
Abstract
Objectives
Early diagnosis of biliary atresia is essential to improve long-term outcomes. Newborn screening with an infant stool color card allows early recognition of biliary atresia patients. Our aim was to develop and validate a mobile phone application (PopòApp) able to identify acholic stools.
Methods
An intuitive app was developed for iOS and Android smartphones. A learning machine process was used to generate an algorithm for stools color recognition based on the seven colors of the infant stool color card, which were considered as the gold standard. Consecutive images of stools were taken by the PopòApp, directly into the diapers of children aged ≤6 months. The PopòApp classified the photographs as “normal”, “acholic” or “uncertain”. To validate the PopòApp, four doctors independently classified all images, and only those for which all doctors agreed were included. The sensitivity, specificity, positive/negative predictive values, and accuracy of the PopòApp were evaluated.
Results
Of 165 images collected, 160 were included in the study. All acholic stools were recognized by the PopòApp. The PopòApp sensitivity was 100% (95% CI:93.9%–100%) with no false negatives, regardless of the brand of phone. The specificity was 99.0% (95% CI:94.6%–99.9%). The accurancy of the PopòApp was 99.4% (95% CI:96.6%–99.9%), with a positive predictive value of 98.4% (95% CI:89.8%–99.8%).
Conclusion
The current study proved, in a large cohort, that the PopòApp is an accurate and easy tool for recognition of acholic stools. The mobile App may represent an effective strategy for the early referral of children with acholic stools, and potentially could improve the outcomes of biliary atresia.
Introduction
Biliary atresia (BA) is the most common cause of neonatal cholestasis and pediatric end-stage liver disease, and the leading indication for pediatric liver transplantation (LT). 1 The incidence varies from 1/5000 to 1/18,000 in Europe and North America, 2 while reaching about 1/10,000 live births in Asian countries. 3 BA is a progressive disease affecting the biliary tract, characterized by a complete inability to excrete bile as the result of sclerosing inflammation of the bile ducts.4,5 Infants with BA are usually full-term babies in good general condition, developing jaundice, acholic stools, and dark urine within the first few weeks of birth. 4
Kasai portoenterostomy (KP) is the first-line treatment for BA consisting of a surgical procedure aiming to restore the bile flow from the liver into the intestines.4,5 Infant age at the time of surgery is one of the most important prognostic factors for successful outcome and strongly correlates with transplant-free survival.1,4,6,7
Unfortunately, diagnosis of BA is often delayed beyond the optimal timepoint for intervention because physiologic jaundice in newborns is extremely common, and differential diagnosis might be challenging.
Population-based screening using an infant stool color card (ISCC), which provides color images of stools ranging from cholic to acholic, can allow the identification of children with pale color stools who might have BA.8–10
The American Academy of Pediatrics (AAP) recently analyzed the cost-effectiveness of BA screening with ISCC and reported that it is associated with lower costs and improved outcomes compared with no screening. 11 However, the ISCC screening system requires an efficient collaboration of local practitioners nationwide with specialized centers, which might be difficult. 12
Due to advances in technology and the increased access to smartphones, in recent years the number of available health “Apps” has exploded, and mobile applications have gained a concrete role in healthcare systems. 13 Since 2015, some mobile phone applications have been developed which aim to recognize acholic stools,14–16 but further data are needed to confirm their clinical applicability in a larger cohort and the impact of the Apps on the early diagnosis of BA.
The aim of the current study was to develop and validate a mobile phone application (PopòApp) able to identify acholic stools according to the ISCC.
Material and methods
Software development
The PopòApp was developed in collaboration with Indra Italia Spa® and was established to work on iOS (version 11 or superior) and Android (version 4.4-KITKAT or superior) devices. The conceptual framework, user interface, and navigability were designed by a dedicated team composed of pediatric surgeons, hepatologists, and communication managers. For the iOS platform, Objective-C programming language was used, while Kotlin programming language was adopted for the Android platform. The PopòApp was developed in different languages, including Italian, English, and French.
