
Abstract
Objective
Biliary atresia (BA), a leading cause of paediatric liver failure and liver transplantation, manifests by three weeks of life as jaundice with acholic stools. Poor outcomes due to delayed diagnosis remain a problem worldwide. We evaluated and assessed the cost-effectiveness of methods of introducing a BA Infant Stool Colour Card (ISCC) screening programme in Canada.
Setting and Methods
A prospective study at BC Women’s Hospital recruited consecutive healthy newborns through six incrementally more intensive screening approaches. Under the baseline “passive” strategy, families received ISCCs at maternity, with instructions to monitor infant stool colour daily and return the ISCC by mail at age 30 days. Additional strategies were: ISCC mailed to family physician; reminder letters or telephone calls to families or physicians. Random telephone surveys of ISCC non-returners assessed total card utilization. Primary outcome was ISCC utilization rate expressed as a composite outcome of the ISCC return rate and non-returned ISCC use. Markov modelling was used to predict incremental costs and life years gained from screening (passive and reminder), compared with no screening, over a 10-year time horizon.
Results
6,187 families were enrolled. Card utilization rates in the passive screening strategy were estimated at 60–94%. For a Canadian population, the increase in cost for passive screening, compared with no screening, is $213,584 and the gain in life years is 9.7 ($22,000 per life-year gained).
Conclusions
A BA ISCC screening programme targeting families of newborns is feasible in Canada. Passive distribution of ISCC at maternity is potentially effective and highly cost-effective.
Introduction
Biliary atresia (BA), a potentially lethal liver disease of unknown aetiology, is the most common cause of paediatric liver related death and the leading indication for liver transplantation in paediatrics.1–3 Incidence in Canada is 1/19,000 live births (22–25 new cases per year), a rate comparable with that in the United States and Western Europe, but lower than in Taiwan (1.25/10,000). 4 The cardinal clinical disease feature, presenting by the third week of life, is persistent jaundice due to a conjugated hyperbilirubinaemia, with pale acholic stool, in an otherwise thriving neonate. Standard treatment is hepatic Kasai portoenterostomy (KP) to alleviate the obstructive jaundice and preserve the native liver. Liver transplantation is reserved for those with failed initial KP, those presenting late with decompensated liver disease where the initial KP is contraindicated, or those post KP who, at an older age, still progress to cirrhosis. Without surgical intervention, all infants with BA will die by age three years.
The most important prognostic factor for a successful KP outcome is the infant’s age at the time of the KP.1,5 The older the infant, the less likely it is that the KP will be successful, rendering the infant in urgent need of liver transplantation to ensure survival. In Canada, almost 20% of BA infants have their KP at >90 days, due to late recognition and diagnosis, with a subsequent 4-year native liver survival of 33%. 4 Delays in timely BA detection and intervention with poor native liver survival have been reported worldwide.4–11 Following the introduction of a universal BA screening programme in Taiwan using an infant stool colour card (ISCC), no infant had a KP at >90 days old and the 5-year post KP native liver survival has improved from 37% to 64%.12,13,14
While the ISCC BA screening programme has proven success in Taiwan, its feasibility in other populations, where lower disease prevalence rates reduce the proportion of affected children among those with a positive test, and with differing public health care systems and policies, has not been studied. A cost-effectiveness analysis of a home-based BA screening programme has never been performed.
The primary aims of our study were to assess the practicability of initiating a home based ISCC screening programme for BA in Canada, and to determine its cost-effectiveness.
Methods
The study was approved by the University of British Columbia and Hospital Institutional review boards.
Study design
Study design and enrolment.

Outcome of intervention strategies.

N/A: not ascertained.
Study population
Healthy newborns discharged within two weeks of birth from BC Women’s Hospital, Vancouver, British Columbia, between 1 December 2010 and 31 December 2011 were eligible, including those who required phototherapy. Newborns who remained in hospital longer than two weeks due to neonatal complications were excluded, as we anticipated that they would be closely followed by specialized health care providers. We did not expect any variation of the characteristics for healthy newborns or their respective families through the study period, and therefore considered the groups of families consecutively recruited to be comparable. The opt out consent system ensured that parents could withdraw from further participation in a next step intervention strategy at any time.
