
Abstract
Objective
In the population-based Swedish regional colorectal cancer (CRC) screening program of Stockholm–Gotland using the fecal immunochemical test (FIT), gender-specific cut-off levels of fecal hemoglobin are applied, since previous studies have indicated a lower sensitivity of FIT for CRC in women. The aim was to evaluate the diagnostic yield and the screening costs overall and per detected CRC of this strategy.
Methods
All individuals aged 60–69 invited to screening in 2015–2017 were included. Cut-off level for positive FIT was 40 µg/g in women and 80 µg/g in men. Those with a positive FIT were referred to colonoscopy. The yield of CRC and screening cost for the study period were assessed and compared to cut-off levels of 80 µg/g in both genders.
Results
Approximately 230,000 individuals were invited. Overall participation rates were 72% in women and 65% in men (p < 0.05). FIT was positive in 4256 individuals (2.7% in both genders). In 3758 colonoscopies, 258 (6.9%) CRCs were detected. The positive predictive value for CRC was significantly higher in men (8.3% vs. 5.8%). In 120 women with CRC, 28 (23%) had FIT < 80 µg/g. Negative colonoscopies were more common in women (24% vs. 17%, p < 0.05). Total costs for the study period were 52,000,000SEK (≈5,200,000€), i.e. 16% higher compared to using cut-off levels of 80 µg/g in both genders, and corresponding to a 3% increment in cost per detected CRC.
Conclusion
The high rate of CRC detected in women in the lowest FIT category outweighs the minor reduction in screening costs if the same cut-off level was used as for men.
Introduction
Colorectal cancer (CRC) is the second most common type of cancer in women and the third most common type in men worldwide. 1 Fecal immunochemical test (FIT)-based screening for CRC is recommended in order to detect disease at an early stage. Individuals with a positive test result are offered colonoscopy, and as FIT is a quantitative test the cut-off level can be matched to the available colonoscopy resources.2,3 Previous evaluations have shown a lower sensitivity for FIT in women than in men for detecting advanced neoplasia4,5 as well as a higher rate of screening program interval cancer in women than in men.6,7 Hence, the Swedish population-based regional program of Stockholm–Gotland switched from guaiac fecal occult blood test (gFOBT) to FIT with gender-specific cut-off levels in 2015. 8
The cost efficiency of FIT screening has been assessed in several studies and reviews, concluding that FIT screening is cost efficient compared to no screening or to screening with colonoscopy.9–12 Simulations of multiple gender-specific as compared to gender-uniform FIT screening strategies have indicated that FIT screening is less effective measured in quality-adjusted life years (QALY) in women, but that gender-based strategies are not more cost-effective than gender-uniform. 13 To determine the gain in QALY with various screening strategies, utility weights are used for each stage of disease. 14 However, the utility weight assigned to each CRC outcome state varies considerably between different studies evaluating quality of life, which could make QALY measurement difficult to assess. 15 Therefore, the present study aimed at using total screening costs and cost per detected CRC as outcome measurement for the cost evaluation. Furthermore, different simulation models can give different estimates of effectiveness for the same screening scenario depending on the underlying assumptions of the model, such as adenoma dwell time, and the external validity of simulation models may be problematic.16–18 Hence, evaluation of existing programs is called for.
The regional screening program of Stockholm–Gotland started in 2008 as the first to use gender-specific cut-off levels, of 40 µg/g for women and 80 µg/g for men, for a positive test. As CRC-screening programs are being implemented nationally and worldwide, assessments of diagnostic yield and costs are imperative.19,20 The aim of this study was to evaluate colonoscopy findings and screening costs overall and per detected CRC in the Stockholm–Gotland screening program 2015–2017 as compared to estimations of a gender-equal cut-off level of 80 µg/g.
Methods
The Stockholm–Gotland CRC screening program is a population-based program inviting all residents aged 60–69 without any exclusions, and has a coverage of 100%. An invitation, along with instructions and a stool test for blood, is sent biennially. Individuals with a positive test are referred for colonoscopy at the clinic closest to their home address. In October 2015, FIT (OC sensor®, Eiken, Japan) replaced gFOBT (Hemoccult®) as the primary test, with a cut-off level for a positive test of 40 µg/g for women and 80 µg/g for men, yielding around 2% positivity among both sexes. 8
The screening program is operated by a central administration at the Regional Cancer Centre of Stockholm–Gotland, which manages the invitations and collects data in the screening register regarding the screening procedure, colonoscopies and FIT results. Details of the shift to FIT from gFOBT, participation and positivity rate have been reported previously. 8
Study population
The study population comprised individuals, aged 60–69, invited to the program from 1 October 2015 until 31 December 2017, including both a screening-naïve population and those previously screened using gFOBT. Since the screening program is biennial, individuals invited in October to December 2015 were also invited in October to December 2017, except if they were then aged > 69, were deceased, were being followed up in the polyp surveillance program or surgical clinic after the previous screening round, or had moved out of the region. The first complete participation, if several, was included in the analysis and each individual was counted only once. The inclusion period was ended on 31 December 2017 to allow for enough follow-up time for completion of the investigation and the time lag for registration in the Swedish Colorectal Cancer Registry (SCRCR).
Fecal immunochemical test
FIT test tubes were mailed to the invitees. After sampling, the participants were instructed to record the sample date on the test tube and return the tube to the laboratory by mail in a prepaid envelope. If the tube was unanalyzable a new kit was sent. A reminder was sent after 8 weeks to nonresponders.
Women with ≥ 40 µg Hb/g feces and men with ≥ 80 µg Hb/g feces were offered colonoscopy at the endoscopy unit closest to their home address.
