
Abstract
Objectives
Colorectal cancer is among the top three most common cancers globally. In order to reduce the health burden, it is important to improve the uptake of colorectal cancer screening by understanding the barriers and facilitators encountered. There are numerous reports in the literature on the views of the general public on cancer screening. However, the experiences of colonoscopy patients are not as well studied. This paper maps their perceptions.
Methods
Keyword searches for terms such as ‘colorectal’, ‘colonoscopy’ and ‘qualitative’ were conducted on 3 December 2019 in five databases: Medline, Embase, CINAHL, PsycINFO and Web of Science Core Collection. Qualitative articles that quoted colonoscopy-experienced patients with no prior history of colorectal cancer were included for the thematic analysis. The systematic review was then synthesized according to PRISMA guidelines.
Results
The major themes were distilled into three categories: pre-procedure, during and post-procedure. The factors identified in the pre-procedure phase include the troublesome bowel preparation, poor quality of information provided and the dynamics within a support network. Perceptions of pain, emotional discomfort and the role of providers mark the experience during the procedure. The receipt of results, opportunities given for discussion and finances relating to colonoscopy are important post-procedure events.
Conclusion
Understanding colorectal cancer screening behaviour is fundamental for healthcare providers and authorities to develop system and personal level changes for the improvement of colorectal cancer screening services. The key areas include patient comfort, the use of clearer instructional aids and graphics, establishing good patient rapport, and the availability of individualized options for sedation and the procedure.
Introduction
Rapidly developing and developed countries encounter the problem of an increasing burden of chronic diseases, notably colorectal cancer (CRC), which is among the top three most common cancers in the world. 1 In 2018, in the United States alone, the approximate number of new cases was over 140,000, with 50,630 deaths. 2 The early detection of CRC through screening modalities such as colonoscopy can reduce the health burden of this cancer. While colonoscopy is considered the definitive method of CRC screening (CRCS), there is often an inertia in undergoing this procedure, even though it demonstrates better staging and overall long-term survivability outcomes. 3 , 4 CRCS rates by colonoscopy remain low with suboptimal adherence to screening guidelines for follow-ups.5–7
Broad coverage has been given to the general public – who constitute most of the unscreened population – in order to understand the facilitators and barriers encountered with regards to colonoscopy.8–10 While this provides insight into the fears and desires of those unscreened, it is limited in depth and coverage. It merely considers perceptions about colonoscopy that are shaped by others. 10 Instead, resources could be channelled into gathering the opinions of screened patients based on their first-hand experience of colonoscopy. Screened patients are a unique population that is less studied but offers accurate and practical wisdom pertaining to the current practice of colonoscopy and its negative connotations. These opinions can be analysed to determine the factors that contribute to a poor experience. Subsequently, the knowledge obtained can influence strategies for managing and improving CRCS services.
Thus, we aim to review current qualitative papers on the post-procedure views of patients who have undergone a colonoscopy as part of a screening. A qualitative approach allows for the compilation and mapping of the rich personal accounts of patients, to provide a deeper level of understanding around the experience of having a colonoscopy.
Methods
The systematic review was synthesized according to PRISMA Guidelines. 11 Searches were conducted using five electronic databases (Medline, Embase, CINAHL, PsycINFO, Web of Science Core Collection) from inception to 3 December 2019. The search strategy was developed with assistance from a medical librarian and search terms were coded for synonyms of ‘colorectal’, ‘colonoscopy’ and ‘qualitative studies’. The full search is available in Supplementary Material 1. The citations were downloaded from each database and imported into Endnote for duplicate removal.
Selection criteria
Articles were screened by three authors with a pre-specified selection criteria. Articles that included the opinions of patients after a colonoscopy procedure were identified to be of interest. With reference to the clinical guidelines from the American Society of Colon and Rectal Surgeons, 12 articles with a study population of patients aged over 45 were included. Qualitative or mixed method studies such as semi-structured and focus group narratives were considered, but inclusions were limited to those in English and original peer-reviewed articles, excluding commentaries, conference abstracts and editorials. Thereafter, a full text review of the articles was conducted by independent pairs, with consensus reached via a third author when disagreements occurred.