The Infant Stool Colour Card (ISCC)
The ISCC contained general information about BA, instructions on how to use the card, and a series of six photo images of different stool colours: #1–3, abnormal stool colours pale yellow to white; #4–6, normal stool colours, golden yellow to green (Figure S-1; available online). The photo images were identical to those validated in Taiwan (provided by Dr. Mei Hwei Chang). 13 The ISCC and all study information were available in the five most common languages spoken by mothers delivering at BC Women’s Hospital. At the time of discharge from maternity, all parents or guardians of eligible newborns were given a study package containing the ISCC and a letter detailing information about BA and the study. A toll free telephone number was provided for general enquiries and emergencies.
Screening strategies
An incremental approach was used to assess different strategies designed to increase the return and utilization of the ISCC (Table 1). Each strategy was planned to continue for one to two months.
Step 1 was passive distribution, whereby the study package was issued to eligible families at the time of discharge from the maternity ward. A few weeks prior to the study launch, educational and training sessions were provided to every nurse and unit clerk on the five maternity wards. The discharge nurse, using a standardized “study script”, briefly reviewed the study protocol: Parents were instructed to observe their infant’s stool colour at home daily for the first 4 weeks after birth and to compare the stool colour with the photo images on the ISCC. At 4 weeks post birth the parents were to assign a numerical grade to their infant’s stool colour and mail the self-addressed, postage paid card to the study centre. If at any time an abnormal stool colour was recognized during the first four weeks, the parents were instructed to complete the card and immediately return it by mail/fax, or to contact the study centre. The infant was then referred for diagnostic evaluation with confirmed BA cases having a KP arranged in an expedited manner. Step 2 involved step 1, with the addition of a reminder letter and ISCC mailed to the family in the third to fourth week after the infant’s birth. Step 3 was identical to step 2, except that a scripted telephone call was made instead of a mailed reminder package. At step 4, in addition to steps 2 or 3, an information letter and an ISCC were mailed to the infant’s health care provider in the fourth week after the infant’s birth. The health care provider was asked to complete and return the ISCC by the routinely scheduled first vaccination office visit at the eighth week. At step 5, in addition to step 4, a reminder telephone call with a scripted message was made to each physician’s office in the sixth week after the infant’s birth. Step 6 returned to the initial “passive” strategy, 8 months after its launch, to determine whether there was any temporal effect influencing the card return rate established in step 1.
Family telephone survey to determine card utilization
A sample of 100 English-speaking families who had not returned the ISCC in each of steps 1–3 was selected using a random number generator for a telephone interview conducted 3–4 months after the end of the specific screening strategy. Trained staff used a semi-structured questionnaire to determine whether families utilized the ISCC despite not returning it.
Cost-effectiveness analysis
A combined decision tree and Markov model was constructed using TreeAge DATA Pro (TreeAge Software Inc., Williamstown, Mass). The decision tree component represents short-term clinical pathways and the Markov additions represent processes that evolve over time (Figures S-2 and S-3; available online). 15 The model structure was informed by existing literature, and discussions with clinical experts who advised on the clinical pathways of a child with BA. The model simulates a cohort of newborns (born over a 12 month period) and follows that cohort over a 10-year time horizon.
To model the screening programme (Figure S-2; available online), a distinction was first made between true BA positive and negative cases. Uncertainty was then considered in terms of parents’ use of the card and, if the card was used, the return rate. When an abnormal stool colour is identified, the model assumes that there is a paediatrician visit, as well as laboratory and further diagnostic tests to determine whether the child has BA. All BA positive children are considered for a KP. Reasons for not having the procedure include progressive liver disease and signs of liver decompensation from the late detection of BA or other contra-indications to surgery. 10
For those children with false positive test results, a distinction was made between transient or durable stool colour changes. For both, a paediatrician visit is required, followed by further diagnostic tests when the colour change is durable. Newborns in this latter group are likely to have another liver condition, but subsequent costs are not assigned to the BA screening programme, on the assumption that the other liver condition would have been uncovered irrespective of the BA screening programme.