Participants who did not have the FIT sample analyzed within 1 month of taking the sample or did not complete colonoscopy within 6 months were excluded. This was to ensure that the FIT laboratory analysis was timely, and to allow CRC specimens a complete histopathological diagnosis and registration in SCRCR, i.e. colonoscopy before 1 July 2018. Findings of CRC and advanced adenoma were evaluated for all participants that completed the investigation.
Colonoscopy and findings
Bowel preparation was performed according to the clinical practice of the endoscopy unit. Colonoscopy quality parameters such as bowel cleaning, cecal intubation, and withdrawal time, along with the colonoscopy findings and possible immediate complications were recorded in the screening register.
The colonoscopy findings were classified as CRC (invasion beyond muscularis mucosae), advanced adenoma (AA) that required follow-up colonoscopy (according to Swedish polyp surveillance program: adenomas ≥10 mm, those with high-grade dysplasia or villous histology, serrated polyps with dysplasia or ≥10 mm in size, ≥3 low-risk adenomas), low-risk adenoma not requiring follow-up colonoscopy (non-AA: 1–2 tubular adenomas <10 mm, sessile serrated adenomas < 10 mm and without dysplasia), other sources of bleeding (hemorrhoids, angiodysplasia, inflammation), and clean colon where no source of bleeding was found. The most severe lesion determined the classification.
Results from pathology reports of polyps were recorded in the screening register. Participants with AA are recommended a follow-up colonoscopy after 3 years, according to the Swedish polyp surveillance program. 21 Participants with no need for follow up were continued to be invited in the screening program.
All CRCs were verified by matching of data to the SCRCR, which is a national register with high validity and a coverage of > 98%. 22 CRC stage was classified according to TNM7 and grouped into stage I–II (no regional lymph node metastases), III (regional lymph node metastases or tumor deposits), IV (distant metastases). Information on stage (pTNM) was retrieved from the pathology report for the surgical specimen and was completed with clinical data (cTNM) regarding stage IV and in the case of missing data. Screening-detected CRC was defined as CRC diagnosed within 6 months of the screening colonoscopy. If there was uncertainty whether the CRC was screening detected or not, the patient’s medical record was reviewed.
Cost analysis
The costs for invitation, FIT analysis and materials were retrieved from the Regional Cancer Centre's national fees for screening (personal communication with central screening nurse). The costs for colonoscopy procedure were retrieved from the NordDRG database at the Swedish National Board of Health and Welfare. 23
The cost analysis was done for all participants and included index colonoscopies and follow-up colonoscopy for AAs. Only costs associated with the screening procedures were included. The costs were compared with the estimated costs had the FIT cut-off level been 80 µg/g in both men and women. In a separate sensitivity analysis the estimated cost of follow-up colonoscopy was excluded.
Additional costs of CRC treatment or indirect costs due to absence from work were not included in the analysis, and nor were estimated costs for colonoscopy complications, such as perforations and bleeding.
Statistics
FIT positivity was defined as the number of FITs above or equal to the cut-off level divided by the number of participants with analyzable tests. Positive predictive value (PPV) was defined as the number of participants with AA or CRC divided by the number of colonoscopies among FIT positives. PPV was estimated overall, for men and women, and for different FIT cut-off levels. Number needed to scope (NNS) was defined as the number of colonoscopies required per detected CRC or AA. NNS was estimated for all participants and in subgroups as above. Differences between gender and FIT category (40–79 µg/g, ≥ 80 µg/g) subgroups in proportion of CRC and AA, CRC localization and CRC stage were analyzed using chi-squared test. P-values < 0.05 were considered statistically significant, and 95% confidence intervals (CI) were calculated. All statistical analyses were done in R version 3.6.2 (R Core Team 2019, Vienna, Austria; www.R-project.org).
Ethical permission and consent
The study was approved by the Regional Ethics Board in Stockholm (no. 2019–04850). Informed consent was considered when a participant sent in the test tube. Access to underlying research material can be obtained by email to the corresponding author.
Results
Invitations to screening were sent to 229,944 individuals, aged 60–69, between 1 October 2015 and 31 December 2017. Of the invitees, 6309 were invited twice (October–December 2015 and October–December 2017) and their first compliant participation, if more than one, was included in further analysis. Overall, 158,149 participated of whom 4256 (2.7%) were FIT positive. Participation and FIT positivity in different age and gender groups are detailed in Table 1. In all age groups, FIT participation was higher among women than men (72% vs. 65%, p < 0.05). FIT positivity was 2.7% and equal between genders. Compliance to complete colonoscopy was 88% overall and higher among women than men (90% vs. 86%, p < 0.05).
Participation and FIT positivity rate in the Stockholm–Gotland FIT screening program in different age and gender groups.