User interface of PopòApp
The App was designed to target parents and caregivers, and consequently, its development aimed to be intuitive, intelligible, and reassuring. Through a touch screen interface, the user may open different pages including a description of the application’s objectives and utility, an explanation of BA disease and instructions on how to perform a photo shoot (Figure 1(a)). The App describes that its goal is to identify the acholic stools of infants in order to provide an early referral to a specialist center; moreover, a supportive message notifies the user that the PopòApp is not a diagnostic tool but a screening instrument. A notice summarizes the respect of personal information according to the privacy policy.
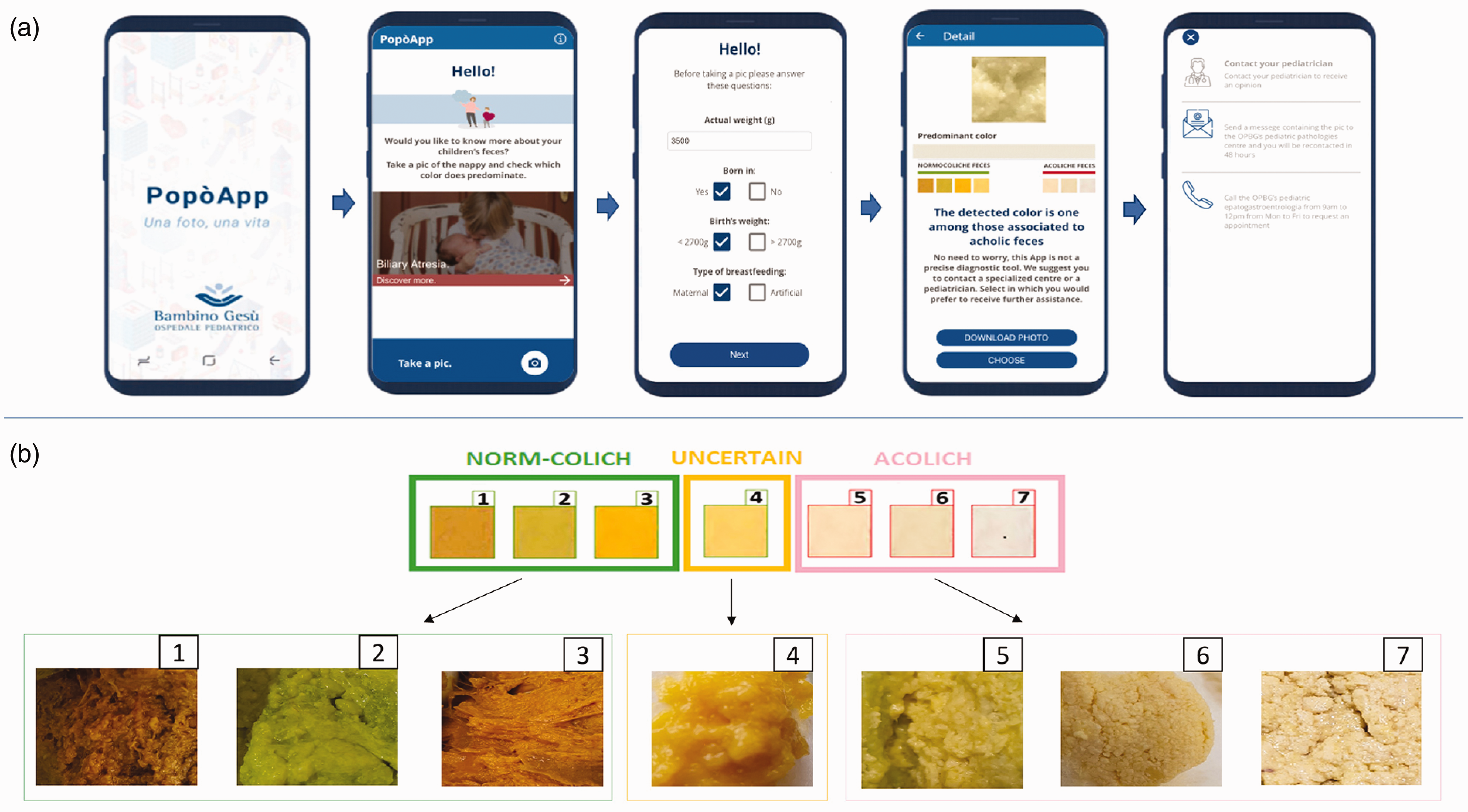
(a) PopòApp screenshots. Using a touch screening interface, the PopòApp provides an informational page explaining the biliary atresia disease and the propose of the mobile phone application. After a baseline questionnaire, the App invites the users to take a picture of the stools in the diapers using the mobile’s camera; then, the PopòApp displays the predominant color of the photo. When the App detects “acholic” stools, a screen message suggests to contact the pediatrician or a specialized center of whom a direct contact list is provided. An option bottom offers the possibilities to take a new photo shoot, to download the images into the smartphone and/or to directly send the phot by email imagines to a specialized center (pediatric hepatogastroenterology unit). (b) Samples of stools images performed by the PopòApp and classified by the mobile application according to the seven colors of the infant color stool card.
