
Abstract
Objective
To determine whether signed family physician reminder letters to women overdue for screening mammography prompts rescreening.
Methods
A randomized double-blind trial conducted in 2013 among women aged 51–73 and overdue for screening by 6–24 months. The study was carried out by the publicly funded British Columbia Cancer Agency Screening Mammography Program, which routinely sends standard reminder postcards to women who are due for mammography. Participating family physicians signed letters for the overdue women in their practices. The overdue women were mailed either the signed reminder letter and the standard reminder postcard, or the standard reminder postcard alone. The primary endpoint was the proportion of overdue women that attended a screening mammogram appointment within six months of mailing the study letters. The analysis was by intention to treat.
Results
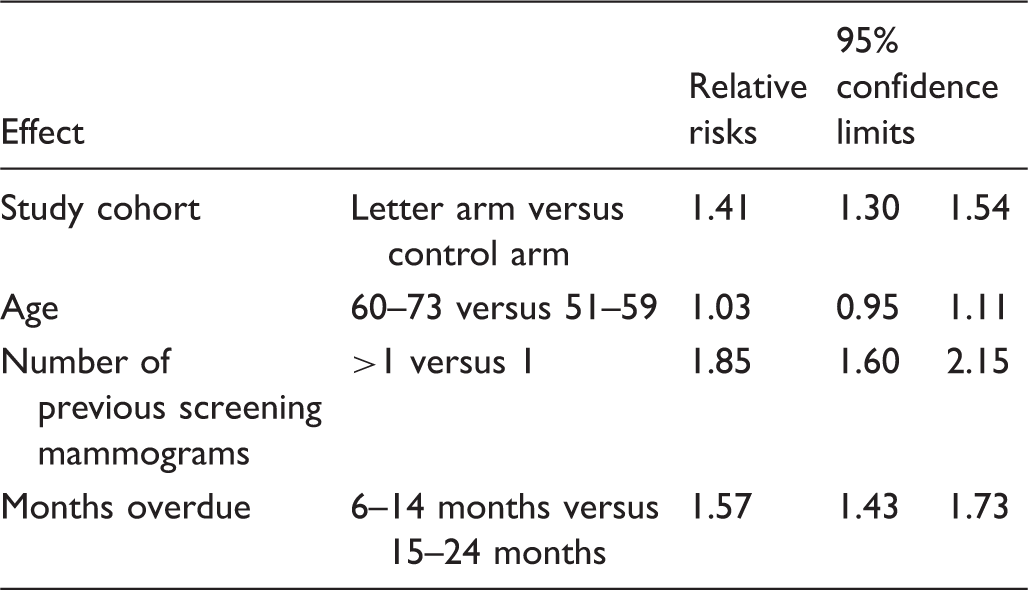
In total, 822 family physicians participated and 5638 women were randomized. Mammography attendance by six months after mailing the reminders was 34.4% (947/2749) for women in the signed family physician letter arm, compared with 24.0% (660/2749) for women in the control arm (p < 0.0001). Adjusting for age, number of previous screening mammograms, and months overdue, women in the signed letter arm were significantly more likely to return for screening than women in the control arm (RR 1.41; 95% confidence interval: 1.30–1.54).
Conclusion
A signed family physician reminder letter improved mammography attendance for women who were overdue for screening mammography.
Introduction
Among women aged 50–74, screening mammography reduces breast cancer mortality and is supported by consistent recommendations.1,2 In British Columbia (BC), Canada, screening mammography has been available via self-referral or physician referral through the Screening Mammography Program of BC (SMP) since 1988. 3 At the time of this study (2013), women aged 50–74 were invited to return for screening every two years, at 38 fixed and three mobile sites throughout the province.