The Markov component of the model (Figure S-3; available online) consists of six states. BA patients who do not receive a KP move immediately to the ‘awaiting first liver transplant’ state. Driven in part by available data and clinical considerations, a one-year cycle length was chosen.
Data Inputs
To populate the model with data, we first made use of data from the associated clinical research. Where such data were unavailable, we used published data or input values from expert opinion (Tables S3, S4, and S5, available online). Age and sex specific annual probabilities of dying were derived from Canadian life tables, to reflect underlying mortality. 16
Card utilization rates were estimated using our study results. Because the study was conducted over a limited time frame, with low incidence of BA, we expected a very small number of BA positive cases to be observed. The card return rates and the associated sensitivity and specificity estimates were therefore taken from the Taiwanese study, which implemented a similar BA screening programme. 13 Costing was performed using the publicly-financed health care system and so out-of-pocket patient costs were not considered. Costs, discounted at 5%, are reported in 2011 Canadian dollars (Table S6; available online).
Outcome measures
A primary outcome measure was the ISCC utilization rate. This was derived as a composite of the actual ISCC return rate and the rate of family use of non-returned ISCC, based on the telephone surveys. The total ISCC utilization rate in a given strategy was calculated as the [percent of families who returned the ISCC] + [percent telephone survey ISCC utilization][percent of families who had not returned the ISCC]. For cost-effectiveness, the outcome measure was the incremental cost-effectiveness ratio (ICER) calculated for each screening strategy. The ICER is the difference in the costs divided by the difference in effects (life-years gained). Initially, passive screening was compared with no screening, and then passive screening supplemented with a reminder was compared with passive screening. In judging cost-effectiveness and value-for-money, a willingness to pay threshold of $50,000 per life-year gained was assumed.
Statistical methods
Statistical comparisons between screening strategy cohort ISCC return rates were assessed using Chi square tests. A sensitivity analysis was conducted to determine a “best” and “worst” case scenario of the percent telephone survey ISCC utilization. The most conservative approach assumed that those who did not participate in the telephone survey did not use the ISCC (percent telephone survey ISCC utilization= [N who stated they used the card/ N of the total randomly selected for telephone interview]). The most optimistic approach determined the percent telephone survey ISCC utilization based on the responses of those who actually participated in the telephone survey (percent surveyed who utilized the ISCC= [N who stated they used the card / N of the total families actually interviewed]). All significance tests were two tailed with α fixed at 0.05. All statistical analyses were performed with R software (2.14.0).
For cost-effectiveness, a probabilistic analysis was run for the base case, applying relevant distributions to model parameters: a beta distribution for binomial data and a Dirichlet distribution for multinomial data. 17 Through Monte Carlo simulations (sampling 10,000 times), values were selected at random from the assigned distributions. The expected costs and life-years gained estimates were applied to the Canadian population, assuming 381,400 births per annum. The results, therefore, indicate costs and survival gains accrued over a 10-year period for a single cohort of newborns screened over a 12 month period.
Results
There were 6,843 births during the one-year study period, and 6,187 (90%) families were enrolled into the study. Of the cases excluded, 211 were directly admitted to a Neonatal Intensive Care Unit, 382 were improperly registered, 46 cases had remained in the regular nursery for >2weeks, 2 babies had died, and 15 families opted out, in accordance with the consent process, within two weeks of their infant’s birth. At some time later through the study period, another 430 families chose to withdraw from further study participation, after having completed the initial request to monitor their infant stool colour for the first month of life.
A total of 2,448 cards (40%) were received. Of the returned cards, 3% did not have an assigned stool colour. All of the six infants reported to have abnormal colour stools were identified as having transient stool colour change, and no further evaluation was required. Four percent of families recorded a normal stool colour and returned the card early, prior to two weeks after their infant’s birth. One infant, whose stool colour was recorded and returned as normal 5 days after birth, was later diagnosed with BA. No other cases of BA were identified.
During the two-month study step 1, the ISCC return rate was 26%, and of those who returned the card, 2% withdrew from further study participation (tables 1 and 2). The median infant age at which the ISCC was completed by the family was 31 days (Figure S-4; available online) and the median additional time for the mailed card to be received by the study centre was 13 days.