After a baseline questionnaire (age, weight, type of feeding), the App invites the user to take a picture of the stool in the diaper. Once the picture is taken, the PopòApp automatically analyses the color, displaying the predominant color of the photo. Based on the color classification, the App will provide a screen message notifying that stools are defined as “normal”, “acholic” or “uncertain”. Any color not classified by the App will be defined as “indeterminate”. An option is then available to either start a new photo shoot, download the images into the smartphone and/or send them to the reference center, which will review the photo and give feedback by email. When the App detects “acholic” stools, a screen message recommends that the user contacts the family pediatrician or a specialized center. The App also suggests retaking the photo in cases where “uncertain” or “indeterminate” colors are detected.
The App has been designed to collect patients’ data and stools’ images anonymously by a centralized server, remaining available for further analysis. When the user decides to send the images to the reference center, the App requires the user’s contact (email or phone) to be sent with the stool’s photos to the reference center.
Color analyzer algorithm
The CAA was developed with the programming language Java EE. The mobile App uses the digital camera with the color recognition software of the smartphone, without requiring arrangements for light exposure. The color detection algorithm was based on parameters as red, green, blue (RGB). To avoid the inclusion of surrounding colors, the App has an automated zoom-in function allowing it to focus the picture in the predominant color of the stools. A multiresolution algorithm was developed to find the dominant color, analyzing the most frequent RGB triplet at several resolutions and weighting the final color based on the most frequent color on each resolution. Also, a normalization algorithm was applied to compensate several illumination aberration scenarios as, for example, neon lights or incandescent yellow lights, in order to maximize the sensibility and sensitivity and to reduce the risk of false negative results. The CAA used a learning machine process which was able to improve the algorithm’s ability of color recognition.
The CAA was developed according to the previously validated 7-panel stool colors of the ISCC,10 which were considered as the gold standard for BA screening in Europe.12,17 After the colorimetric analysis, the App classified each stool’s color into a category from 1 to 7 defined by the ISCC. Using the newly developed neural network, the App defined the stools as “normal” for categories from 1 to 3, “uncertain” for category 4, and “acholic” for categories from 5 to 7 (Figure 1(b)). All other colors not included in the seven categories of the ISCC were classified as “indeterminate”.
Validation process of the PopòApp
Children aged ≤6 months admitted as inpatient in the Department of Hepatobiliary Surgery and Hepato-gastroenterology of the Bambino Gesù Children’s Hospital IRCCS were consecutively enrolled, and images of stools were taken using the PopòApp by four doctors (two pediatric gastroenterologists and two pediatric surgeons). Data were collected in an anonymous prospective database.
After the photo shoot, the App classified the images based on the seven categories of the ISCC, and photographs were memorized. Then, stools were independently classified by each doctor, without knowing the categorization of the App and the diagnosis. Only the doctor that took the picture saw the stool sample, while the others reviewed the photos saved in the database.
Results of the doctors’ classifications were recorded and compared with those obtained from the App. Only images for which all four doctors agreed on the color classification were included in the final analysis.
Statistical analysis
To assess the accuracy of the application in recognizing acholic stools, we analyzed the sensitivity, specificity, positive predictive value, negative predictive value, and accuracy for each category (cholic, uncertain, acholic, and indeterminate) and for each color (1–7, N/A), along with 95% confidence intervals (CI). This study was conducted following the STARD criteria. 18 .
Ethics statement
This study involved the use of de-identified photographs and was approved by the Bambino Gesù Children’s Hospital IRCCS Istitutional Rewiew Board (ref. number: 1839_OPBG_2019).