For screening to be effective, participants must return at appropriate intervals after an initial visit. The SMP uses an automated recall system in which reminder postcards are mailed to women five weeks prior to, and if an appointment has not yet been booked, five weeks after the two year anniversary date. If a woman does not book a mammogram, she would receive additional reminder postcards five weeks before, and if an appointment had not yet been booked, five weeks after the three-year anniversary date. In BC, the percentage of women aged 50–69 returning for screening mammography at 30 months was 75.3% for the period 2012–2014. 4
Several published reviews of interventions that improve on time screening rates for breast and other cancers5–9 have shown that generic or personalized reminder systems using print or telephone contacts improve screening attendance. Previous breast, colorectal, and cervical cancer screening studies have evaluated the impact of trust in primary care providers and physician’s attitudes toward screening on participation rates.10–12 Physician’s recommendations for screening have been consistently identified as a significant factor in a person’s decision to undergo screening.13–15
In a trial to investigate reminders from family physicians for women to attend screening mammography, O’Connor et al. 16 randomized 473 women, including a subgroup of 145 previous screenees who did not attend after their last screening invitation. The intervention, a letter recommending screening mammography, was signed by the women’s family physicians and was mailed along with an explanatory leaflet about breast screening two weeks prior to their expected invitation from the breast screening unit. The trial reported no improvement in the likelihood of rescreening in the letter arm in the entire group of women or in the subgroup of overdue women. The objective of our randomized trial was to investigate the effect on rescreening of a personalized reminder letter, signed by a woman’s family physician, in a larger sample of overdue women, who had not returned for rescreening despite standard reminder postcards.
Methods
This randomized, double-blind trial recruited family physicians across BC with women overdue for screening mammography in their practice. Women enrolled in the SMP were invited to return for repeat screening at the 24-month anniversary of a prior appointment, unless a cancer had been diagnosed in the interval or they were scheduled for ongoing diagnostic breast investigations. For this study, the women who had not returned by 30 months from a prior screen were deemed to be “overdue.” The SMP database was queried to identify active family physicians with women in their practices meeting the following criteria: previously enrolled in the SMP, eligible for ongoing screening, aged 51–73, 6–24 months overdue for return screening mammography, residing in BC, and having completed the section of the SMP registration questionnaire saying they were “willing to be contacted in the future for studies relating to cancer research.” In the SMP database, 91% of women had indicated that they were open to such contact. Among SMP attendees, 97.7% had a designated family physician. The remaining 2.3% were under the care of either a nurse practitioner or walk in clinic.
The SMP tests its standard reminder postcards by measuring the percentage of women who attend for screening mammograms after mailing each postcard design. The most effective SMP reminder postcard was selected for use in both arms of this study (eFigure 1). The wording of the family physicians’ letter to overdue women was drafted based on feedback from focus groups evaluating prior written SMP communication materials and then edited in consultation with members of the BC Cancer Agency’s Family Practice Oncology Network.
The REB required the consent of family physicians to participate in the study because, once informed of the overdue women in their practice, the family physicians could have opted either to remind all overdue women themselves, or to allow the overdue women to be randomized in the study. A full page advertisement in the BC Medical Journal promoted the study to physicians one month before mailing of the study packages (eFigure 2). All eligible family physicians received a study package that contained a consent form to sign, a list of the overdue women in their practice, and letters addressed to the identified women to sign (eFigure 3). Participating physicians were asked to sign the consent form, review the list of overdue women, sign the letters for women who were appropriate for screening, and return the signed letters and consent form in a postage paid envelope to the SMP. The physician recruitment phase lasted six weeks. Physicians were neither reminded to participate in the study, nor reimbursed for their time.
Women with signed physician letters were randomized to two groups by the study statistician using a computer-generated random number algorithm. No stratification or minimization factors were used. The family physicians were blinded to the random assignment of the overdue women in their practices. The women were not aware that they were participating in a study and were, therefore, blinded to their random assignment. The REB waived the need for the women’s consent because this study intervention involved minimal risk to the women, the women had agreed to be contacted about research, and because informing the women of their participation in a reminder study might have altered their behavior and rendered the study results invalid.
Women were randomized to receive either the postcard alone (control arm), or the postcard plus the signed letter together (letter arm), mailed in an envelope marked with the return address of the family physician’s office. During the study, the SMP’s automated recall system continued to send reminder postcards to overdue women around the three-year anniversary of their last screening mammogram.
Six months after the mailing, the SMP database was queried to determine which women had attended a screening mammogram appointment. The primary endpoint was the proportion of overdue women who attended screening mammography in the control and letter arms within six months of the mailing.