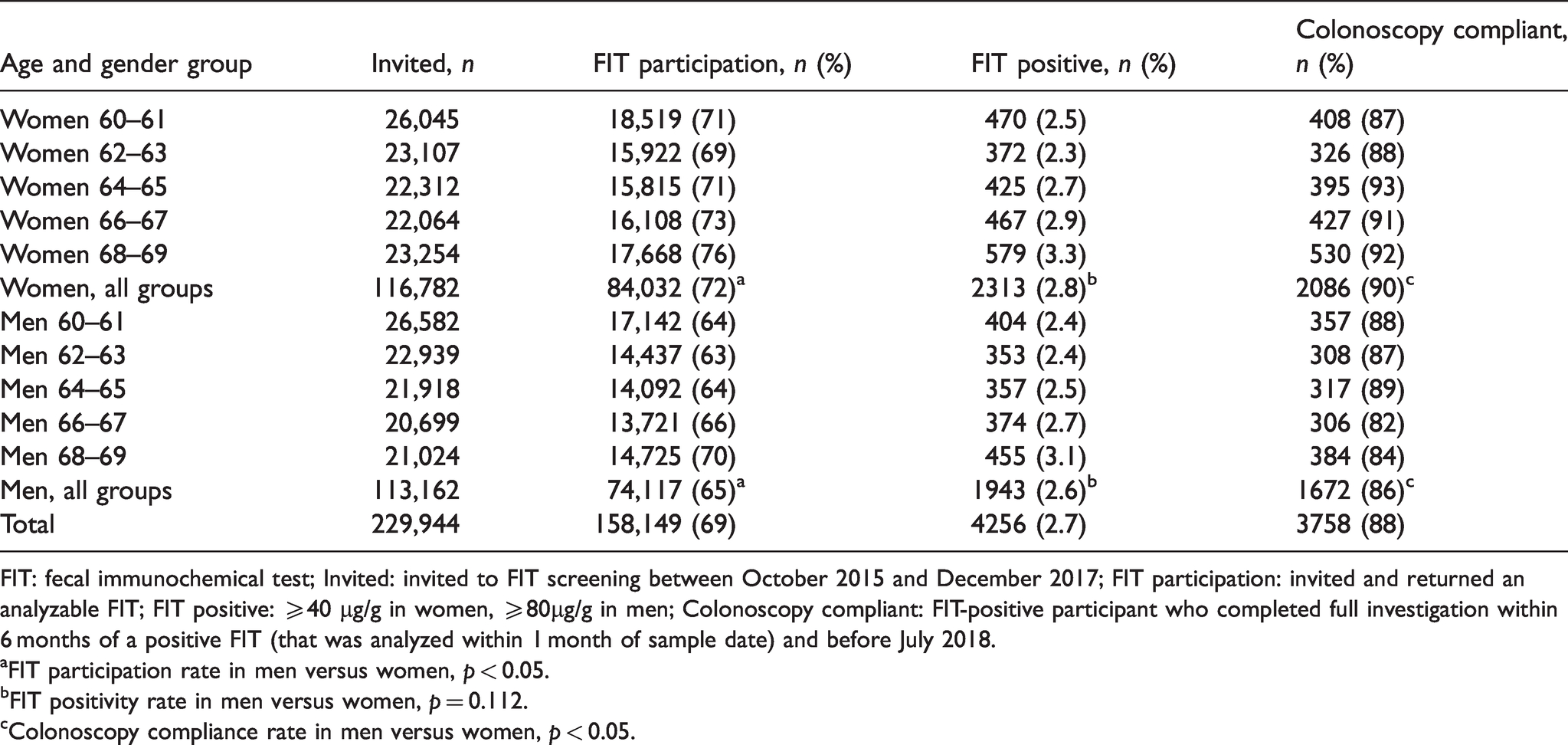
FIT: fecal immunochemical test; Invited: invited to FIT screening between October 2015 and December 2017; FIT participation: invited and returned an analyzable FIT; FIT positive: ≥40 µg/g in women, ≥80µg/g in men; Colonoscopy compliant: FIT-positive participant who completed full investigation within 6 months of a positive FIT (that was analyzed within 1 month of sample date) and before July 2018.
aFIT participation rate in men versus women, p < 0.05.
bFIT positivity rate in men versus women, p = 0.112.
cColonoscopy compliance rate in men versus women, p < 0.05.
Of the 3872 FIT positives who complied with colonoscopy, 114 were excluded from further analysis of colonoscopy findings due to more than 1 month duration from sample taken to sample analysis, or more than 6 months’ duration from sample taken to performed colonoscopy (Figure 1). Three participants had symptomatic CRC diagnosed by nonscreening-initiated colonoscopy and were thus not counted as screening-detected CRCs.
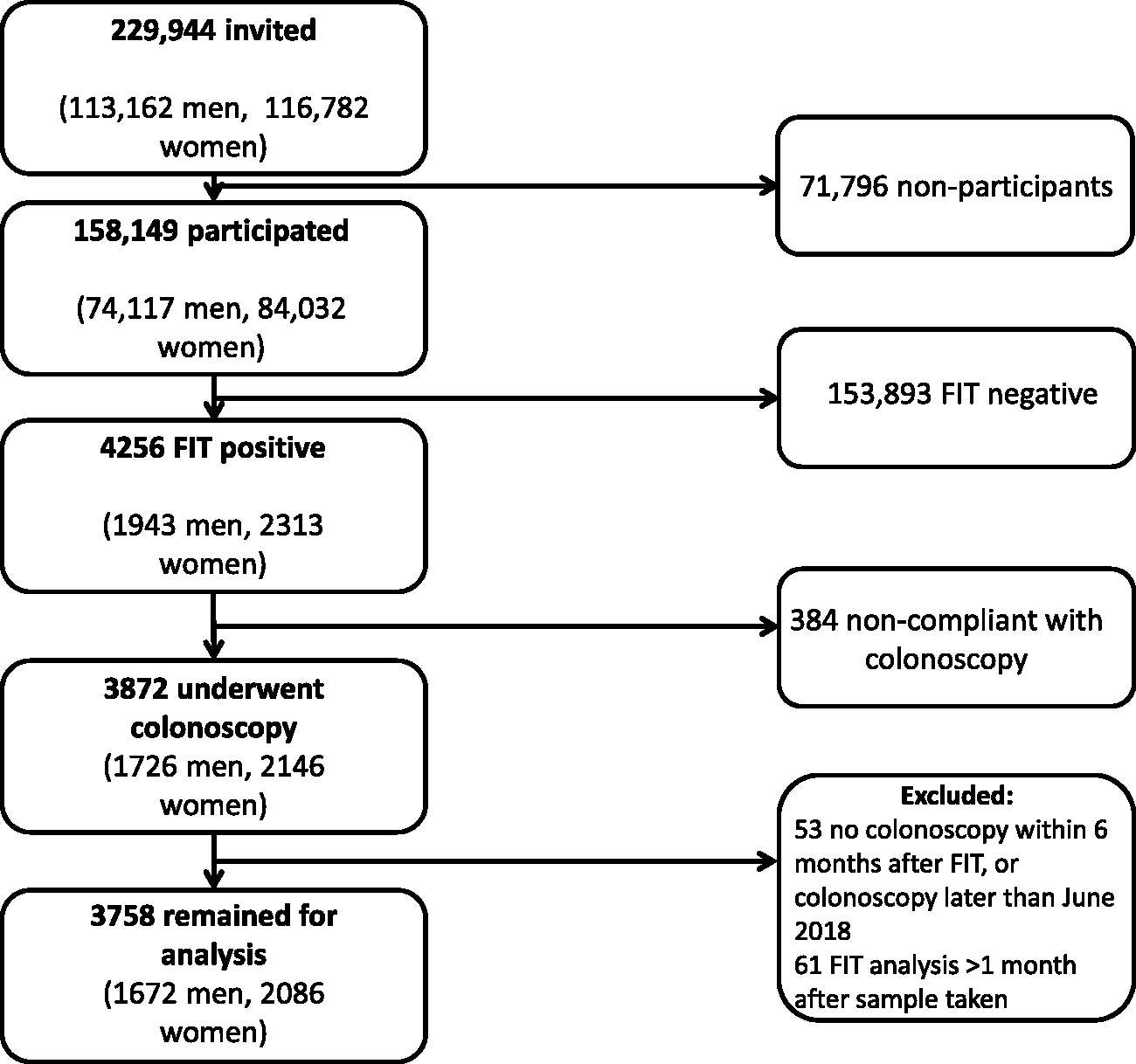
Flowchart of screening participants in the Stockholm–Gotland screening program 2015–2017.