Results
Between January and November 2019, 165 photos of infant stools were taken using the PopòApp. Five photographs were not included in the analysis because of a lack of agreement in color classification between all doctors. Therefore, 160 photos were enroled in the analysis, for which all doctors gave the same color classification.
Study population
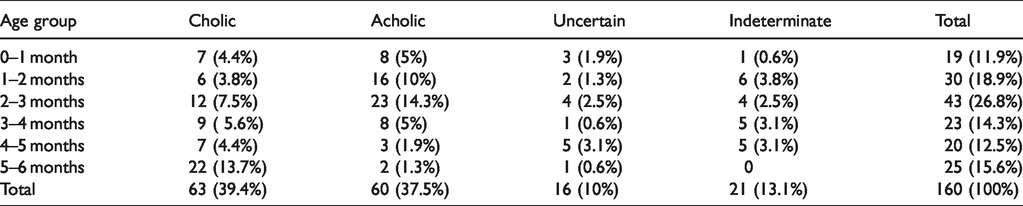
The median age of children enrolled was 2.7 months (range:15 days–6 months). Of 160 children, 19 (11.9%) were less than 1 month of age, 30 (18.8%) were between 1 and 2 months, 43 (26.8%) between 2 and 3 months, 23 (14.4%) between 3 and 4 months, 20 (12.5%) between 4 and 5 months, and 25 (15.6%) between 5 and 6 months.
Acholic stools were more frequently detected in infants less then 3 months of age (78.3%) as detailed in Table 1. All patients with acholich stools were diagnosed with BA, except two patients who presented Alagille syndrome and Progressive Familiar Intrahepatic Cholestasis type-2. Among children with colic stools, the majority were admitted for infectius disease (enterocolitis, bronchiolitis, diarrhea), while five of them presented unlying liver disease including two cases of hepatisis associated to neonatal sepsis, one metabolic liver disease, one liver hemangioma, and one transient hypertransaminasemia.
Distrubution of stool colors according to the age of children.
Sensibility and specificity
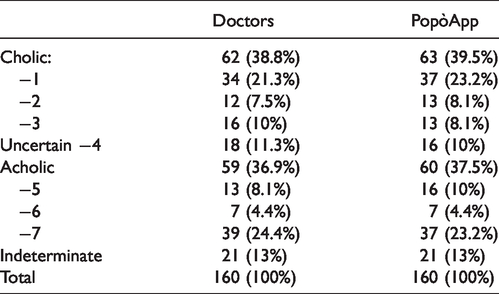
In 62 cases, the images were classified as cholic by doctors, while the PopòApp identified 63 diapers with cholic faeces. In 18 cases, the color of the stool was defined as uncertain, whereas the PopòApp placed 16 samples in this category. Doctors then identified 59 photos with acholic faeces (13 in category “5”, 7 in category “6” and 39 in category “7”), compared to 60 images recognized in this category by the PopòApp (16 in category “5”, 7 in category “6” and 37 in category “7”). In 21 cases, the doctors and the PopòApp classified the color of the stool as indeterminate (Table 2).
Stools classification by doctors and PopòApp.
The overall PopòApp sensitivity was 100% (95% CI: 93.9%–100%) with no false negatives. The specificity was 99% (95% CI: 94.6%–99.9%). The accuracy of the PopòApp in identifying acholic stools was 99.4% (95% CI: 96.6%–99.9%), with a positive predictive value of 98.4% (95% CI: 89.8%–99.8%). The diagnostic test evaluation for each category and color is detailed in Table 3. All acholic stools were recognized by the PopòApp and classified in accordance with doctors’ evaluations. Only one stool photo was defined as an “indeterminate” color by doctors and classified as acholic by the mobile application.
Accurancy of PopòApp.