The sample size was based on two assumptions from prior SMP experience, first that 18% of women who had not attended screening at 30 months after their initial visit attended screening by 36 months, 17 and second, an estimate that the intervention would improve screening attendance by a relative risk of 1.33. 7 Using two-sided statistical testing with alpha = 0.05, the estimated number of overdue women to achieve power = 0.8 was 574 in each arm or 1148 in total. To maximize the likelihood of reaching this sample size in the subgroup of initial screenees, all family physicians in the province were invited to participate in the study.
Analysis was by intention to treat. Only women who were overdue at the start of the physician recruitment phase but who had attended for screening before randomization were excluded from analysis. The Kaplan–Meier method was used to calculate confidence intervals (CIs) around attendance rates. Data were analyzed overall, and by age, number of prior screening mammograms, and months overdue from their expected on time mammography. Statistical analyses were conducted using the SAS 9.3 software (SAS Institute Inc, Cary, NC, USA). The following subgroups were defined for each variable—age: 51–59, 60–73; number of prior screening mammograms: 1 (initial screenees), >1 (subsequent screenees); and months overdue from their expected on time mammography: 6–14 months (few), 15–24 months (many). The random assignment and variables exhibiting significant differences between subgroups were entered into a multivariable log binomial regression model. Relative risk was used as the measure of association, because screening attendance is a relatively common outcome.
This trial was registered with ClinicalTrials.gov (NCT02660788). The University of BC—BC Cancer Agency Research Ethics Board approved the protocol.
Results
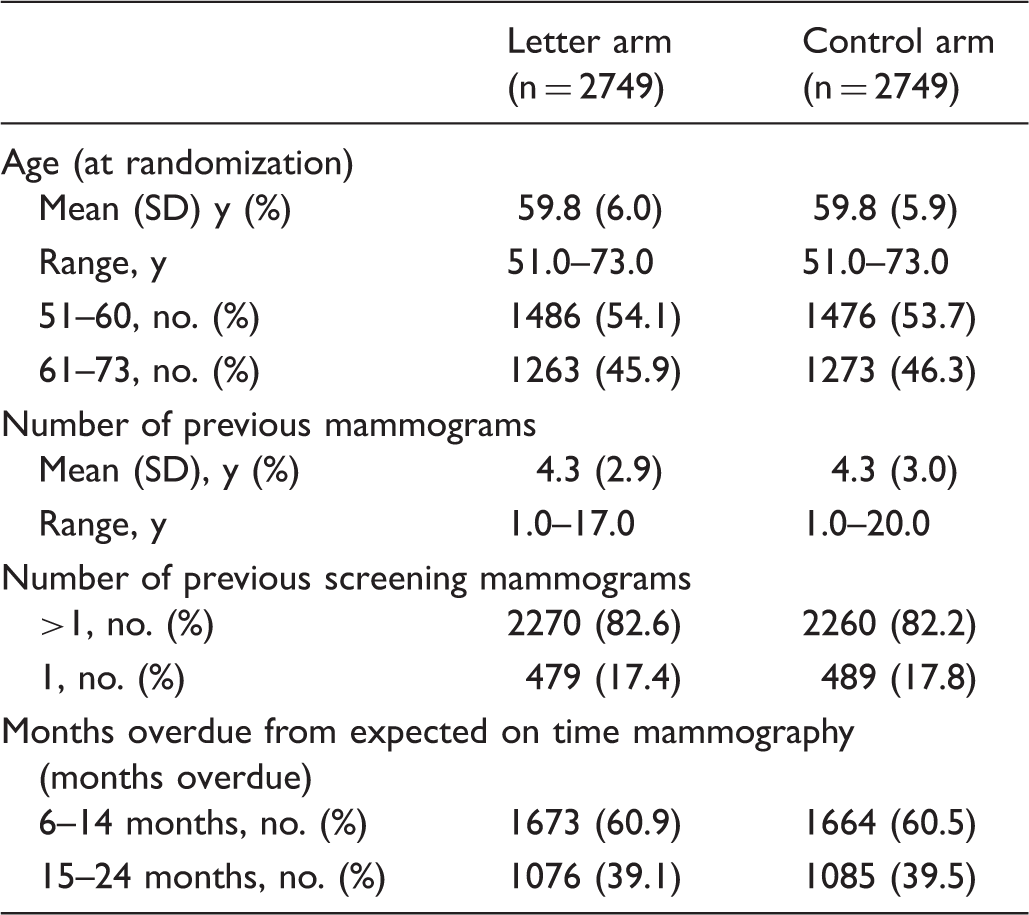
The SMP database query identified 3117 family physicians with 22,865 overdue women in their practices. The physician recruitment period was from 21 February to 3 April 2013. At the time of randomization (16 April 2013), 822 family physicians (26.4% response rate) had responded with correctly signed consent forms and study letters for 5638 eligible women. Between the database query and the date of randomization, 140 women ceased to be overdue and so were excluded, leaving 2749 overdue women in the letter arm and 2749 overdue women in the control arm (see Figure 1). The baseline characteristics of women in the two study arms are described in Table 1.