Strategy step 2 remained in place for a longer period than step 1 (4.5 months), as there was threat of a provincial postal strike. The overall rates of ISCC return in steps 2 and 3 were significantly higher compared with the step 1 strategy (Table S-7; available online). There was no difference between the ISCC return rates in the reminder letter and reminder telephone call strategies. The physician mail out strategy step 4 was continued for 16 weeks, because of the ongoing risk of a postal strike. The physician group supplemented an additional 6% to the percentage of parent ISCC return in this strategy, a rate significantly lower than those returned by the parents in the step 1 strategy (p < 0.0001). The step 5 strategy yielded the highest card return rate. While a reminder telephone call to physicians significantly improved the physician card return (13% vs 6%), the overall return rate was significantly less than that in any of the parent groups. The median infant age at which the stool colour was recorded by the physician was 44 days (Figure S-4; available online). There was no significant difference in the percentage of cards returned between the initial step 1 strategy and the one that was repeated 8 months later (table S-7; available online).
Randomized telephone surveys of families who did not return card.
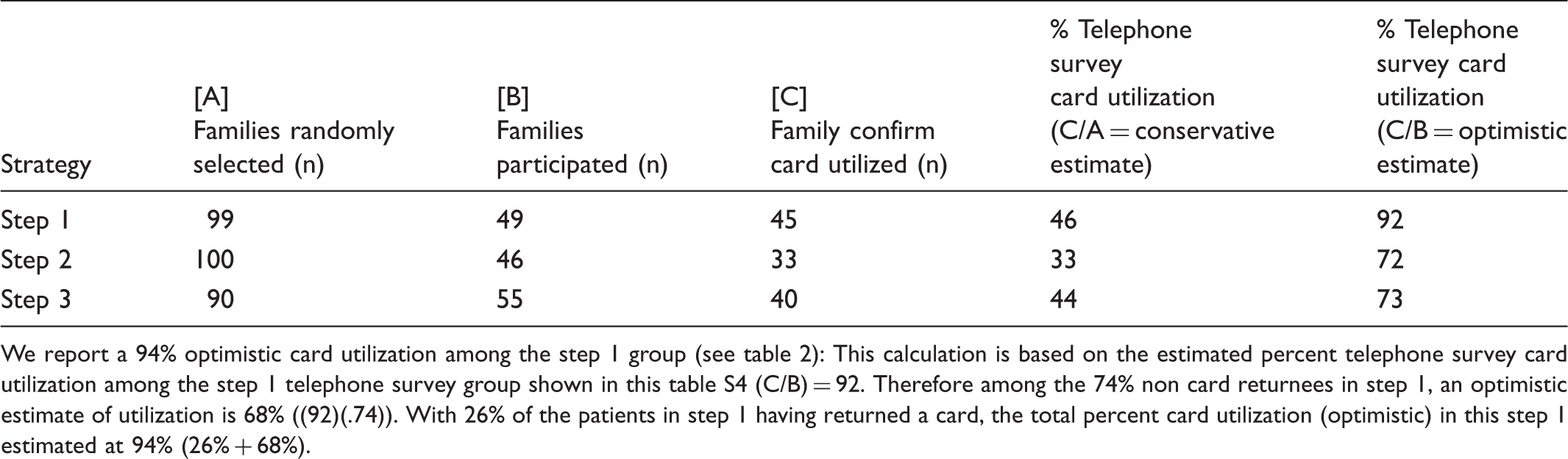
We report a 94% optimistic card utilization among the step 1 group (see table 2): This calculation is based on the estimated percent telephone survey card utilization among the step 1 telephone survey group shown in this table S4 (C/B) = 92. Therefore among the 74% non card returnees in step 1, an optimistic estimate of utilization is 68% ((92)(.74)). With 26% of the patients in step 1 having returned a card, the total percent card utilization (optimistic) in this step 1 estimated at 94% (26% + 68%).
For the cost effectiveness analysis, the predicted number of false positives was 244 per 381,400 births for the passive step 1 strategy, and 257 for step 2 (reminder letter) (table S-9; available online). The number of KP procedures performed increased from 17 (no screening) to 18 (step 2 reminder letter). As expected, the number of liver transplants decreased from 55 (no screening) to 52 (passive step 1 screening). The results indicate that universal passive screening is associated with fewer liver transplants and more KP procedures.