Data extraction and synthesis
Data extraction was conducted through a structured pro forma on the 11 included studies. The study characteristics (location, year, sample size, age, gender, setting, population of study), methodology and primary findings of results were organized in a separate datasheet. The individual codes which spanned the experience of patients during the initial screening process, during the conduct of the procedure and post-procedure were first analysed and compared for similarity to form broad descriptive themes. The extracted codes were then thematically organized to develop new hypotheses beyond that of the primary literature. 13 Data relating to surveillance colonoscopy were excluded. All three authors met for discussion with qualitative experts to reach a consensus and further refine the final themes. Despite the variances in geography, sample size, setting and healthcare systems, the findings were found to be thematically consistent.
Quality assessment
Quality assessment of included articles was undertaken through the Critical Appraisal Skills Programme (CASP). 14 The CASP tool is recommended by the Cochrane Qualitative and Implementation Methods Group to assess the quality of an article on the domains of the clarity of its aims, the corresponding conformity with the research design, suitability of the sampling and data collection methods, and the validity of the results. 15 Each included article would be scored as ‘good’, ‘adequate’ or ‘poor’ based on its methodological quality and limitations. CASP was undertaken by two independent authors, with consensus reached through a third author. Considering the difficulty in qualitative appraisals, 16 the CASP results did not influence the exclusion of any articles. Rather, they were used to enhance the rigidity of the synthesis. 17
Results
A total of 3282 articles were collated after duplicates were removed. Following that, the records were screened individually, and a further 2916 papers were excluded based on failing to meet the criteria of being a peer-reviewed qualitative article or being colonoscopy centric. Forty-six articles were found to meet the inclusion criteria in the full text review and a total of 11 articles were included in the final analysis (Figure 1). The eligible articles incorporated the opinions of patients who were symptomatic 18 (n = 1), asymptomatic 19 (n = 1), from both groups20–23 (n = 4) and those whose status was unknown24–28 (n = 5). All participants did not have a diagnosis or personal history of CRC prior to the study. A phenomenological method of inquiry was adopted, by conducting either focus group discussions (n = 7) or interviews (n = 4) in various settings (e.g. hospitals, primary care clinics, offices, etc.). A summary of the included articles can be found in Table 1. Most included articles had minor methodological limitations. The individual scoring of CASP and the tabulated score of all included articles can be found in Supplementary Materials 2 and 3, respectively.
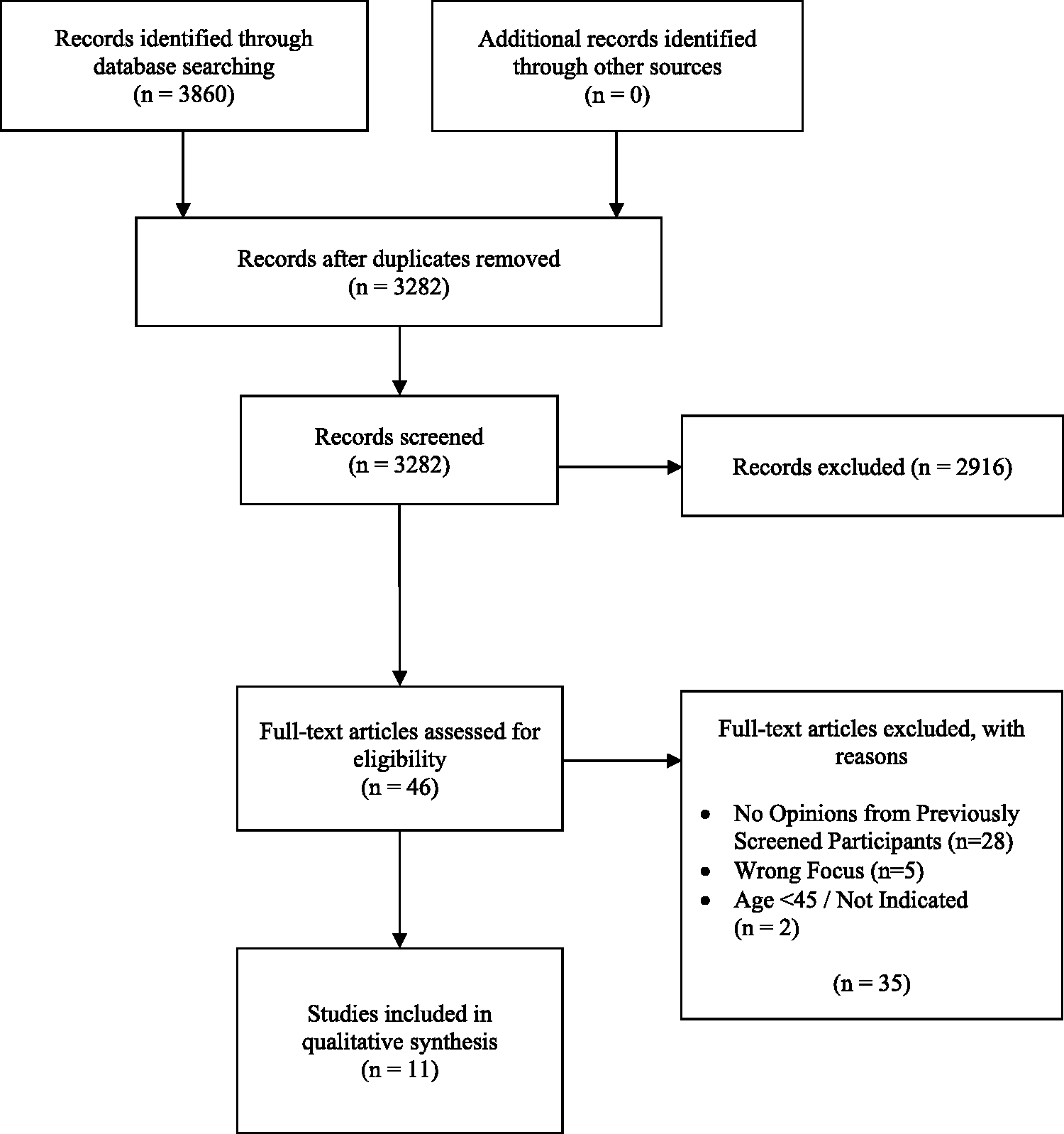
PRISMA flowchart of systematic review. A total of 2916 articles were removed during title abstract screening for lack of qualitative approaches in methodology (n = 459), lack of focus towards colonoscopy procedure (n = 2436), commentary, editorial and abstracts (n = 21).
