScreen Norway in 2016 and is used for invitations to the program only if activated by the invitee.
Variables of interest
In addition to invitation type (ordinary invitation and reminder), screening history, recall, biopsies, cancer detection and histopathological tumor characteristics were included in the analysis.
The women's screening history was stratified into prevalent and subsequent screening examinations. Prevalent is the first screening examination in BreastScreen Norway, while all following examinations were defined as subsequent. The attendance rate after an ordinary invitation was calculated as the number of screening examinations following ordinary invitations divided by the number of ordinary invitations sent. The attendance rate after reminders was defined as the number of examinations following reminders divided by the number of reminders sent. The overall attendance rate was calculated as the number of all screening examinations divided by the number of ordinary invitations.
Recall rate was defined as the number of screening examinations prompting further assessment due to abnormal mammographic findings or symptoms reported by the women at time of screening, divided by all screening examinations. Biopsy rate was calculated as number of biopsies divided by screening examinations.
Screen-detected cancer was defined as breast cancer diagnosed after recall for assessment and within 6 months of the screening examination. We included ductal carcinoma in situ and invasive cancer in our definition of breast cancer. Interval cancer was defined as breast cancer diagnosed within 24 months of a negative screening result or within 6–24 months of a false positive screening examination. Positive predictive values were estimated as the percentage of screen-detected cancer among all recalled women (PPV-1), and among all biopsied women (PPV-3).
For invasive cancers, we presented histological type, tumor diameter, grade, lymph node status, and molecular subtypes by immunohistochemical (IHC) surrogate markers. Using estrogen (ER), progesterone (PR) and human epidermal growth factor receptor 2 (Her2) status, we divided the tumors based on a modification of the St. Gallen guidelines (without Ki67) into Luminal A-like, Luminal B-like (Her2-), Luminal B-like (Her2+), Her2+ (non-luminal) and triple negative. 13
To estimate the delay caused by not attending the ordinary invitation, we calculated the time (days) from originally scheduled appointment to screening examination after a reminder.
Statistical analysis
Participation, recall, biopsy, and cancer detection rates were stratified by invitation type. For categorical variables, we presented frequencies and proportions. Age was presented using mean and standard deviation (SD), while time and tumor diameter was presented using median and interquartile range (IQR) due to a non-normal distribution. Differences in recall, biopsy, screen-detected cancer, interval cancer, PPV-1, PPV-3, and tumor characteristics for attendance after ordinary invitations versus reminders were analyzed with bivariate tests. In addition, odds of recall, biopsy and screen-detected cancer were adjusted for time between scheduled appointment given at ordinary invitation and attendance in multivariable logistic regression models. Results were presented as unadjusted and adjusted odds ratios (OR) with 95% confidence intervals (CI). We used STATA version 17.0 for Windows (StataCorp, TX, USA) for all statistical analyzes.
Results
Participation was 70.4% after ordinary invitations and 17.3% after reminders, which resulted in an increase of 5.0% in overall participation after reminders and an overall participation rate of 75.4% among women invited to BreastScreen Norway, 2004–2020 (Figure 1). The participation rate after reminders as well as the overall attendance rate was highest for those receiving digital invitations (Figure 2).