Expected incremental costs and life years gained from Universal Screening per 381,400 births in Canada.
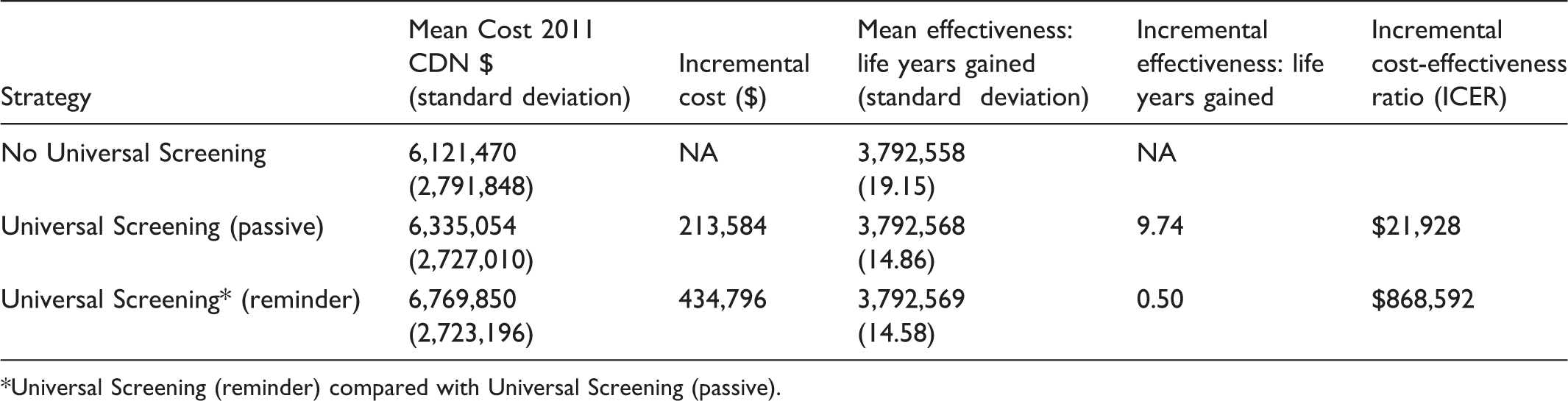
Universal Screening (reminder) compared with Universal Screening (passive).
Discussion
This is the first systematic study of a home based ISCC screening programme for BA outside Taiwan employing different intervention strategies to increase the ISCC return and utilization rates. It is also the first to present a decision analytic model and cost-effectiveness analysis for such a screening programme. The design was unique in that it was home-based and family-centered. 18
The high enrolment rate reflected strong family support for the relatively simple screening process, with minimal risk to the child. The highest percentage of ISCC return (55–63%) was observed among parents who were issued an ISCC at maternity and who then received a reminder card in the mail or a reminder telephone call in the third to fourth week after birth. ISCC utilization rates were estimated at 60–94% based on the telephone surveys. In contrast, the health care provider group had the lowest ISCC return rate, even among physicians who received a reminder telephone call. Several logistical challenges were identified with the physician strategy, suggesting that it is suboptimal for timely BA screening.
A novel decision tree and Markov model was developed to evaluate cost-effectiveness. The results indicate that a passive card distribution strategy (without reminder letter) is cost-effective, and the most parsimonious strategy for screening in Canada. The model was developed in consultation with clinical experts in hepatology, and thus closely represents clinical reality. In addition, the model was extensively validated to compare model predictions and screening outcomes. Parameter estimates were based on the best available evidence on the costs and effects. Estimates for having a second liver transplant as well as waiting for a first when there was no KP performed were based on expert opinion, as these estimates were not available in the literature. The time horizon was restricted to 10 years because we were modelling a paediatric population. Increasing the time horizon beyond this would have required data on costs and outcomes for adult populations.