Summary and characteristics of included articles in systematic review.
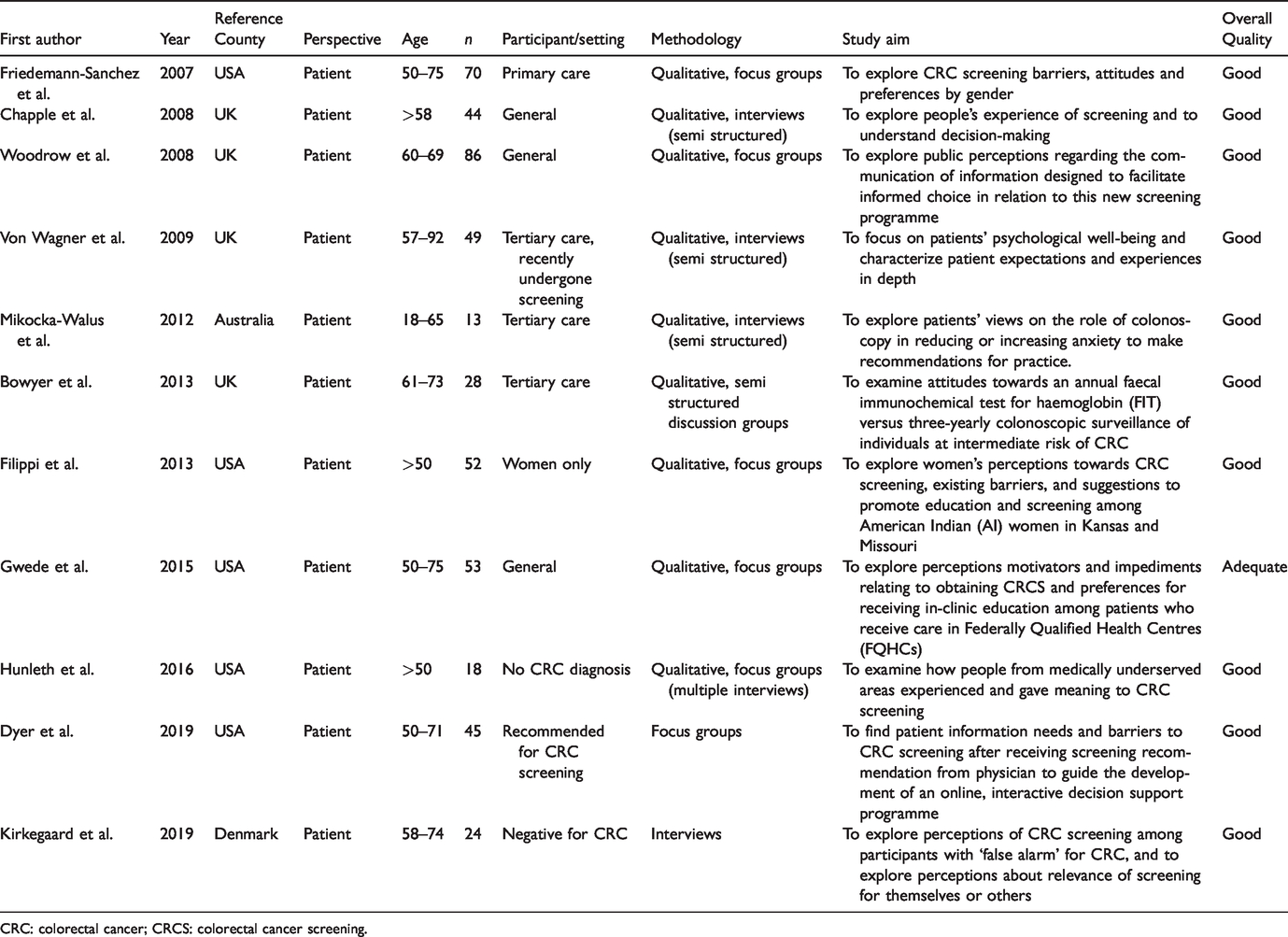
CRC: colorectal cancer; CRCS: colorectal cancer screening.
The findings describe views that are essential in determining a patient’s willingness to procure a colonoscopy in the future, following the completion of their most recent experience. The major analytical themes were segmented into three main categories: pre-procedure, during the procedure and post-procedure. The pre-procedure experiences of patients were around the bowel preparation required for a colonoscopy, the quality of information provided and the role a support network plays. Perceptions relating to pain, emotional discomfort and the role of providers are detailed as part of the experience during the procedure. The receipt of the results, discussion and finances related to colonoscopy are elaborated on as the post-procedure experience.
Pre-procedure
Bowel preparation
The bowel preparation required before a colonoscopy posed a challenge to working adults, given that a two days leave of absence may be required for the preparation and procedure itself. 21 It is also disruptive for patients with chronic illnesses to halt their medication regimen. 24 Patients expose themselves to risk by trying to comply with taking laxatives and adhering to a strict diet, while continuing work. 26 Instead, patients may opt for a faecal immunochemical test (FIT) to circumvent the troublesome bowel preparation. 23 The laxatives were viewed as repulsive, unreasonable in volume and abusive even, compared to the actual colonoscopy, which was cited to be simple. 24
Information
The information provided about CRCS was perceived to be overtly general and unhelpful in aiding a patient to make well-informed healthcare decisions. 26 This can cause misconceptions such as the belief that CRC only affects male patients 24 and that colonoscopy is less accurate than an annual FIT. 21 , 23 Such misunderstandings discourage the uptake of colonoscopy. 23 For women, this is worsened by fragmented healthcare information that stresses the importance of breast and cervical cancer screening, but leaves out information about CRCS. 22 , 24 However, providing a general overview prior to consent-taking was appreciated, as it empowers patients to be well-informed of the process 27 and possible consequences. 21
Support network
A support network constituting family and friends facilitates the dispelling of fear and stigma to encourage the uptake of the procedure. 22 However, in follow-ups, social networks serve as a source of pressure for individuals who opted to receive a colonoscopy in order to avoid being a subject of sympathy and conversation. 22 , 26 , 27 On the other hand, the loss of friends who succumbed to CRC despite having a colonoscopy seeds doubt about the effectiveness of the procedure and discourages uptake. 20 Another challenge encountered in the preparatory phase is accommodation to the requirements of the procedure. Patients who are unable to find a relative or friend to escort them may be ineligible for sedatives during colonoscopy. This may be a reason for dismissal of the procedure altogether. 18 , 19 , 28 Some patients undergoing burdensome life events reorder colonoscopy to be of lesser priority compared to the more pressing issues such as the termination of employment or divorce. 26 This makes it difficult for patients to follow through with an appointment. 18 , 19