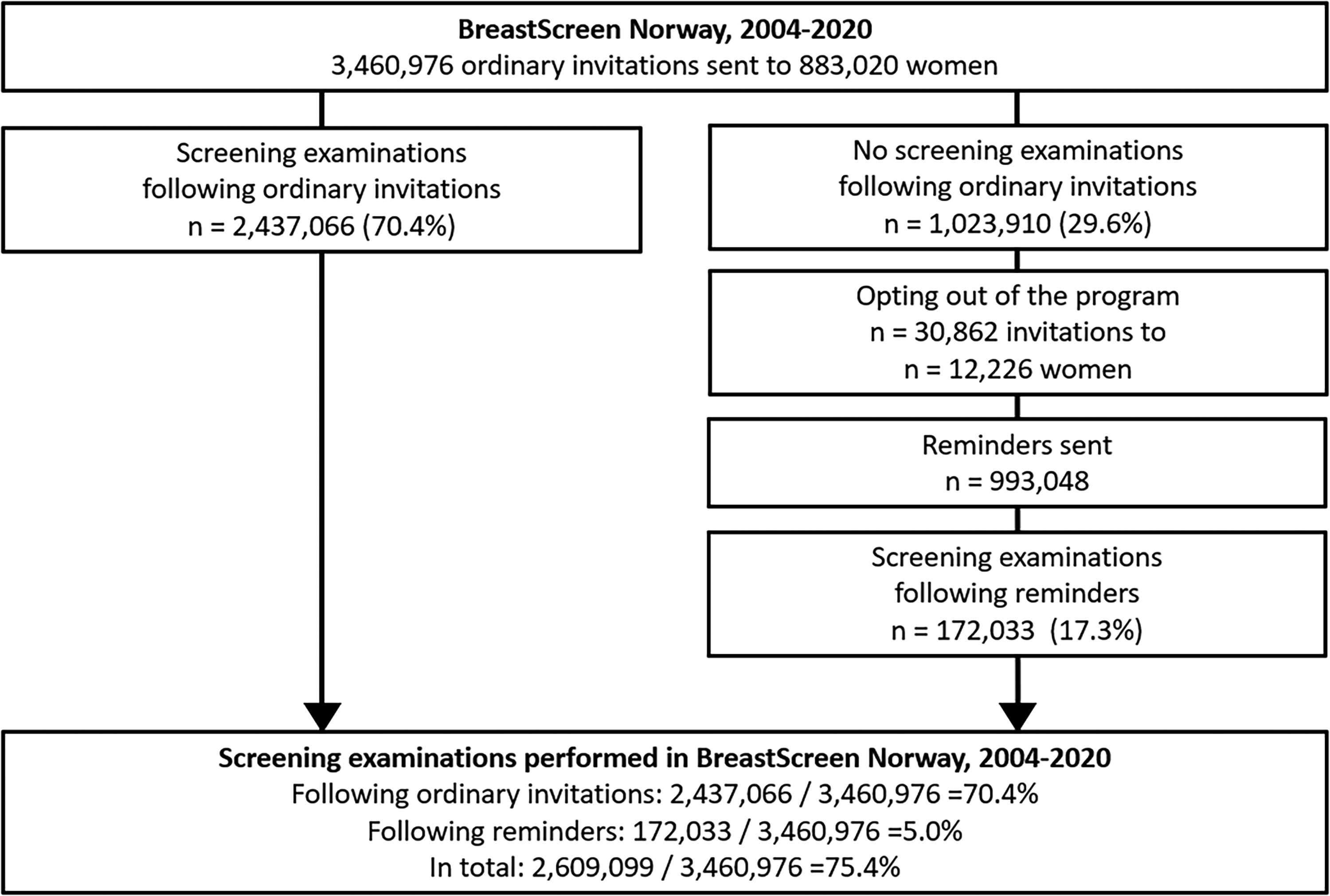
Flowchart of the study sample. Number of screening examinations following ordinary invitations and reminders for digital mammographic screening, sent to women with no history of breast cancer targeted by BreastScreen Norway during the period from 2004 to 2020.