Details of the 1672 men and 2086 women who completed colonoscopy are listed in Table 2. Clean colon and cecal intubation was complete in 97% and cecal withdrawal time >10 min in 99% of the colonoscopies. Screening-detected CRC was found in 138 (8.3%) men and 120 (5.8%) women (p = 0.003 between genders). CRC proximal to splenic flexure was significantly more common in women than in men: 37 (31%) versus 25 (18%) (p = 0.025). Of participants with CRC, 148 (57%) were early stage (stage I–II). The distribution of CRC stage I–II versus III–IV between men and women was similar (p = 0.749). The proportion of normal colonoscopies was significantly higher in women than in men: 498 (24%) versus 276 (17%) (p < 0.05).
Colonoscopy findings and quality parameters in 1672 men and 2086 women who completed screening.
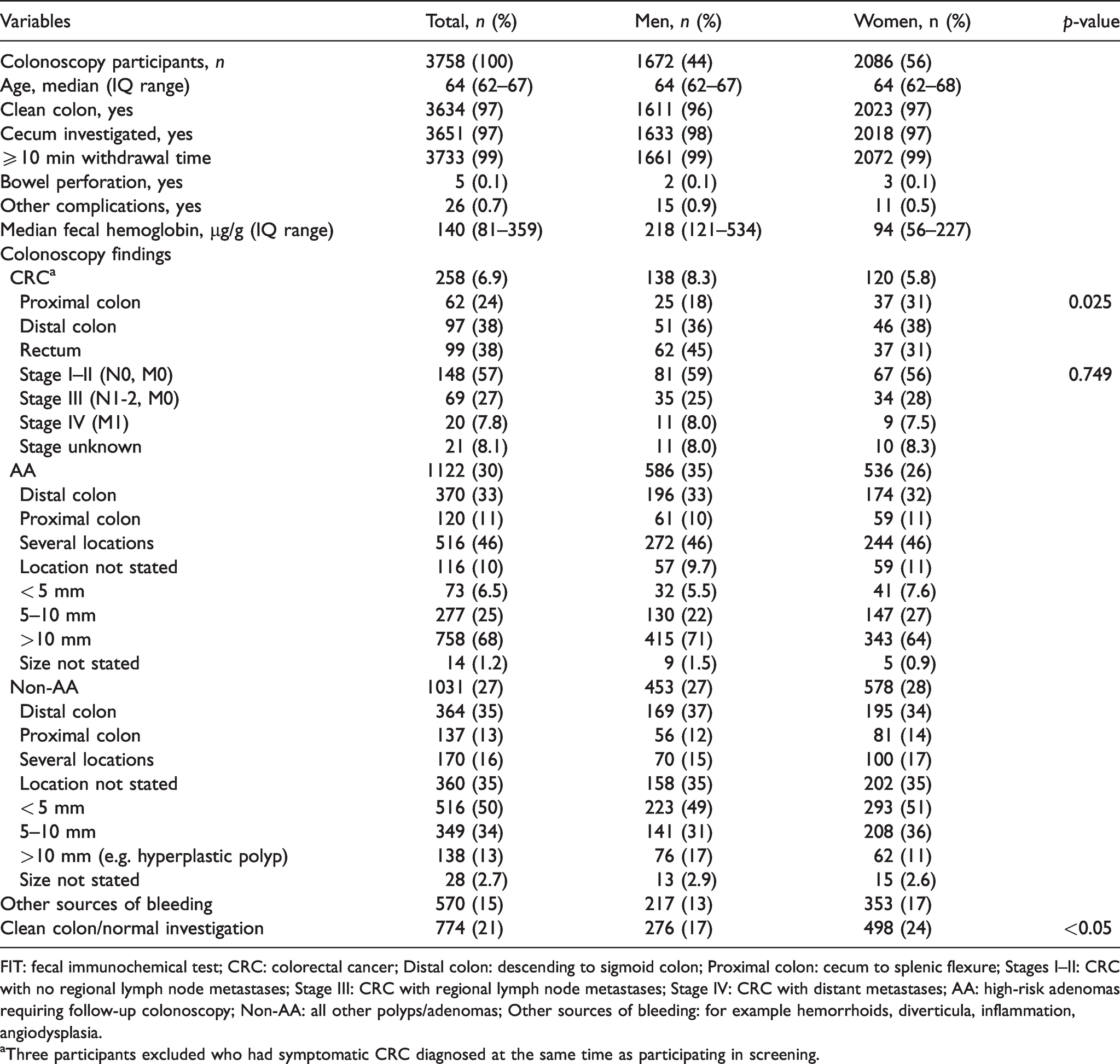
FIT: fecal immunochemical test; CRC: colorectal cancer; Distal colon: descending to sigmoid colon; Proximal colon: cecum to splenic flexure; Stages I–II: CRC with no regional lymph node metastases; Stage III: CRC with regional lymph node metastases; Stage IV: CRC with distant metastases; AA: high-risk adenomas requiring follow-up colonoscopy; Non-AA: all other polyps/adenomas; Other sources of bleeding: for example hemorrhoids, diverticula, inflammation, angiodysplasia.