During the procedure
Pain
Pain is commonly experienced by patients 18 , 24 , 27 , 28 and can lead to colonoscopy being remembered as rough and unacceptable. 20 , 24 A patient recounted his experience as being traumatic, as it crushed the positive spirit he initially had. 20
The administration of a sedative is often the solution to address discomfort. 18 While colonoscopy was initially perceived to be invasive due to the risk of perforation and pain, 19 , 24 , 25 patients who had received a sedative were pleasantly surprised post-procedure and remarked that their initial anxiety and fears were irrational and unfounded. 19 , 22 These patients considered their experience as easy, fast and acceptable, 19 , 22 , 27 with the benefits taking precedence over any physical discomfort. 25 One reported that they only had to allow themselves to be eased into sleep through the administration of the sedative and be woken up a few moments later to the completion of the procedure. 19
Emotional distress
Humiliation, embarrassment and depression were commonly felt, because patients had to be unclothed or worked on in a private region of their body. 19 , 20 , 22 This emotional distress was frequently expressed by female patients who felt their dignity was violated, compared to male patients who viewed the invasive nature and the sexual connotation 19 , 20 associated with the procedure with disdain. 19 , 24 The anxiety experienced led patients to dread future colonoscopies, in fear of experiencing similar distress, being unconscious or even death. 19 , 20 , 22 The desire of patients to be independent and in control can lead to an exacerbation of these negative emotions, given the helplessness one feels being on the receiving end of the procedure. 22 Having experienced the procedure, patients anticipated a less daunting and a better experience moving forward. 22
Rapport with providers
Providers play a direct role in determining the experience of a patient. Patients appreciated being made aware of the proceedings though a live commentary during the colonoscopy. 24 Some welcomed doctors showing them the video feed from the colonoscope during the procedure, citing that it was reassuring, entertaining and a good distraction. 18 , 24 However, reactions varied, and a few avoided looking at the explicit images onscreen. 18 , 24 The opportunity to be actively involved and converse with the doctor during the procedure allowed patients to feel valued and respected as equals. 28 The behavioural coping techniques advised by doctors or nurses assisted patients in feeling encouraged and relaxed, and also served to reduce pain. 22 , 24 The sensitivity of the staff through their words of affirmation, humour and physical acts of support, such as holding of the patient’s hand, was well-received and hoped for in future procedures. 18 , 24 Such care, understanding and professionalism fostered greater trust between patients and providers that can contribute to patient compliance with colonoscopy screening. 22 , 28 A lack of rapport between patients and providers is detrimental, resulting in patients feeling unheard and disrespected. 22