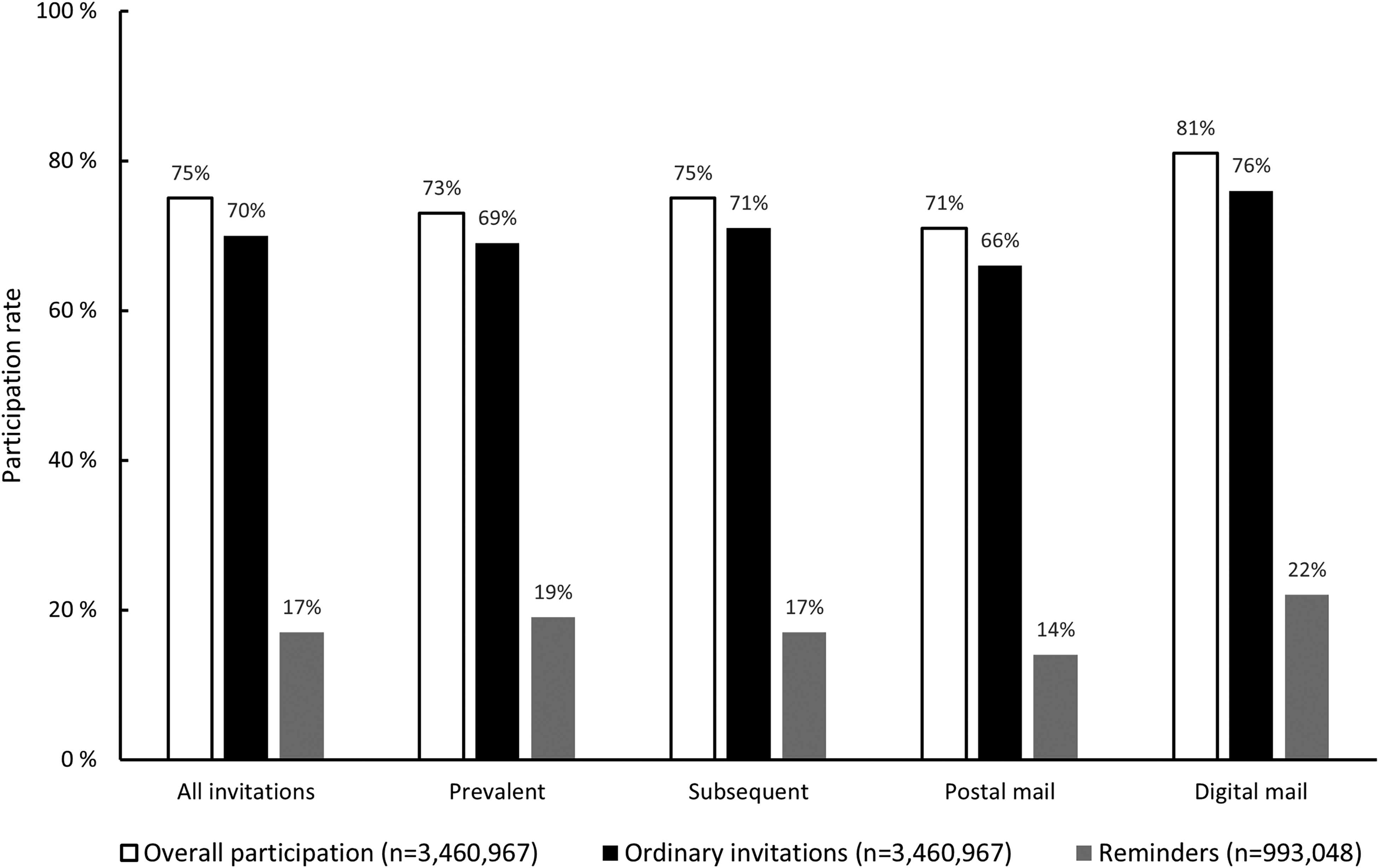
Participation after prevalent, subsequent, postal, and digital invitations stratified by overall participation and participation after ordinary invitations and reminders.
Women attending after ordinary invitations and after reminders both had a mean age of 59 years (SD = 6) at screening. Median time from ordinary scheduled appointment to participation after a reminder was 103 days (IQR: 73–154). For prevalently screened women the median was 111 days (IQR: 76–175 days) and for subsequently screened, 101 days (IQR: 72–150 days).