aThree participants excluded who had symptomatic CRC diagnosed at the same time as participating in screening.
The number of colonoscopies and advanced colonoscopy findings in men and women at different FIT cut-off levels for a positive test are listed in Table 3. With the current screening strategy, the PPVs for CRC and AA were significantly higher in men than in women: 8.3 (95% CI 6.9–9.6) versus 5.8 (95% CI 4.8–6.8) and 35.0 (32.8–37.3) versus 25.7 (23.8–27.6), respectively. With a cut-off level of 80 µg/g in women, the PPV for CRC was equal to that in men (7.7 [6.2–9.2], p = 0.648).
Colonoscopies required, advanced findings and positive predictive values at different FIT cut-off levels among 74,117 men and 84,032 women who sent in FIT samples.
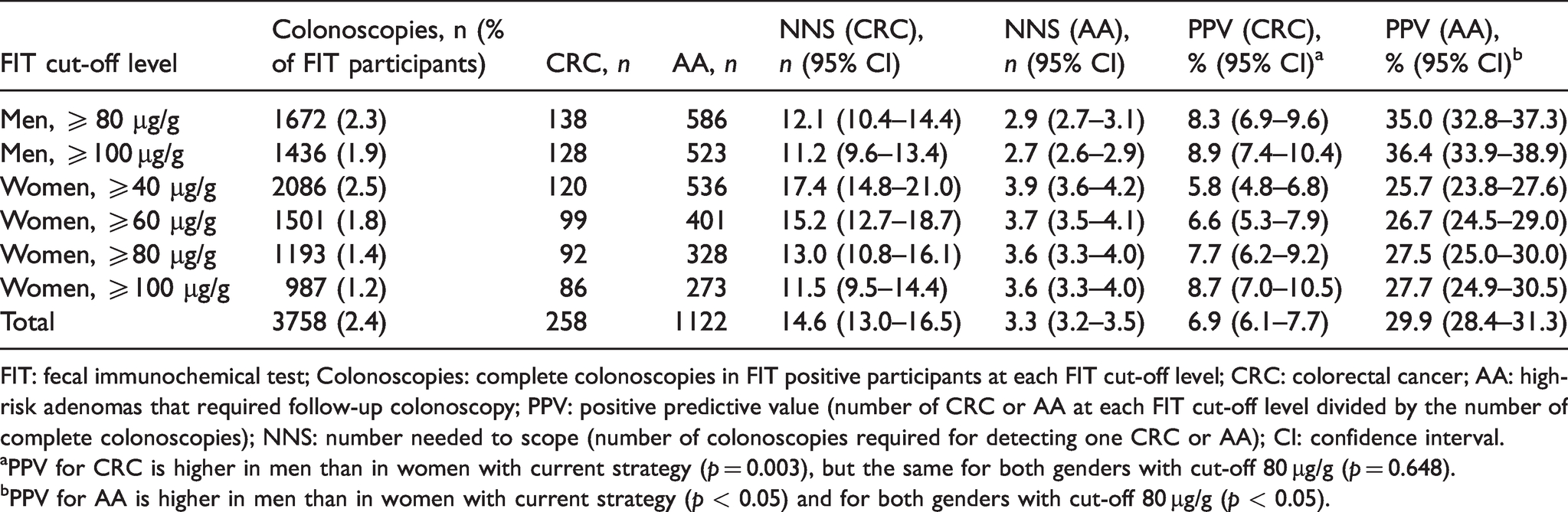
FIT: fecal immunochemical test; Colonoscopies: complete colonoscopies in FIT positive participants at each FIT cut-off level; CRC: colorectal cancer; AA: high-risk adenomas that required follow-up colonoscopy; PPV: positive predictive value (number of CRC or AA at each FIT cut-off level divided by the number of complete colonoscopies); NNS: number needed to scope (number of colonoscopies required for detecting one CRC or AA); CI: confidence interval.
aPPV for CRC is higher in men than in women with current strategy (p = 0.003), but the same for both genders with cut-off 80 µg/g (p = 0.648).
bPPV for AA is higher in men than in women with current strategy (p < 0.05) and for both genders with cut-off 80 µg/g (p < 0.05).