Post-procedure
Receipt of results
Sedated patients have marked gratitude when the outcomes of the colonoscopy are revealed during the recovery period. 18 Most patients were relieved to have benign or normal colonoscopy findings, and expressed joy in completing the procedure as a confirmatory test. 28 However, one perceived colonoscopy to be of no use to her, especially since the exclusion of bowel cancer left her frustrated and hopeless with regard to understanding the cause of her persistent symptoms. 22 However, this could have been an unrealistic expectation caused by an exaggeration of the protective effect of colonoscopy and the advancement of medical technology. 23 Results being made available through email is another facilitator for patients. 27
Post-procedure discussion
There was a desire for closer interaction with healthcare staff to discuss, explain and attend to inquiries. 26 The lack of thoughtful care coordination post-procedure can lead to feelings of distress, misunderstanding and even misinformation. 26 Patients were troubled by unexpected costs incurred from the procedure such as for the removal of additional polyps and further testing such as a tissue biopsy. 26
Finances
The hefty bill that comes with colonoscopy can restrict participation solely to affluent patients with insurance coverage, 26 especially in countries with a privatized healthcare system that is largely based on the principle of self-sufficiency, such as that in the United States of America. Insurance premiums are often expensive and have coverage that may not extend to future surveillance colonoscopy. 26 In such cases, the affluent can supplement their existing insurance with other private insurance plans. 26 However, financially disadvantaged patients resort to undertaking multiple jobs to avoid medical debt or gain access to company health insurance schemes. Other patients avoid colonoscopy until they are symptomatic. 26
Discussion
This systematic review summarizes current views of patients after their colonoscopy experience. More than half a century has passed since the conduct of one of the first documented colonoscopies and, despite the barriers and inconveniences, 29 colonoscopy remains the gold standard for CRCS. While studies to date have dissected the existing barriers against colonoscopy, minimal investigations have been made to understand the afterthoughts of patients post-colonoscopy. Those who had undergone a colonoscopy before experienced reduced pre-procedure apprehension of pain and discomfort as compared to colonoscopy-naïve patients. 19 , 22 There is a shift in the mindset of pain as a barrier, having experienced the procedure for themselves. Patients would even consider their initial anxiety and fears as irrational and baseless. 22 These findings sharpen the focus on measures that can be used to improve and increase repeat uptake of colonoscopy.