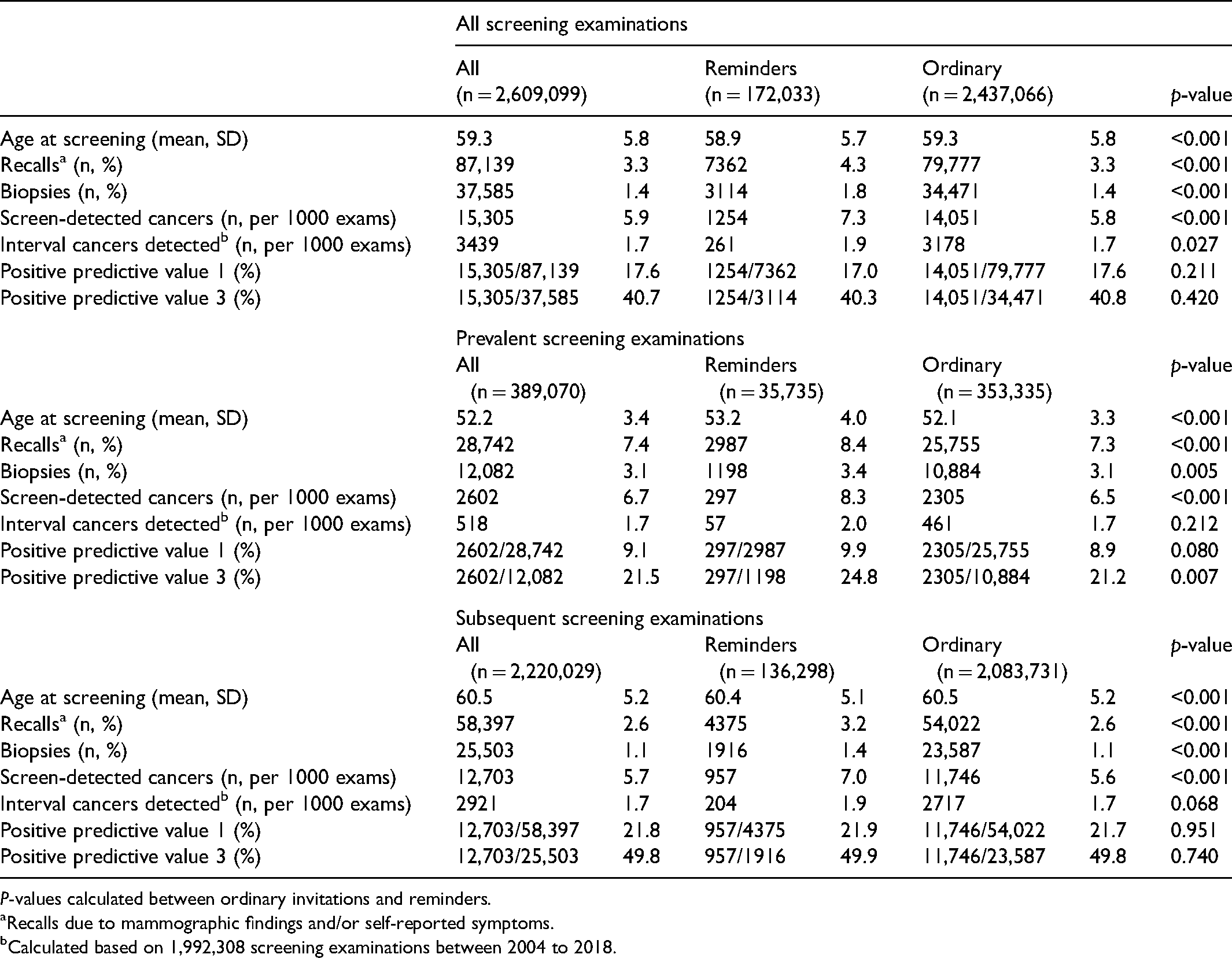
A total of 4.3% of examinations following a reminder and 3.3% of those following an ordinary invitation resulted in a recall for further assessment (Table 1). Recall rate due to self-reported symptoms was 0.55% among women participating after a reminder and 0.25% after an ordinary invitation (p < 0.001).
Age at screening and early screening outcomes stratified by ordinary invitations and reminders for all screening examinations, prevalent and subsequent examinations.
