
Abstract
Objective
To evaluate and discuss the outcomes of the universal newborn hearing screening program conducted at four public hospitals in Malaysia.
Method
A retrospective analysis of the universal newborn hearing screening database from each hospital was performed. The database consisted of 28,432 and 30,340 screening results of babies born in 2015 and 2016, respectively. Quality indicators (coverage rate, referral rate, return for follow-up rate, and ages at screening and diagnosis) were calculated.
Results
Overall coverage rate across the four hospitals was 75% in 2015 and 87.4% in 2016. Over the two years, the referral rates for the first screening ranged from 2.7% to 33.93% with only one hospital achieving the recommended benchmark of <4% in both years. The return for follow-up rates for each participating hospital was generally below the recommended benchmark of ≥95%. The mean age at screening was 3.9 ± 1.2 days and 3.3 ± 0.4 days, respectively. The mean age at diagnosis for 70 infants diagnosed with permanent hearing loss was 4.7 ± 0.7 months in 2015 and 3.6 ± 0.9 months in 2016.
Conclusions
Quality measures for the universal newborn hearing screening program in four public hospitals in Malaysia were lower than the required standards. Nevertheless, some quality indicators showed statistically significant improvements over the two years. Next steps involve identifying and implementing the best practice strategies to improve the outcome measures and thus the quality of the program.
Keywords
Introduction
Globally, around 1–5 newborns per 1000 live births are diagnosed with congenital permanent hearing loss. 1 In a local study conducted at a university hospital in 2006, the prevalence of hearing loss among newborn babies was 0.42%. 2 The Joint Committee on Infant Hearing (JCIH) has endorsed early detection and intervention for infants with hearing loss through universal newborn hearing screening (UNHS). 3 The goals are to screen by one month of age, to confirm the diagnosis by three months, and to provide intervention by six months.
To date, UNHS has proved to be effective in detecting hearing loss at an early age.4–6 UNHS has also been associated with improved speech and language outcomes in hearing-impaired children.7–9 These positive outcomes have spread the adoption of UNHS in many countries across the globe, including Malaysia. As of today, there has been no national program on newborn hearing screening in Malaysia, but UNHS has been carried out through hospital initiatives. The implementation of UNHS started in the early 2000s in a few non-public hospitals such as Universiti Kebangsaan Malaysia Medical Centre and Universiti Sains Malaysia Hospital. 2 , 10 For public hospitals run by the Ministry of Health, the first program of UNHS was established in 2011, and three more programs were implemented two years later. In 2014, a total of seven UNHS programs were implemented in the Ministry of Health facilities. 11
Like every other program, the development and implementation of UNHS in these seven public hospitals have been based on the guidelines recommended by the JCIH.3,12,13 These guidelines also promote a quality assessment protocol to track the program’s performance against set benchmarks: a screening coverage rate of at least 95%, a referral rate of not more than 4%, and a return for follow-up rate of at least 95%. Therefore, the Ministry of Health’s Audiology Technical Committee took the initiative of measuring the performance of UNHS in the seven hospitals in 2014. 11 The results revealed unsatisfactory performance for all of the measured quality indicators. For instance, the coverage rate was only 72%, and the referral rate was above 4%, ranging from 5% to 32%.
For continued improvement of the UNHS programs already implemented by public hospitals in Malaysia, it is crucial to assess and monitor regularly the quality of the services provided. Therefore, this study was carried out to evaluate and report on the performance of four public hospitals that have implemented the UNHS program, for 2015 and 2016. Specifically, the goals were to evaluate the quality indicators of coverage rate, referral rate, and return for follow-up rate against the standard benchmarks. The measured quality indicators obtained in each year were compared to evaluate the progress of each UNHS program. The age at diagnosis was also measured to determine if the programs were effective in detecting the presence of hearing loss by three months of age.