Colonoscopy findings in women are specified in Table 4. Of the 120 women detected with CRC, 28 (23%) had FIT category 40–79 µg/g and would thus have remained undiagnosed at a cut-off level of 80 µg/g for a positive test. Of the CRCs in this low FIT category, 15 (54%) were stage I–II and 8 (29%) were stage III–IV. The proportion of proximal and early stage CRC was the same in women with FIT < 80 µg/g as compared to those with FIT ≥80 µg/g. Forty-nine percent of women with a normal colonoscopy had FIT < 80 µg/g.
Colonoscopy findings in women by different FIT categories.
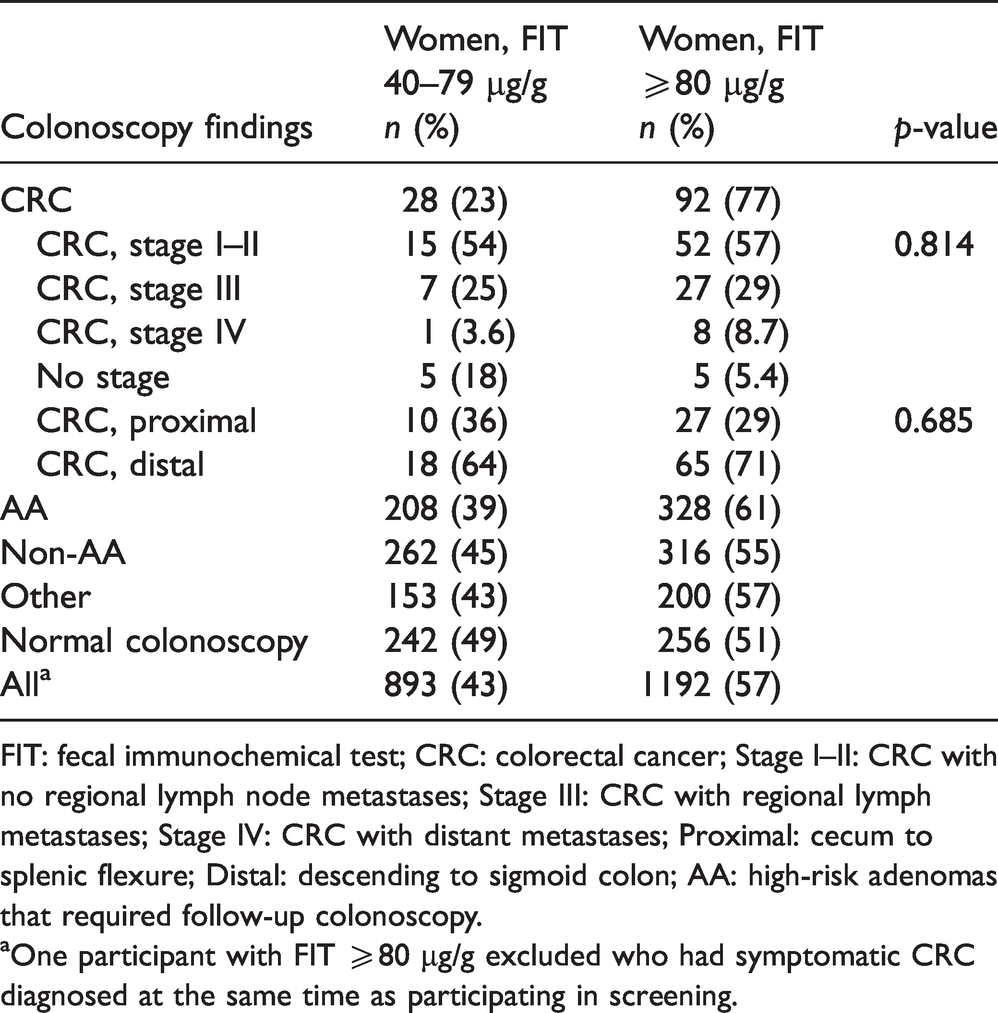
FIT: fecal immunochemical test; CRC: colorectal cancer; Stage I–II: CRC with no regional lymph node metastases; Stage III: CRC with regional lymph metastases; Stage IV: CRC with distant metastases; Proximal: cecum to splenic flexure; Distal: descending to sigmoid colon; AA: high-risk adenomas that required follow-up colonoscopy.
aOne participant with FIT ≥80 µg/g excluded who had symptomatic CRC diagnosed at the same time as participating in screening.
The costs of administration, invitation, laboratory analysis and colonoscopy are listed in Supplementary Table 1. In Table 5, costs are summarized for the total study period with the current screening strategy, and an estimation is given of costs with cut-off level 80 µg/g for both genders. Of all 3758 index colonoscopies, 893 (24%) were performed in women with FIT < 80 µg/g.
Estimated costs for Stockholm–Gotland screening program with current strategy of cut-off of 80 µg/g for men and 40 µg/g for women, and expected costs with equal cut-off of 80 µg/g.