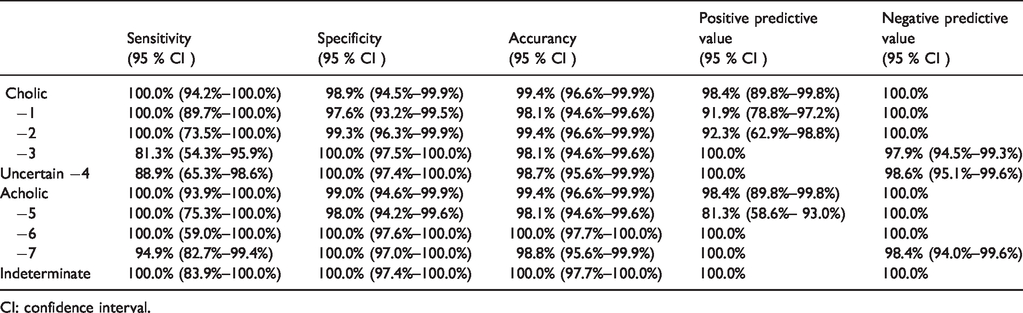
CI: confidence interval.
In the sub-group of infants less than two months of age, the sensibility, and specificity for detecting acholic stools were 100.0% (95% CI: 85.8%–100.0%) and 100.0% (95%CI: 97.3%–100.0%) respectively, with accuracy of 100.0% (95% CI: 97.7%–100.0%); for the group < 3 months of age, the sensitivity was 100.0% (95% CI: 92.5%–100.00%), the specificity was 100.0% (95% CI: 96.79%–100.0%), and the accuracy was 100.0% (95% CI: 97.7%–100.0%).
Both iOS and Android devices correctly identified all acholic stools with a sensitivity of 100% (95% CI: 91.6%–100%). Using the Android device, the PopòApp identified acholic stools with a specificity of 100% (95% CI: 92.6%–100%) and an accuracy of 100% (95% CI: 95.9%–100%). For the iOS mobile phone, the specificity was 98.1% (95% CI: 80.5%–100%) and the accuracy was 98.6% (95%CI: 92.3%–100.0%) in detecting acholic stools.
Discussion
BA causes progressive liver failure and death within two years of life if untreated. 19 The KP is the first treatment of BA and its outcomes improve if performed within two months of age. 20 In children with late BA diagnosis or undergoing unsuccessful KP, LT represents the only curative option and BA is the most common indication to pediatric LT.21 Whilst nowadays long-term patients’ survival after pediatric LT for BA approaches 95%, transplantation is not a risk-free procedure and is associated with mortality and morbidity.22,23 Moreover, the organs’ viability and the access to liver transplant programs are not uniform worldwide; in Italy, the pediatric LT waiting-list mortality is about 2.5%, 24 thus it ranges from 7 to 12% in US.25
In the last decade, BA screening has been proposed, based on the recognition of the two most important signs present early in the disease, consisting in acholic stools and elevated bilirubin plasma levels. 26
The major national BA screening programs were developed in Taiwan and Japan, and both demonstrated that the use of ISCC is an efficient method for the early diagnosis of BA and is associated with improved outcomes.8–10 In Taiwan, the introduction of ISCC screening was related to a significant reduction in the average age at KP (from 65.9 to 46.9 days) and improvement of overall BA mortality (from 70% to <20%). 27 In Japan, a case-control study demonstrated that the probability of native liver survival is superior for ISCC users. 28
BA screening with ISCC was also applied in other countries, such as China, 29 British Columbia, 30 Canada, 31 and Germany. 12 Although all reports demonstrated the utility of the early diagnosis of BA by acholic stool recognition, the use of ISCC has not yet become universal due to the complexity of the setup of a newborn screening program and its associated costs. Moreover, in countries where the ISCC is not obligatory, the screening program requires active collaboration from local practitioners, which is often lacking in voluntary studies (e.g. only 20% of local practitioners’ adherence in Germany). 12 Another limitation is related to the fact that when ISCC are distributed directly to parents at the neonatal center, they might be not re-evaluated by doctors, with the possible consequence of misrecognition of the disease.
As an alternative screening system for BA, other series reported the efficiency of regular blood sampling of bilirubin plasma level in newborns,32–34 but its use is limited due to the recurrent traumatization for the infants. 26
To overcome the limitations of the screening systems based on ISCC or blood sampling, in 2015 the Johns Hopkins University group firstly developed a mobile phone application (PoopMD), 14 able to identify acholic stools according to the color ranges of the Taiwan ISCC with a sensitivity of 100% and specificity of 89%. The excellent results of the PoopMD opened new horizons for non-invasive BA screening; however, this study was based on a small-sample of photos (34 images) and excluded colors ranging from red to black (i.e. from gastrointestinal bleeding) with the consequential restriction of its use to all varieties of color.