Methods
This study was approved by the Research Ethics Committee of Universiti Kebangsaan Malaysia (UKM PPI/111/8/JEP-2019–244) and the Medical Research and Ethics Committee, Ministry of Health Malaysia (NMRR-19–3277-51586). Seven hospitals that conducted the UNHS program were approached to participate, but only four consented to take part. All participating hospitals in the study were required to follow a guideline developed by the Ministry of Health, Malaysia. 14 Generally, the initial hearing screening was done by nurses while audiologists performed the diagnostic hearing test.
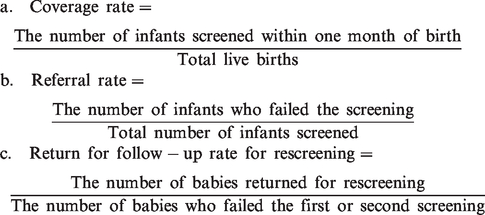
This was a retrospective cohort study based on data from the UNHS database of each participating hospital collected from 1st January 2015 to 31st December 2016. Each database contains demographic information, initial and rescreening test results, age at first and subsequent screening, age at diagnosis, and device used for screening. The databases only allowed the generation of quality indicators for screening that include coverage rate, referral rate and return for follow-up for rescreening. The quality indicators were expressed as a percentage and calculated using the following formulae:
Data analysis
Data were analysed using Microsoft Excel version 2007. Descriptive analysis in particular percentages was used to compute the quality indicators. Differences in the measured quality indicators between years were statistically tested using χ2.
Results
The UNHS program characteristics
Generally, the first screening was performed either in the post-natal ward or neonatal intensive care unit (NICU) before babies were discharged. The duration of time until second screening ranged from two weeks to two months. Second (and third) screenings and diagnostic hearing evaluation were carried out as outpatient treatments in the audiology clinic. As of 2016, all the hospitals studied had less than five years’ experience in conducting the UNHS program. Table 1 displays the general characteristics of the UNHS program for each participating hospital. Depending on hospital resources, automated auditory brainstem response (AABR) and distortion product otoacoustic emissions (DPOAE) were used, either alone or combined, as the hearing screening tool. All hospitals used a consistent hearing screening protocol from 2015 to 2016, except for Hospital D in which both AABR and DPOAE were utilised to screen all babies born in 2015. However, this hospital changed its hearing screening protocol the following year; AABR was performed on babies who were born with high-risk indicators while healthy neonates were screened using DPOAE.
General characteristics of universal newborn hearing screening (UNHS) program for each participating hospital.
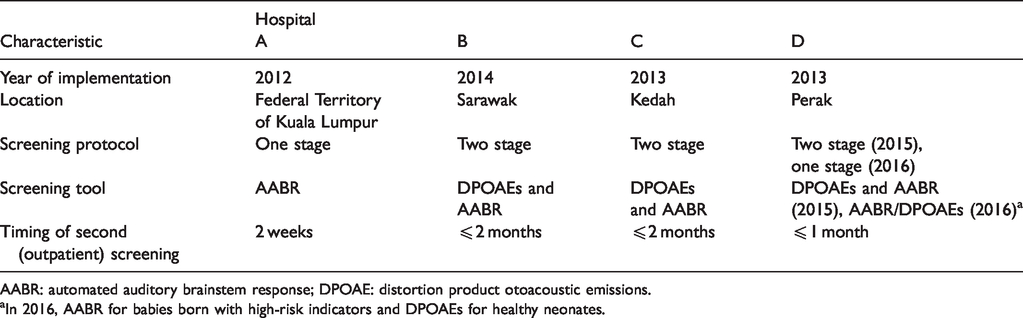
AABR: automated auditory brainstem response; DPOAE: distortion product otoacoustic emissions.
aIn 2016, AABR for babies born with high-risk indicators and DPOAEs for healthy neonates.