P-values calculated between ordinary invitations and reminders.
Recalls due to mammographic findings and/or self-reported symptoms.
Calculated based on 1,992,308 screening examinations between 2004 to 2018.
The rate of screen-detected cancers was 7.3 per 1000 examinations after reminders compared to 5.8 after ordinary invitations (Table 1). A higher rate of screen-detected cancer was also observed for examinations after reminders when stratified by screening history. The interval cancer rate after reminders was 1.9 per 1000 examinations and 1.7 after ordinary invitations. There were no statistically significant differences in the interval cancer rates when stratified by prevalent and subsequent examinations.
Using attendance after an ordinary invitation as reference and adjusting for days between scheduled appointment and attendance, the OR for recall was 1.09 (95% CI: 1.05–1.14) and the OR for screen-detected cancer was 1.03 (95% CI: 0.95–1.12) for women attending after a reminder (Table 2).
Odds ratio (OR) and 95% confidence interval (CI), unadjusted and adjusted, for recall, biopsy and screen-detected cancers (SDC) among women attending mammographic screening after a reminder.
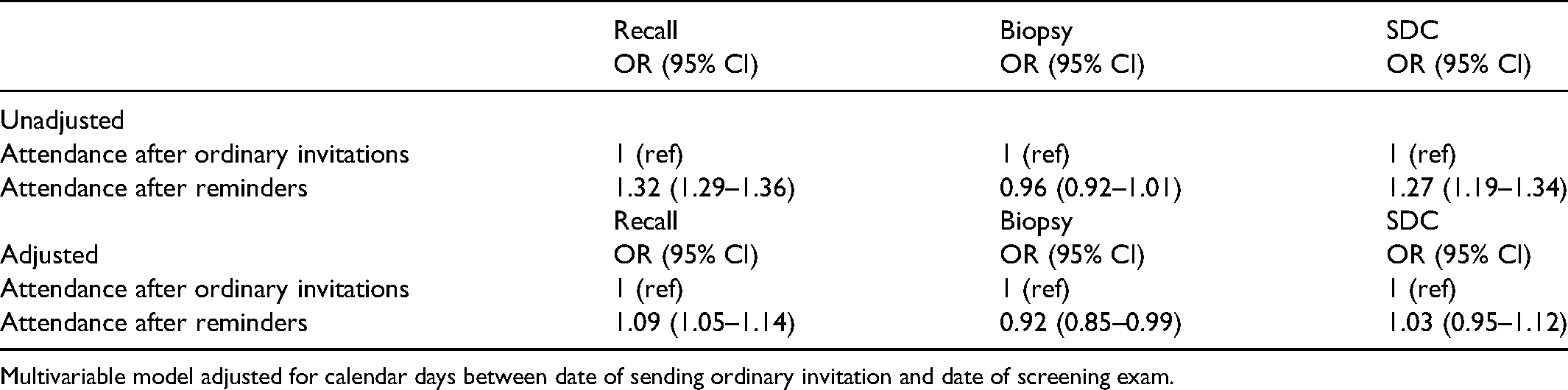
Multivariable model adjusted for calendar days between date of sending ordinary invitation and date of screening exam.
Median tumor diameter for invasive screen-detected tumors after a reminder was 14 mm (IQR: 9–20), compared to 13 mm (IQR: 9–19) for those detected after an ordinary invitation (Table 3). Among cancers detected after a reminder the proportion of histologic grade 3 tumors was 25.2% (258/1045) while the corresponding proportion detected after ordinary invitations was 21.7% (2438/11,416). The proportion of lymph node positive tumors was 23.6% (239/1045) and 20.9% (2328/11,416) among cancers detected after reminders and ordinary invitations, respectively.
Tumor characteristics of screen-detected cancers among screened women, stratified by attendance after ordinary invitations and attendance after reminders.