Flow of the trial. Baseline characteristics of the women in the study. Control arm: reminder postcard alone; Letter arm: signed family physician letter and reminder postcard; SD: standard deviation.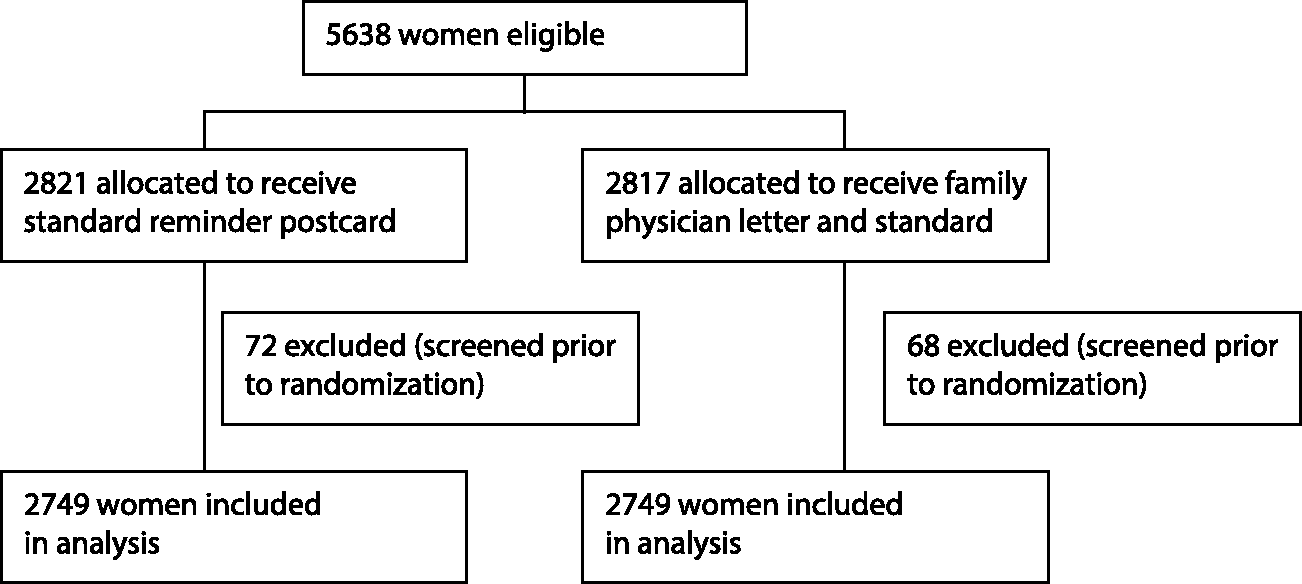
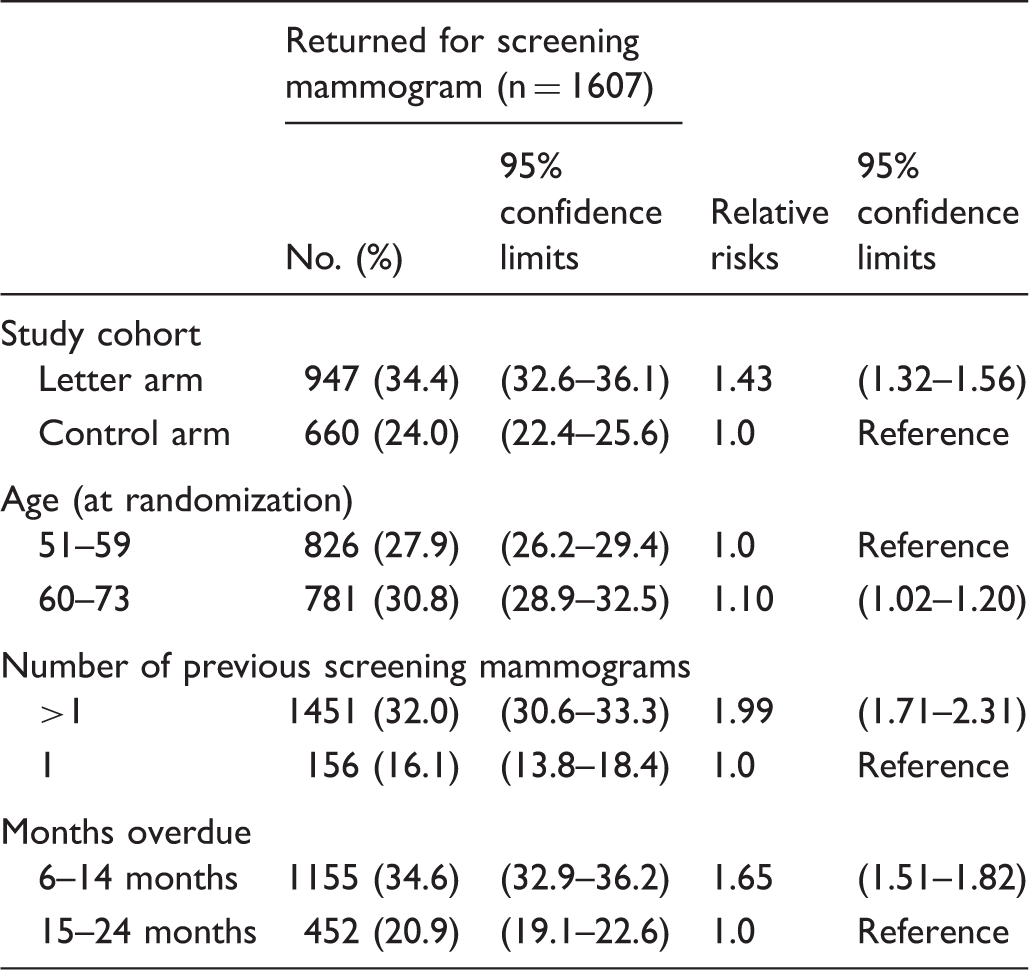
The reminders in our study were mailed to the overdue women on 26 April 2013. Six months later, 34.4% (947/2749) of women in the letter arm had attended the SMP for screening mammography compared with 24.0% (660/2749) in the control arm (p < 0.001). The unadjusted relative risk ratio was 1.43 (95% CI: 1.32–1.56). Attendance for screening mammography over time by study arm is illustrated in Figure 2(a). Response to the signed letter intervention in the following subgroups is illustrated for initial screenees compared with subsequent screenees in Figure 2(b), and few versus many months overdue from their expected on time mammography in Figure 2(c). Women were significantly more likely to attend for repeat screening mammogram in the letter arm than the control arm for all subgroups (see Table 2).