Current newborn screening programmes identify several rare neonatal diseases, including those with an incidence similar to BA (ie. Phenylketonuria), however, what is lacking for early BA detection is an accurate and convenient laboratory test that can be incorporated into routine neonatal screening regimens.19,20,21 As with these other types of newborn testing, BA screening using ISCC raises concerns about false positive results and parental anxiety. However, the rate of false positive results using this card is small and speedy diagnostic testing for those who present with a false positive can help reduce this anxiety. While we believe that this level of anxiety would not require psychological counselling, we recognize that these issues require further study.
Use of an ISCC as a screening tool for BA was first initiated by Matsui in Japan in the 1990s. 22 In Taiwan, BA screening is now a national programme and the ISCC is integrated into the newborn health booklet. In the absence of any noted stool colour abnormality by the family, the doctor is still required to check the stool colour at the one month vaccination visit.12,13 While use of an ISCC has been reported in Switzerland and Brazil, details of the screening strategy used and results for card utilization have not been published.23,24
In contrast to the Taiwan programme, direct integration of the physician to the screening process appears less appealing in Canada. In Canada, the United States, and other Western countries, the first routine vaccination visit to a health care provider is later, at two months v one month in Taiwan, an age much less favourable for optimal and timely BA diagnosis. 11
As BA is a rare disease, with fewer than 4–6 new cases expected each year in British Columbia, our study was not designed to examine the screening efficiency for the diagnosis of BA. One aim of this study, however, was to determine the methods for optimizing the BA screening process in a setting outside Taiwan. We observed that 4% of families completed and returned the card early, having recorded normal stool colour before their infant was 2 weeks old. Given the natural history of BA, where acholic stools may not be present until after 2 weeks old, earlier assessment of stool colour would increase the false negative screening rate. 5 Indeed one infant with BA, whose card was completed and returned 5 days after birth was scored as having normal stool colour, and missed by the screening programme.
The median postal time to deliver the ISCC in Canada (13 days) was excessive, and a “mail-in” system for screening would impede timely BA intervention. In countries with similar postal challenges to those in Canada, consideration should be given to having a process for `hotline' telephone or electronic submission (fax/email/web site).
While it was not possible to precisely calculate the total ISCC utilization rate, we recognize that the utilization rate, rather than the card return rate, is key to the success of the screening program. In the Taiwan studies, ISCC utilization rates were not reported, however the overall card return rate was 65% and those with abnormal stool colour proved more likely to return the ISCC.12,13 Even our most conservative estimate of utilization (60%) is well below what would be achieved in an active screening programme, where only babies with abnormal stool colour would require notification to the screening centre.
We realize that families attending a tertiary care teaching hospital may be more inclined to adhere to screening protocols, lending bias to our card return and utilization rate results. While we excluded those patients having high-risk pregnancy or postnatal complications, and also employed a consecutive recruitment design to prevent selection bias, further studies, particularly in rural jurisdictions, are necessary to confirm the consistency of our findings.
Conclusions
This is the first report to systematically examine a variety of screening strategies and assess the feasibility of introducing a BA ISCC screening programme outside Taiwan. It is also the first to develop a BA Markov model to assess the cost-effectiveness of universal screening for BA. Our report identified several important challenges with the current Taiwan screening strategy, mostly as a result of variations in North American maternal infant identification practices and public health vaccine policies. Our study provides evidence to support a home based screening programme for BA in Canada with its operational design primarily targeted at families. A screening strategy involving parents is innovative and novel, and potentially has applicability to other health care programmes in Canada and elsewhere. Our results also suggest that universal screening using a passive card distribution can be cost-effective, on the assumption that it can be administered at a low cost and can achieve comparable screening performance levels with those reported in Taiwan.
We believe that home-based stool colour card screening strategy should be given serious consideration as a policy option in Canada. However, it would be necessary to confirm that our observed response rates are accurate and reproducible in other regions and settings, prior to acceptance and universal implementation of the screening programme in Canada.
Footnotes
Acknowledgements
We thank Dr. Jeffrey Lin and Dr. Mohsen Sadatsafavi for their generous statistical support and guidance, and Drs. Mei-Hwei Chang, Ben Shneider and Gary Levy for their input on the model structure and parameters. Dr Collet’s activity is supported by a Child and Family Research Institute research scholarship.
Conflict of interest
None of the authors have any conflicts of interest.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.