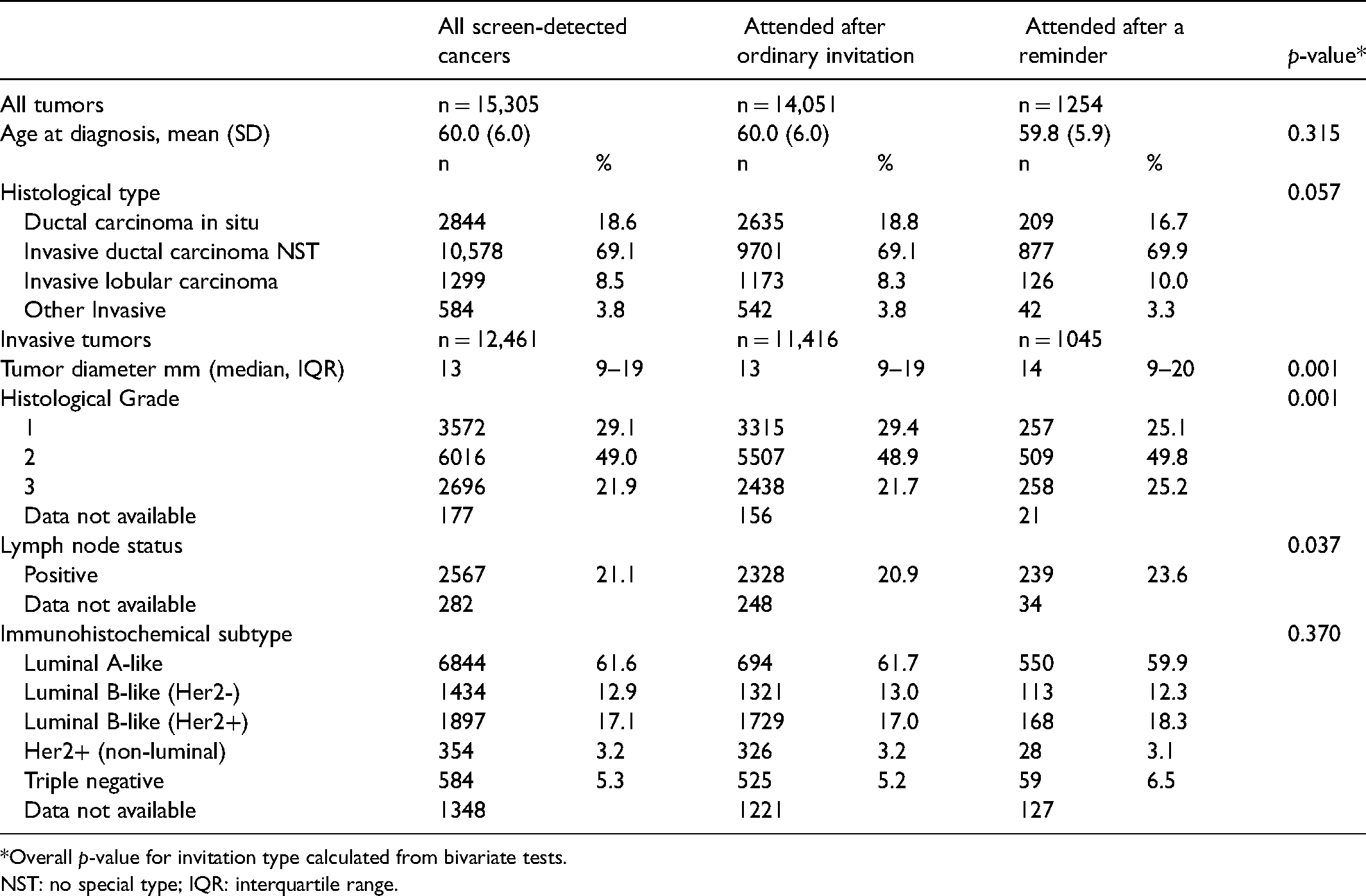
*Overall p-value for invitation type calculated from bivariate tests.
NST: no special type; IQR: interquartile range.