Hearing screening results
Results of the hearing screening test from all four hospitals in 2015 and 2016 are summarised in Table 2. The number of live births in Hospitals A and C was about two times larger than in Hospitals B and D. In general, a decline in the number of live births in 2016 was observed in all hospitals. Concerning the UNHS program, 28,432 and 30,340 babies were screened from all four hospitals in 2015 and 2016, respectively. In each year, about 2% of this population were screened after the age of one month. The proportion of infants screened in Hospital A was identical for the two years, at about 92%. A gradual increase over the two years in the number of infants screened for hearing loss was observed in Hospital B (i.e. from about 76% to 81%) and C (i.e. from about 83% to 87%). Hospital D showed a rapid increase in the number of infants screened, from about 59% in 2015 to 98% in 2016.
Summary of hearing screening results from each participating hospital in 2015 and 2016.
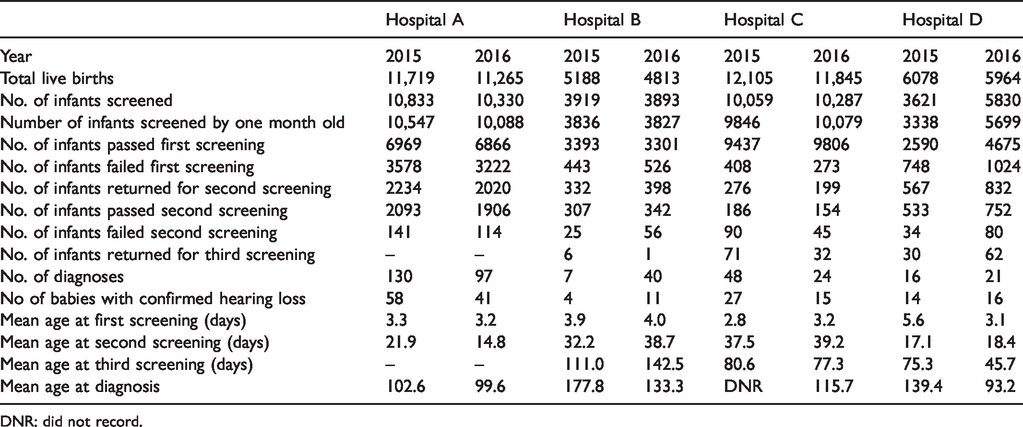
DNR: did not record.
Also shown in Table 2 is that babies with referral results were screened up to three times in Hospitals B, C and D while screening in Hospital A was done only twice. Consequently, Hospital A managed to complete the hearing screening process within a month in the two consecutive years (i.e. 21.9 days in 2015 and 14.8 days in 2016). For the other hospitals, the average time taken to complete the screening process was 4.5 ± 0.8 months for B, 2.8 ± 0.1 months for C and 2.2 ± 0.7 for D. In total, for 2015 and 2016, about 48.6% (n = 186) of infants were diagnosed with hearing loss and 197 out of 383 (51.4%) who attended the diagnostic evaluation were found to have normal hearing bilaterally.
Quality indicators
Coverage rate
As shown in Table 3, the coverage rate in 2015 varied from 54.9% to 90%, with none of the hospitals achieving the standard benchmark of 95%. A statistically significant increase (p < 0.0001) in the coverage rate was observed for all hospitals in 2016, except Hospital A (p = 0.14). The coverage rate for Hospital D accelerated from about 55% in 2015 to about 96% in 2016 (p < 0.0001). Moreover, Hospital D was the only centre that managed to hit the benchmark of 95% coverage rate for the 2016 birth cohort.
Quality indicators for each hospital in 2015 and 2016.

Referral rate
The referral rate refers to the number of infants who failed the first or subsequent screening tests either in one or both ears. The initial referral rates were beyond the quality standard target of 4% except in Hospital C, which reached the recommended benchmark in both years. Moreover, Hospital C showed a decreasing trend in referral rate over the two years (i.e. 4.1% in 2015 to 2.7% in 2016), and the reduction was found to be statistically significant (p < 0.0001). A significant decrease in the initial referral rate was also observed for Hospital D (p < 0.0001) but not for Hospital A (p = 0.002). For the proportion of infants who failed the second screening, all hospitals exceeded the 4% benchmark and the differences between their rates were not statistically significant.