In another study, the saturation in HSV (H-hue; S-saturation; V-value) was shown to be an important parameter for the recognition of acholic stools with a sensitivity of 100% but a specificity of 85% which is not ideal, especially for stools of dark green color (that might reflect a high concentration of bile pigment). 15
Recently, Hoshino et al. 16 integrated a stool color evaluation system, developed for mobile devices with pattern recognition and a machine learning process, into a new mobile App (Baby Poop). Baby Poop App was able to correctly identify five BA stools with 100% accuracy in a sample of 40 pictures, although all images analyzed were taken from a pre-existing collection of pictures and, consequently, some variables related to the photo shoot, such as the brightness of exposure, could not be tested. Moreover, the App was tested only in iPhone devices, and is not available for other smartphone brands.
In the current study, we developed the first free application for mobile devices (PopòApp), which integrated all stool color evaluation systems previously developed with the aim to recognize the color of infant stools in a large cohort of samples. To include all type of stool colors and to test different light exposures, new images of stools were consecutively taken by the PopòApp from all children younger than six months admitted in our departments during a nine-month period, without exposure adjustments. The PopòApp accuracy was tested on 160 photographs, which represents the largest cohort of images collected using an App (Table 4).
Mobile device applications with stool color recognition systems for biliary atresia screening.
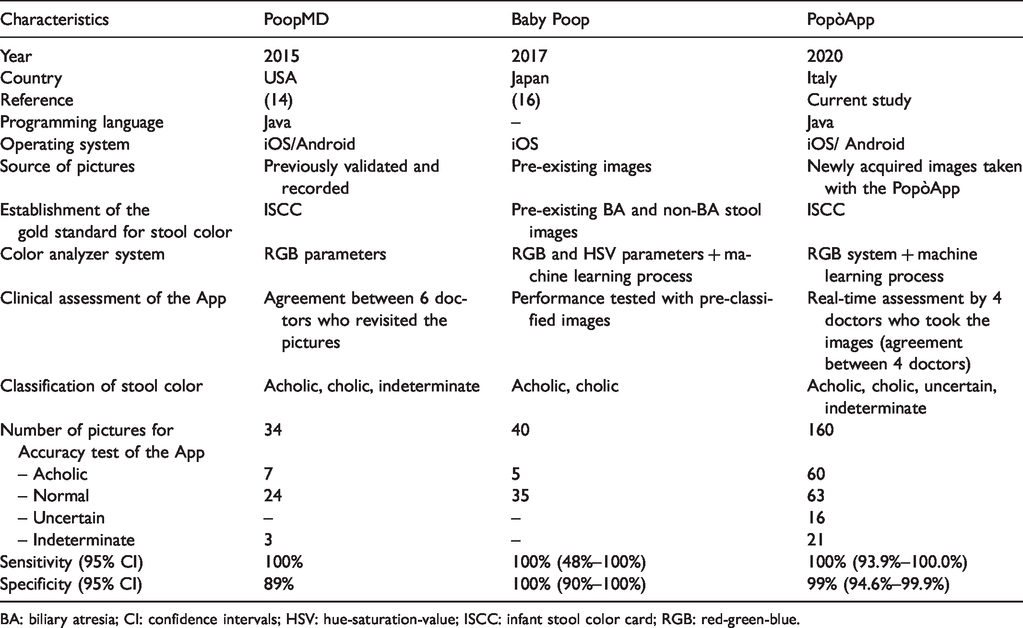
BA: biliary atresia; CI: confidence intervals; HSV: hue-saturation-value; ISCC: infant stool color card; RGB: red-green-blue.