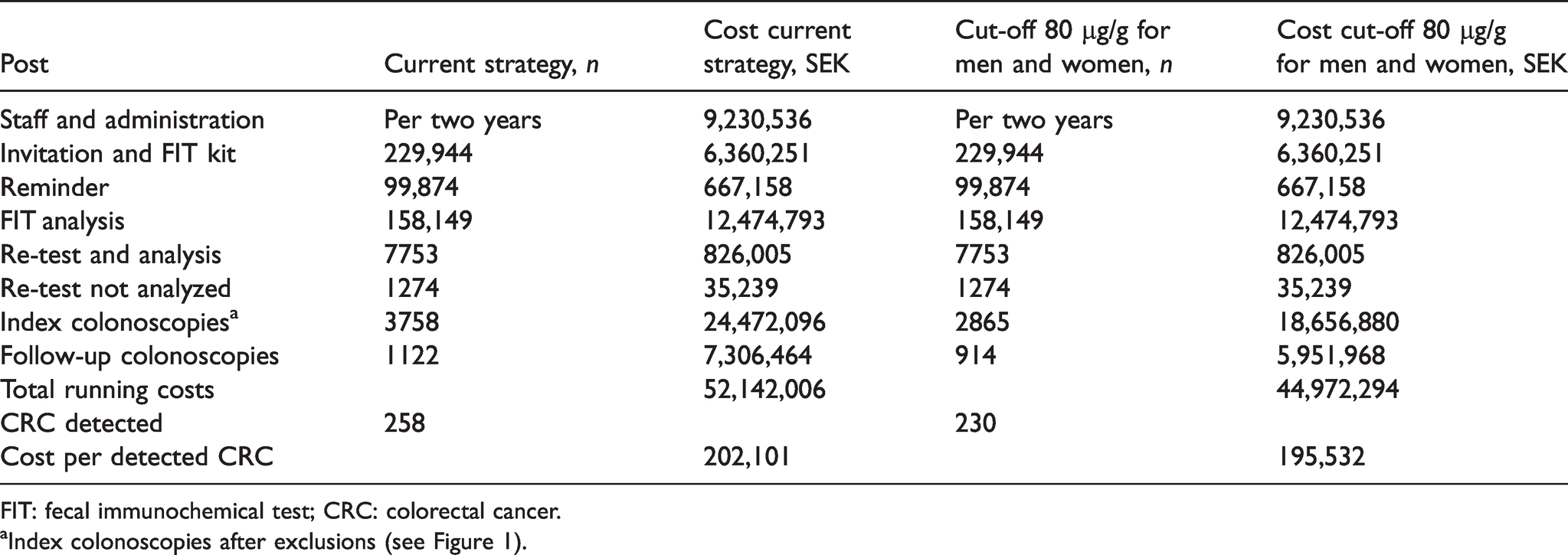
FIT: fecal immunochemical test; CRC: colorectal cancer.
aIndex colonoscopies after exclusions (see Figure 1).
The total cost was 52,142,006 SEK (≈5,188,259€) for the 3758 index colonoscopies and 1122 follow-up colonoscopies. In addition, there was a cost for administration of the screening program of 4,615,268 SEK (≈459,231€) per year regardless of screening strategy; hence this was not included. Of the total running costs, the current strategy was 16% more expensive than a strategy with gender-equal cut-off levels. The cost per detected CRC was 196,000 SEK (≈19,502€) with gender-equal cut-off levels, as compared to 202,000 SEK (≈20,100€) with the current strategy. This corresponds to a 3% increment for the gender-specific cut-off levels.
A sensitivity analysis was performed where the follow-up colonoscopies were excluded. With the current screening strategy, the total running costs were 44,835,542 SEK (≈4,461,248€) corresponding to 173,781 SEK (≈17,292€) per detected CRC. The equivalent cost for a gender-equal strategy was 39,020,326 SEK (≈3,882,620€) corresponding to 169,654 SEK (≈16,880€) per detected CRC, which gave almost equal percentages of savings as in the current model.
Discussion
As CRC screening is being implemented worldwide as well as nationally in Sweden, estimations of costs and colonoscopy yield are urgently needed. This study provides the first results from an established screening program with gender-specific cut-off levels, relevant for decisions on screening strategy. Our evaluation of the population-based Swedish FIT screening program of Stockholm–Gotland, with a fecal hemoglobin cut-off level of 40 µg/g and 80 µg/g for women and men respectively, demonstrated a significantly higher rate of detected CRC and AA in men than in women, as well as a higher rate of normal colonoscopies in women compared to men. However, 23% of screen-detected CRC in women would have been missed with an equal cut-off of 80 µg/g in both genders, with a minor reduction in the screening-associated costs.
Our study found a higher PPV for CRC and AA in men than in women with the current strategy, relating to a higher prevalence of advanced neoplasia (AA and CRC) in men. 24 At cut-off 80 µg/g in both men and women, PPV for AA was higher in men but gender differences in PPV for CRC were nonsignificant, similar to a recent Swedish screening study. 25 Equal PPVs for advanced neoplasia were found in a previous randomized trial through a range of FIT cut-off levels, 26 but others have found a consistently lower PPV for advanced neoplasia in women as well as a lower sensitivity. 4
The lower the FIT threshold applied for a positive test, the higher is the observed detection rate of advanced neoplasia in both men and women. 27 Over repeated screening rounds, some of the missed lesions in previous rounds are detected, but the cumulative detection rate remains higher with a low cut-off level. 28 In men, but to a lesser extent in women, the detection of advanced neoplasia decreases from prevalence to incidence rounds, reflecting the higher prevalence and sensitivity in men than in women.13,29 As the prevalence of advanced neoplasia is higher in men, it is expected that the yield in screening is higher in men. Efforts to equalize the FIT positivity rate and colonoscopy findings between the genders, such as lowering the cut-off level in women, might render a proportionally larger detection rate in women. However, when evaluating the yield, the rate of missed lesions must be considered. Missed lesions will be higher in women than in men if screening sensitivity is lower in women, and hence provide a rationale for applying a lower cut-off level in women.6,7 Indeed, early evaluation of the Finnish gFOBT screening program revealed no survival benefit for participating women. 30 Previous evaluation of the gFOBT program in Stockholm–Gotland found a higher rate of interval cancers in women than in men, which warranted the switch from gFOBT to FIT with gender-specific cut-off levels. 31 A similar strategy is also being launched in Finland. 32 The proportion of interval cancers is estimated to be lower in FIT programs than in gFOBT programs, and future studies will assess the interval cancer rate in the Stockholm–Gotland program. 33
The rate of proximal CRC was the same in women with FIT category 40–79 µg/g as in women with FIT ≥80 µg/g. An equal distribution of proximal CRC in those with high levels of FIT as compared to those with low levels seems to be consistent with a recent meta-analysis that found equal FIT sensitivity for proximal and distal CRC. 34 As increased FIT levels are associated with a more severe advanced neoplasia, early stage CRC is presumed to be represented in the low FIT range.35,36 This could not be demonstrated in the present study, where the proportion of early stage CRC was equal in men and women as well as between women in the high and low FIT categories. However, the number of observations in the female subgroups was limited.