Many studies pertaining to colonoscopy focus on views irrespective of screening status. 30 As a result, although it is important to shed light on the general population’s impression of colonoscopy, the unique perspectives of patients who have undergone the procedure may often be marginalized when compared to the larger colonoscopy-naïve population. Among post-colonoscopy studies, a variety of factors arise, such that some reported psychosocial concerns and costs as the main barriers 26 while others reported rapport with physicians as the most significant facilitator. 18 , 22 , 24 To our knowledge, this is the first comprehensive review of the factors identified pertaining to perspectives after a colonoscopy.
The finances associated with a colonoscopy appeared to be a more prominent factor in countries with a privatized healthcare system, such as the United States. 26 However, the introduction of insurance schemes with broader coverage for various types of cancer screening led to no significant increase in cancer screening rates. 31 , 32 This is concordant with socialized healthcare systems, as in the United Kingdom, where screening rates remain low. 33 The limited effect of financial incentives to increase cancer screening rates 34 , 35 is indicative of the greater role that other factors play in encouraging cancer screening. A larger impact could be achieved by tackling these other concerns, many of which can be alleviated through the clear, concise and thoughtful delivery of information. This can be combined with technological advancements, by going beyond using scripted counselling to merely convey facts and moving into a collaborative method of discussion with patients. Animated graphics can be used to further enhance patient’s understanding before colonoscopy. 36 , 37 Patients who have watched a preparatory video reports less pre-procedure anxiety. 38 Additionally, easily accessible helplines can be utilized for patient to reach out to providers and have their doubts, insecurities and misconceptions addressed prior to the scheduled colonoscopy. Clarity of information provided, especially during risk counselling and when discussing other CRCS modalities prior to consent taking, plays a vital role in decision-making. Counselling information should always be personalized and contextualized to the needs of a patient. The timing for patients to receive the results of their colonoscopy is crucial. A patient’s emotional well-being should also be considered a priority by healthcare services. Patients should first be allowed to rest, then informed of the results and be given the opportunity to have their queries attended to post-colonoscopy.
Even with the most robust approaches to educate and counsel patients on colonoscopy, little can be achieved without good rapport between patient and providers. With high turnover rates at endoscopy units, healthcare provider–patient interactions tend to be overlooked. Empathetic care during the procedure generates trust and confidence in the experience. Providers should strive to build rapport through sensitive and empathetic interactions to ensure the comfort of patients. This can encourage patients to be unafraid in voicing their concerns and be soothing for those who experience feelings of embarrassment or violation. Most patients who were made aware of events during the colonoscopy or were talked through the video feed from the scope18,24 not only had a better understanding of the procedure, but also felt respected and informed.
With the expanding implementation of open-access colonoscopy, it is crucial to recognize patient-centred determinants to augment the sustainability of this modality. Empowering patients to personalize their colonoscopy may be the way forward in the effort to promote patient comfort during the procedure. This includes having the options of on-demand sedation, 39 virtual reality, 40 , 41 music therapy, 42 or other relaxation interventions.
Limitations
This review is limited by the linguistic ability of the authors, leading to the inclusion of only literature in English. The included articles largely arise from North America and the United Kingdom, which may limit the generalizability of the findings to each specific setting, especially in the Asia Pacific region. However, we hypothesize that the consensus of views should not be subjected to extensive variability and should still be coherent at large.
Conclusion
This afterthought review offers an unprecedented range of patient perspectives to help address colonoscopy adherence issues. The key areas of emphasis are perceived patient comfort, the use of clearer instructional aids such as graphics, the importance of patient rapport in this fast-paced era and providing individualized options for sedation and procedural steps. An overall need is identified for a holistic approach to improve colonoscopy adherence rates.
Supplemental Material
sj-pdf-1-msc-10.1177_0969141320923381 - Supplemental material for Afterthoughts on colonoscopy. Was it that bad?
Supplemental material, sj-pdf-1-msc-10.1177_0969141320923381 for Afterthoughts on colonoscopy. Was it that bad? by Glenn M Decruz, Cheng H Ng, Kia T Lim, M K Devi, Frances Lim, Chia H Tai and Choon S Chong in Journal of Medical Screening
Footnotes
Acknowledgement
We thank Ms Annelissa Chin, Senior Librarian, NUS Medical Library for her assistance and guidance on crafting the search strategy.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.