The CAA of the PopòApp involved the development of an algorithm for color recognition with a machine learning process based on the colors of the ISCC, which are considered as the “gold standard” for recognition of infant stools.10,17 For the clinical assessment of the PopòApp, pictures were classified directly by doctors, blind to the infants’ diagnosis, and images were only included in the analysis when four doctors all agreed on the classification, considered as a benchmark for the classification. The color analyzer system of the PopòApp showed a sensitivity of 100% and a specificity of 99% in recognizing acholic stools, which is in line with values obtained by the ISCC9–11 or the bilirubin sample levels.33,34
Compared to the previous mobile device applications for BA screening, the PopòApp showed similar accuracy but in a larger series. Moreover, our study is the only one to date that included new images taken directly by the mobile phone application (not involving pre-existing pictures). The PopòApp is already set for its large-scale distribution and is available for all types of smartphone brand without requiring special arrangement (i.e. exposure, distance) to take the pictures. All acholic stools were recognized either by iOS or Android devices, thus Android phones had higher specificity (100% vs. 98.1%) probably related to its better resolution in low-light settings.
Since the aim of this study was to determinate the accuracy of the application in recognizing acholic stools, the future step is to evaluate its clinical impact on early diagnosis of BA. In the current era, where smartphones are largely diffused and there is a tremendous spread of health applications, our results confirmed that the mobile device application for BA screening represents an effective and promising instrument for a mass screening program, overcoming the limitation of ISCC distribution and the invasiveness of plasma bilirubin dosages. Compared to the ISCC, the mobile App for acholic stools recognition has the advantage of being an easy instrument that parents can directly download into their smartphones and use without any education; pictures can be taken every time they are required and immediate results are provided by the application without waiting for the images to be reviewed by local practitioners. For clinical use, when acholic stools are detected, the PopòApp invites parents to early refer to the pediatrician or to the specialist center, providing direct contacts and reducing the time to diagnosis and treatment; moreover, an alert is sent to specialist center which could contact directly the patient.
However, the absence of a smartphone in a family could potentially compromise a screening program; for the few parents not using smartphone (5% at 30–44 years in Italy 35 ) other family members owing the device or the pediatrician, during the ordinary visits, could perform the screening.
As our purpose was to define the accuracy of the PopòApp in recognizing the color of infant stools, we enrolled children ≤6 months in order to include all variety of stool colors from children breastfed. However, in future screening program, the application should be used in infant < 2 months of age to achieve an early diagnosis and a correct time for KP.
The use of mobile application in BA screening program could be potentially cost-effective even more than the ISCC.11,30 A report from the British Columbia 30 accurately, described the costs for the first two years of the BA screening program using ISCC, amounting for a total of 110.199$ and 0.68$ per birth. Of these, 50% of costs are required for printing/translating the cards and to setup reminder tool to recap parents to analyses their child stool. Differently, the BA screening programs using the App would not require the costs related to print the ISCC, to translate the cards in different languages and to setup reminder QR codes.11,30 The App automatically sends to the device a weekly remind to perform photos if stools’ images are not taken. The expected expanses using the App, as tool in a screening program, include the setup of a service for the App management and update in addition to educational program for healthcare providers. Thus, further studies are required to define the costs of screening programs with the App.
As our study confirmed that the mobile device App for stool color recognition is an accurate instrument to identify acholic stools in a large cohort, further efforts should be made to bring the technology to the clinic in large scaled population-based programs for BA. In clinical practice, mobile App could favor the diffusion of BA screening programs worldwide.
Footnotes
Authors’ contributions
Roberta Angelico – Research design, wrote the manuscript, analysis and interpretation. Daniela Liccardo – Research design, wrote the manuscript, interpretation. Monica Paoletti – Data collection and analysis. Andrea Pietrobattista – Data collection, analysis and interpretation. Maria Sole Basso – Data collection, analysis and interpretation. Antonella Mosca – Data collection, analysis and interpretation. Samira Safarikia – Data revision, analysis and interpretation. Chiara Grimaldi – Data collection, analysis and interpretation. Maria Cristina Saffioti – Data collection, analysis and interpretation. Manila Candusso – interpretation, intellectual content, review accuracy and integrity of the work. Giuseppe Maggiore – interpretation, intellectual content, review accuracy and integrity of the work. Marco Spada – Research design, analysis and interpretation, intellectual content.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The development of the PopòApp was supported by the “Associazione Nazionale Italiana Bambini Epatopatici Cronici”. The authors received no financial support for the authorship and/or publication of this article.
Patient consent
Informed consent was obtained from the patient for publication of their information.