Return for follow-up rate
All hospitals showed unacceptably low return for follow-up rates for both second and third screening with the percentage never exceeding the 95% benchmark in either year. Although not statistically significant, there was a trend which showed a decline over time in the number of babies attending the third level screening for Hospitals B, C and D. A total of 201 infants in 2015 and 182 infants in 2016 attended the diagnostic assessment, and 70 were diagnosed with permanent hearing loss.
Age at diagnosis
The age at diagnosis refers to the chronological age of the child on the date of completing the diagnostic assessment at the audiology clinic. As shown in Table 2, there is a declining trend in the mean age at diagnosis from 2015 to 2016 for Hospitals A, B and D. However, infants in these three hospitals received diagnoses beyond the recommended timeline of three months in both years (i.e. average age = 3.6, 5.6 and 4.2 months for A, B and D, respectively).
Discussion
This study reports preliminary findings on the performance of the UNHS program conducted at four Malaysian public hospitals over two years. Coverage rate, referral rate, return for follow-up rate and age at diagnosis were used to measure the program’s performance.
Coverage rate
The results presented in this study show that all hospitals did not achieve the coverage rate of 95% in 2015. However, one hospital (D) reached the benchmark in 2016. Although a general trend of increasing coverage rate was observed for three out of the four hospitals over the two years, the rates are still lower when compared to other programs employing a similar screening protocol.15,16 A few factors could be responsible for this relatively low coverage. First, some healthy infants might have been discharged early, even within a day of birth. 17 Second, the high birth rate with a shortage of personnel to conduct the screening may hinder the hospitals from providing the optimum service to all infants. Nurses who shoulder multiple responsibilities may not always be able to attend to hearing screening.17,18 Third, about 2% of infants from each hospital in each of the two years were screened after the first month of birth. Further data analysis revealed that this group of infants were from the NICU ward of the participating hospitals or neighbouring centres that did not have a UNHS program in place, or were those who had been discharged early prior to screening. These logistic and coordination issues were teething problems that have also been reported in the early phase of a screening program in Italy. 19
Referral rate
Achieving a low referral rate proved a challenge, as most of the hospitals did not meet the required benchmark of <4%. The mean age at first testing for all four hospitals was beyond 48 h. Therefore, testing using DPOAE should not have caused a high referral rate, because the amniotic fluid or debris had already resolved from the newborn middle ear cavity by the time the first screening was administered. In Uganda, Walsh et al. 20 demonstrated that otoacoustic emissions (OAEs) had a high pass rate (i.e. 90.9%) when performed on infants at least a day old. This was evident with Hospital C having a comparable average age of first screening to the others but yet managing to attain the lowest referral rates when using DPOAEs. As for Hospital A that utilised AABR, the likelihood of achieving the quality standard of <4% should have been much easier than for centres using DPOAEs in the first screening. Substantial evidence indicates that the AABR is not affected by amniotic fluid or debris when measured in newborns a few hours after birth. 15 Based on these arguments, the alarming referral rates found in this study are most likely due to lack of experience with hearing screening procedures, or in handling newborns. A study in Taiwan demonstrated that having a dedicated and experienced hearing screener helped in attaining a low referral rate. 15
Findings in this study also show that the referral rates for the second screening did not meet the benchmark of <4%. However, this rate for most hospitals declined in each year when compared with the first screening (with the exception of Hospital C). These patterns are consistent with many studies that show the use of AABR at the second level of screening helps in reducing the referral rate.21–25
Return for follow-up rate
The return for follow-up rates for all four hospitals was below the standard. This is a common major problem also found in newly implemented programs such as in Italy 19 and Turkey. 26 In this study, the reason for this phenomenon could be a lack of awareness about childhood hearing loss among parents and healthcare professionals. A recent local study found that the majority of mothers from an urban area (87.3%) had inadequate knowledge with regard to childhood hearing loss. 27 Mazlan and Min 28 also found that the majority of Malaysian healthcare professionals (about 80%) who worked in hospitals running a newborn hearing program had poor knowledge about the program. Another possible reason for the poor follow-up rates could be that some mothers went back to their hometowns in areas far away from the birthing hospitals for the postpartum confinement period. Due to the geographical distance, parents may be unable to bring their infants for rescreening. This situation is aggravated by limited access to audiology services, as most facilities are available only in the capital and major cities, and the UNHS program is only available at selected public hospitals. Other possible explanations described in previous literature that might hold for these study results include poor communication between screeners and parents, 17 , 25 and absence of a tracking system. 29
Overall, the measurement of coverage and referral rates in the study is in line with the quality indicators for screening recommended in the JCIH 2019 guidelines. 13 Most of the participating hospitals failed to achieve the recommended benchmarks for these two indicators in both years. Another quality indicator recommended in the recent JCIH guidelines but not measured in this study is the false-positive rate. Instead, we measured the return for follow-up rate, which was routinely collected in many previous studies.