Discussion
We found higher rates of recall, screen-detected cancer and interval cancer among women who participated in BreastScreen Norway after a reminder compared to an ordinary invitation. Screen-detected cancers among reminded attendees had larger histopathological diameter and the percentage of histological grade III cancers was higher. We also showed a higher proportion of lymph node positive screen-detected cases in those reminded. After adjustment for time between the ordinary scheduled appointment and actual attendance, only recall rate differed between the two groups.
Our findings differ from an Irish study where they found lower recall rates among those who attended after a second reminder versus an ordinary invitation while no impact on the cancer detection rates was observed. 9 The proportion of women who received a reminder in Ireland was higher compared to our study and the postal reminder included a pre-booked appointment. In Norway, only the ordinary invitation includes a scheduled appointment while the reminders advise the women to contact the local breast unit to schedule a new appointment. Concerning recall and cancer detection rates, our findings are in keeping with a previous study from BreastScreen Norway. 8 However, the study population was smaller and results on histopathological tumor characteristics were not reported.
Results from the unadjusted analyzes revealed that delay of screening examination influenced cancer detection and histopathological tumor characteristics. Women who attended screening after a reminder had their screening examination delayed by a median of 100 days, during which a potential tumor might grow. With average volume doubling time for breast cancers of approximately 180 days, the observed increase in tumor diameter is within expectations due to the prolonged screening interval. 14 Growth might also explain a shift towards higher-grade cancers when areas that are more aggressive overgrow the more differentiated slow-growing parts of the tumor.15,16 Assessment of histological grade is still in the molecular era an important determinant of breast cancer prognostication. 17
With the high stress put on health care systems due to the ongoing COVID-19 pandemic, mammography and mammographic screening have been postponed in several countries.18,19 Our study illustrates the negative effects of a prolonged screening interval and underlines the importance of avoiding delays in population-based screening.
Time alone cannot explain the higher recall rates among the women who attend after a reminder. We assume some type of bias within this group. A feeling of unease in the breast might motivate the women to attend after the reminder. 8 They might also have concerns due to known risk factors such as family history of breast cancer or use of hormonal replacement therapy. Despite the concerns or uneasiness, they might miss the ordinary invitation for trivial reasons such as not being aware of the letter, forgotten appointment, busy schedule, or illness. The first ordinary invitation could also make the women more breast-aware helping them to recognize a lump or other changes or symptoms. The action needed to book an appointment in response to the reminder might also select more motivated women.
Another finding supporting the idea of bias is the higher proportion of women with self-reported symptoms among reminded attendees. This contributes only to a small number of cancers but is likely to be somewhat underreported because women with symptoms also could have a positive mammography, which overrules self-reported symptoms in the BreastScreen Norway program. A previous Norwegian study showed the risk of breast cancer to be 10 times higher in women with self-reported lumps compared to asymptomatic women. 20 The tumors diagnosed were also larger with less favorable histopathological characteristics and interval cancers were more frequent.
A major strength of our study was the large study sample in which the outcome of screening could be linked with a detailed screening history for the individual woman. Still, we do not know the reasons for not attending after the ordinary invitation. Neither do we know what motivated them to schedule an appointment after receiving the reminder. Lifestyle factors such as physical activity, body mass index, alcohol consumption and smoking, and family history of breast cancer may influence breast cancer risk and tumor characteristics. As we did not have the opportunity to adjust for these variables, the results must be interpreted with caution. In addition, our study did not include any economic calculations on the cost of sending a reminder compared to the potential gain from early diagnosis of cancer, and more research is justified to answer these questions.
In conclusion, postponed attendance in BreastScreen Norway resulted in a higher detection rate of cancer. The tumors were larger, of higher histological grade, and more often lymph node positive. Tumor growth over time could partly explain the difference, but personal reasons for attending after a reminder might also be of influence. Mammographic screening programs should make efforts to avoid delay in the interval between screening examinations. Also, women should be encouraged to attend screening after ordinary invitations to avoid postponing a potential breast cancer diagnosis.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.