In the Stockholm–Gotland screening program the rate of normal colonoscopy investigations in women was 24% and significantly higher than in men (17%), and 24% of the total number of colonoscopies in the program were performed in women with FIT 40–79 µg/g. The benefit of detecting more CRC in women with gender-specific cut-off levels must be balanced against a high rate of unnecessary colonoscopies and the risk of complications due to the procedure. In an Italian screening program, the overall risk of adverse events was 0.42%, and the mortality was 15/118,000 colonoscopies. 37 The Dutch screening program estimated the colonoscopy-related mortality to be 0.23–0.91 per 10,000 colonoscopies. 38 In an evaluation of the Stockholm–Gotland gFOBT screening program, there were no deaths related to colonoscopy, and all complications of bleeding and perforation were related to polypectomy. 39 Complications are rare, especially after a diagnostic colonoscopy, and the benefit of screening seems to outweigh them.
Apart from the risk of complications, a positive FIT with a negative follow-up screening colonoscopy could be associated with emotional distress due to the false positive test—more frequent among women—sometimes persisting for a long time after a negative colonoscopy.40,41 Other studies, however, have shown an improved quality of life after screening colonoscopy regardless of the colonoscopy findings. 42
For detection of the 28 CRCs in women with FIT 40–79 µg/g of which 15 were stages I and II and 8 were stages III and IV, the estimated costs were 16% higher compared to the cost using gender-equal cut-off levels. The increment in cost per detected CRC was only 3%, from 196,000 to 202,000 SEK (corresponding to ≈19,502€ to 20,100€ respectively). As a comparison, a case–control study from Germany estimated an annual treatment cost of 15–21,000€ for early stage CRC (I–II) and 30–35,000€ for late stage CRC (III–IV). 43
This study is limited only to the costs of the screening episode, and does not include cost for CRC treatment, indirect costs due to absence from work, complications of screening colonoscopy or the displacement effects of a high number of normal colonoscopies in women relative to other indications for colonoscopy. QALY and cost per QALY gained (incremental cost-effectiveness ratio) were not meaningful to calculate based on a short study period such as in this evaluation, but should rather take into account the intended repeated participation in a FIT screening program. Other limitations are that histopathological information was not available for some of the patients with AA in the screening register, and thus the classification of AA relied on the judgment of the endoscopist. However, this problem was limited (68 out of 1122), and for the sake of the cost analysis the definition seems justified since all with AA rendered a follow-up colonoscopy.
Moreover, this study does not provide the colonoscopy yield and costs for one screening round of 24 months but for the study period of 27 months. The study period was ended in December 2017 to permit enough follow-up time for verification of diagnosis. This also means that some individuals were invited twice, but each individual was only counted once. Additionally, some individuals were invited for the first time at the end of the study period that would not have been included if only one screening round of 24 months was evaluated. However, the main aim of the present study was not to evaluate the cost for one screening round in absolute numbers, but to compare the yield and cost per detected CRC using gender-specific cut-off levels of 40 µg/g for women and 80 µg/g for men with those of a gender-equal cut-off level of 80 µg/g. Furthermore, narrowing the inclusion period to 24 months would generate fewer included colonoscopies and hence lower costs, but also fewer detected CRCs. The resulting differences in cost per detected CRC between the two screening strategies might thus resemble the one estimated in our cohort. Fewer included participants would also have impaired the statistical strength of the study.
The strength of this study is the evaluation of a large, established FIT screening program with gender-specific cut-off levels and 100% coverage, in a population of both screening naïve and previously screened invitees, and in which all diagnosed CRCs were verified against the SCRCR.
In conclusion, we suggest that the high rate of CRC detected in women in the lowest FIT category in the Stockholm–Gotland screening program with a fecal hemoglobin cut-off level of 40 µg/g for women and 80 µg/g for men outweighs the estimated 16% cost increment as compared to using a gender-equal cut-off level of 80 µg/g. Future studies will address the interval cancer rate by gender in the program.
Supplemental Material
sj-pdf-1-msc-10.1177_09691413211020035 - Supplemental material for Gender-specific cut-off levels in colorectal cancer screening with fecal immunochemical test: A population-based study of colonoscopy findings and costs
Supplemental material, sj-pdf-1-msc-10.1177_09691413211020035 for Gender-specific cut-off levels in colorectal cancer screening with fecal immunochemical test: A population-based study of colonoscopy findings and costs by Hanna Ribbing Wilén, Deborah Saraste and Johannes Blom in Journal of Medical Screening
Footnotes
Authors’ contribution
Hanna Ribbing Wilén: design of the study, analysis and interpretation of data, and manuscript writing; Deborah Saraste: design of the study, analysis and interpretation of data, and critical revision of the article; Johannes Blom: design of the study, analysis and interpretation of data, and critical revision of the article.
Acknowledgements
Thanks to Daniel Öhman at the Regional Cancer Centre of Stockholm–Gotland for managing the data withdrawal. Thanks to Marika Sventelius at the Regional Cancer Centre of Stockholm–Gotland for detailed information about the screening program. Karolinska University Hospital, Trauma & Reparative Medicine, is thanked for allocating working time for the realization of this study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support of this article: This work was supported by Stockholm County Council.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.