Age at diagnosis
The ultimate aim of any UNHS program is to identify every infant with permanent hearing loss before three months of age. Of 383 infants who attended the diagnostic assessment over the two years, 70 were diagnosed with permanent sensorineural hearing loss, giving a prevalence of 0.12%. This value underestimates the true prevalence of permanent hearing loss due to the low coverage rate and the relevant number of drop-out infants at each stage of the screening program (e.g. n = 1768 and 1596 in 2015 and 2016 at initial screening, respectively). The reported mean age at diagnosis for the 70 infants was 4.7 months in 2015 and 3.6 months in 2016. Some infants could not get a timely appointment due to a long waiting list for a diagnostic auditory brainstem response (ABR). Another source of delay in diagnosis was from infants who required several visits from a doctor to rule out middle ear disorders.
Recommendations for improving the UNHS program
Findings from this study indicate the need to review the implementation of the UNHS program in all participating hospitals. As shown in many studies, 18 , 22 , 30 having dedicated personnel who take ownership of the program could help improve the coverage rate. If this is not feasible, hospitals could rotate nursing and midwifery staff, but must ensure that they received training and are competent to perform the screening. Another recommendation that hospitals could follow to improve the coverage rate is to contact parents of infants who were not screened due to early discharge and try to schedule the screening before one month of age.
Regarding the high referral rate, all hospitals that use DPOAE should continue the best practice of screening the newborns after 48 h of age.20,24,25 As the referral rates in this study are most likely attributable to the lack of experience in performing hearing screening, a method for regularly monitoring and assessing screeners’ performance should be established by all hospitals. Apart from that, modifying the existing screening protocol could help to reduce the initial referral rate. Hospital A might consider adopting the two-stage combined DPOAE and AABR protocol which has been proved to be effective and efficient for a large public hospital with a high birth rate. 18 For hospitals that utilise DPOAE, consider repeating the test close to discharge for newborns who failed the initial testing.15,24,31,32
The high lost-to-follow-up rate found in the study acts as a threat to the overall success of the UNHS program. Having a tracking system and educating stakeholders could improve the program’s efficiency. 16 , 28 , 30 , 33
In summary, having dedicated screening personnel, retraining screeners, educating parents and implementing a tracking system are examples of recommendations that might aid participating hospitals in overcoming the current challenges.
Limitations
As only four hospitals participated in this study, the results might not be generalisable to other hospitals in Malaysia, especially those university and private hospitals whose management may be different from public hospitals. No observation was done to have more understanding about each hospital setting and its UNHS program; hence, much of this research relied on the hospital’s willingness to share their database and information about the UNHS program with researchers.
Conclusions
The quality indicators reported in this study represent the beginning of a quality improvement process for the UNHS program for public hospitals in Malaysia. Overall, the performance of all participating hospitals in this study did not achieve the minimum international standard for UNHS. The study also outlines potential factors influencing the program’s performance along with recommendations that could lead to improved program outcomes.
Footnotes
Acknowledgements
We gratefully acknowledge the contributions of the professionals at each facility hospital for their assistance and cooperation throughout the study.
Declarations of conflicting interests
The authors(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.