Percentage returning for screening mammography: (a) For study arms, (b) for initial screenees versus subsequent screenees; (c) for few versus many months overdue from the expected on time mammography. Percentage of women returning for screening mammography at six months.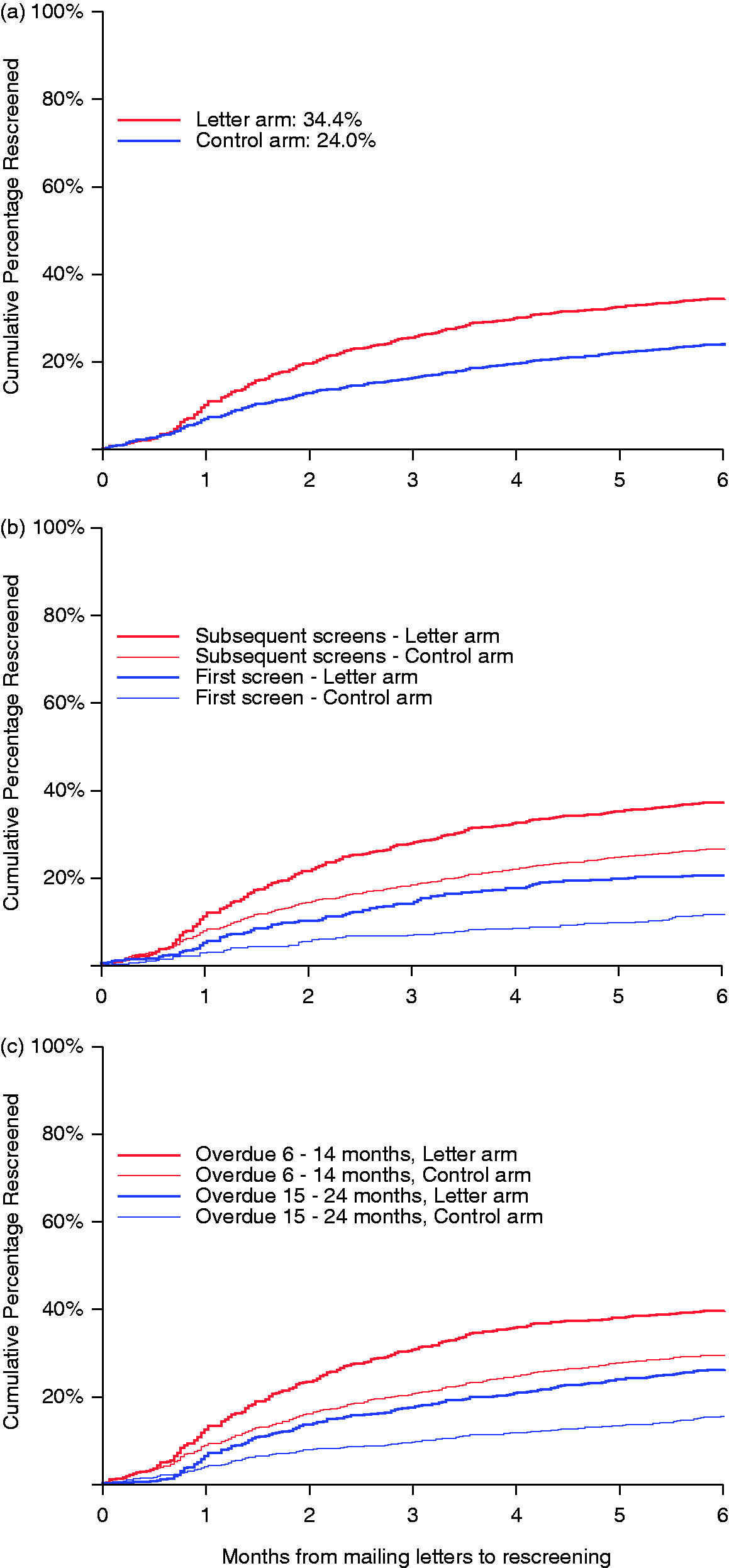
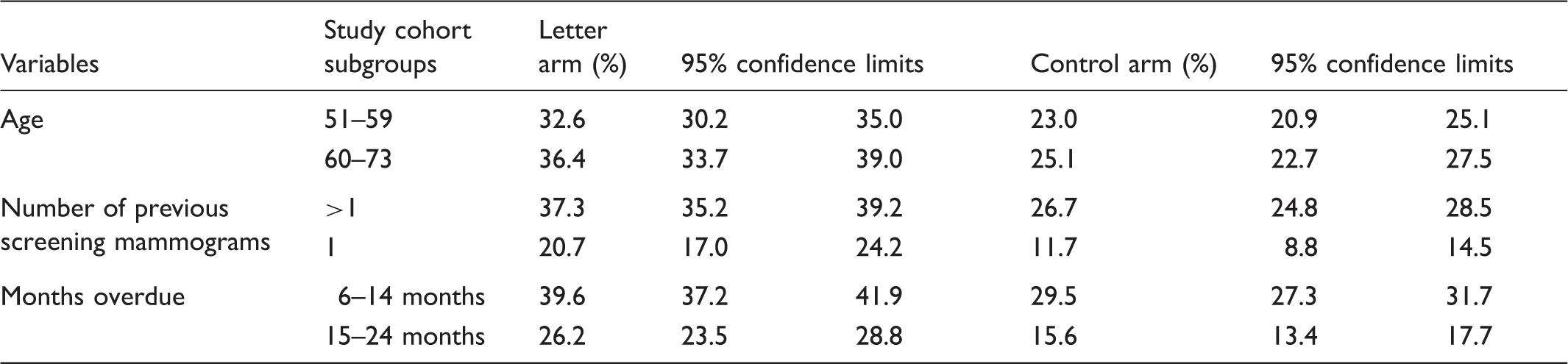
Differences in screening program return rates at six months with unadjusted relative risks and 95% confidence limits.
Multivariable logistic regression model: adjusted relative risks and 95% confidence limits.
Discussion
In this double-blind randomized trial, a reminder letter signed by overdue women’s family physicians significantly increased the percentage of women who returned for screening, from 24 to 34%. This increase was seen in the subgroups defined by age, initial versus subsequent screening, and number of months overdue. These results illustrate that, by expressing concern in a personal letter, family physicians can significantly influence their patients’ behavior. Although an organized screening program conducted this study, the same reminder methodology could be generalized to individual physician’s offices with electronic health records.
Two research groups have studied reminders for women overdue for breast screening.18,19 Phillips et al. 18 showed that, among women overdue for screening mammography, the combination of a letter and a telephone call increased mammography attendance in comparison with a mailed, personalized letter signed by a woman’s physician, or an automated telephone call alone. In a multi-intervention study, Fortuna et al. 19 used a mailed reminder letter from a medical practice (without a physician’s signature) as the control intervention. They found no incremental benefit in the addition of an automated telephone call, an improvement in breast screening participation with the addition of a personal telephone call from a trained outreach worker, and an improvement with an automated reminder telephone call and a paper prompt delivered to the treating clinician at the time of a patient-initiated visit about the individual being overdue for screening.
Two studies have focused on family physician letters as interventions for people overdue for colorectal screening. A randomized controlled trial by Cameron et al. 20 found an improvement in screening for participants with an expired order for colonoscopy using multiple interventions, which included a reminder letter from their family physician. An ongoing UK randomized clinical trial targeting nonresponders 21 is studying the effect of a combined personalized letter signed by the family physician and mailed fecal occult blood test kit, compared with no additional intervention.
Our study had some limitations. It did not determine whether reminder letters would be as effective if signed by another health professional, with a different relationship to the overdue women. In addition, although it would be expedient to mail reminder letters using family physicians’ electronic signatures, this study used genuine signatures from family physicians who vetted the appropriateness of sending a letter to each overdue woman. It is therefore likely that the relative risk observed for the study intervention would be lower if letters were mailed to unselected overdue women. In addition, this study did not determine whether reminder letters with electronic signatures, or text message reminders, would be as effective as letters with handwritten signatures. 22
While the effect of this intervention was large (34% versus 24%) in overdue women, it applies only to the 25% of women in the screening program who were overdue at 30 months. Its effect on the overall population would be to increase attendance by around 2.5% (10% of 25%). It is unknown whether the women who returned for screening because of this intervention would have dropped out of the screening program entirely or resumed screening after being overdue for a period. Our future work will determine whether this intervention improves the overall participation in screening.
Conclusion
This study showed that the addition of a signed family physician reminder letter to a standard reminder postcard system improved mammography attendance for women who were overdue despite prior reminders.
Footnotes
Acknowledgments
We thank Alex Goudreau, Karen Truong, Javis Lui, and the SMP team for their administrative assistance.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for the research was provided by the Canadian Breast Cancer Foundation, BC/Yukon Region. EKC was funded by Canadian Breast Cancer Foundation, BC/Yukon Region Post Graduate Research Fellowship.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.