
Abstract
Objective
To evaluate the quality of colonoscopies performed after a positive faecal immunochemical test in the French colorectal cancer screening programme.
Methods
Retrospective analysis of all colonoscopies performed between 2015 and 2019 after a positive quantitative faecal immunochemical test in the population-based colorectal cancer screening programme organised in Alsace, part of the French programme. The following indicators were evaluated: annual colonoscopy volume, caecal intubation rate, adenoma detection rate, proximal serrated lesion detection rate and proportion of patients referred directly to surgery for benign polyp management. Endoscopists who performed <30 faecal immunochemical test positive colonoscopies were non-assessable.
Results
Overall, 13,455 faecal immunochemical test-positive colonoscopies performed by 116 community gastroenterologists were included, 13,067 of them by 80 assessable endoscopists. The overall caecal intubation, adenoma detection and proximal serrated lesion detection rates were 97.9%, 57.6% and 7.6%, respectively. They were <90%, <45% and <1% for 1.3%, 12.5% and 6.3% of the endoscopists, respectively. Overall, 1028 (7.9%) individuals were examined by 13 low-performing endoscopists and 328 (2.4%) individuals by 33 low-volume non-assessable endoscopists. Among 9133 individuals harbouring polyps, 155 (1.7%) had unwarranted surgery for a benign polyp. Overall, 1487 individuals (11.1%; 95% confidence interval 10.5–11.6) were not given the best possible chances, whereas 5545 individuals (41.2%; 95% confidence interval 40.4–42.0) were offered the best possible chances by 37 endoscopists.
Conclusions
At programme level, the key performance indicators evaluated largely exceeded the target standards. At individual level, at least one in nine individuals was not given the best possible chances during faecal immunochemical test-positive colonoscopies by a minority of poor-performing and/or low-volume endoscopists.
Most colorectal cancers (CRCs) are preventable whatever the screening method used: faecal occult blood test (FOBT), flexible sigmoidoscopy and colonoscopy and polypectomy are effective at reducing CRC incidence and mortality. 1 All these screening methods lead to colonoscopy allowing detection of early-stage CRC and removal of neoplastic polyps. However, colonoscopy is an operator-dependent examination: e.g. colonoscopy completeness, conventional adenoma and serrated lesion detection and polypectomy competency vary dramatically between endoscopists. Low caecal intubation rate (CIR) is associated with post-colonoscopy CRC. 2 Low adenoma detection rate (ADR) is associated with higher risk of post-colonoscopy CRC and fatal post-colonoscopy CRC.3,4 Up to 30% of post-colonoscopy CRCs may be due to incomplete resection. 5
Several sets of quality recommendations for colonoscopy were thus elaborated worldwide.6–9 Notwithstanding, most CRC screening programmes, including organised ones, report wide variations in colonoscopy quality.10–13 Therefore, some countries impose specific certification or accreditation for endoscopists and/or centres authorised to participate in their CRC screening programmes,8,14–16 for example, around 15% of active endoscopists are accredited to perform colonoscopies within the English bowel cancer screening programme (BCSP) and 66% in the Dutch programme. 16
Many countries have performed nationwide evaluations of colonoscopy quality indicators and found that colonoscopy performance was below their quality standards, leading to quality improvement programmes resulting in significant improvement.14,15,17–19 Such an evaluation has never been conducted in France, either for all colonoscopies or for those performed within the national CRC screening programme with faecal immunochemical test (FIT).
The aim of the present study was to evaluate the quality of FIT-positive colonoscopies performed in the French organised CRC screening programme.
Methods
Screening programme
The French organised CRC screening programme, implemented from 2003, moved from guaiac-based FOBT (Hemoccult II) to quantitative FIT (OC-Sensor) in 2015. Its design has been previously described. 20 Residents aged 50–74 years are invited every other year to participate. People with serious comorbidities, recent CRC screening or high CRC risk are excluded. The FIT positivity threshold is set at 30 µg haemoglobin per gram (µg/g) faeces. People with a positive FIT are referred for colonoscopy.
Colonoscopies
All data concerning FIT-positive colonoscopies performed between 2015 and 2019 within the screening programme in Alsace (0.57 million residents aged 50–74) were prospectively collected and retrospectively analysed. In France, almost all colonoscopies are performed by certified gastroenterologists, their certification process including the performance of 200 colonoscopies and 50 polypectomies. There is no certification maintenance rule related to the practice of colonoscopy in general and within the screening programme in particular. All certified community gastroenterologists participated in the screening programme. Colonoscopies were performed generally with anaesthesia provided by an anaesthesiologist. Colonoscopies displaying an invasive CRC were excluded for the calculation of quality indicators. Endoscopists who had performed <30 FIT-positive colonoscopies during the period were considered non-assessable. The pathology examination of detected polyps was performed as a routine procedure by community general pathologists.
Indicators
CIR was defined as the percentage of colonoscopies where the whole caecum and its landmarks were visualised. ADR was defined as the percentage of colonoscopies where at least one conventional adenoma was found, serrated lesions being excluded. 6 Proximal serrated lesion detection rate (ProxSLDR) was defined as the percentage of colonoscopies where at least one serrated lesion of any size was found proximally to the splenic flexure. 21 Polypectomy competency was estimated indirectly by the number of patients referred directly to surgery for benign colorectal lesion management, without prior referral to an experienced endoscopist.
Standards
Minimum and target standards were those recommended by the French colonoscopy quality guidelines, that is, 90% and 95% for CIR, 45% and 55% for ADR, and 1% and 5% for ProxSLDR, respectively. 9 The US guidelines ‘suggest measuring and reporting the proportion of patients referred to surgery for benign colorectal lesion management’. 6 We considered unwarranted direct referral to surgery (without prior referral to a more experienced endoscopist) of individuals harbouring benign appearing polyp(s) by endoscopists who had an endoscopic resection rate of large (≥20 mm) polyps <90%. 22
Statistical methods
Qualitative variables were described by their frequency with 95% confidence intervals (95% CI) and quantitative variables by their median, range, mean and standard deviation (SD). The chi-square test was used to search for statistical significance by comparisons of proportions. The significance level was set at 0.05. Statistical analyses were performed using R software version 3.6.0. This study was approved by the institutional review board of the Mulhouse hospital.
Results
In 2018–2019, the FIT uptake was 44.4%; the positivity rate was 3.8%. During the study period, 14,228 individuals (mean age 62.4 years; SD 7.0; men 59.7%) had FIT-positive colonoscopies performed by 116 endoscopists. The flow chart of the study is presented in Figure 1.
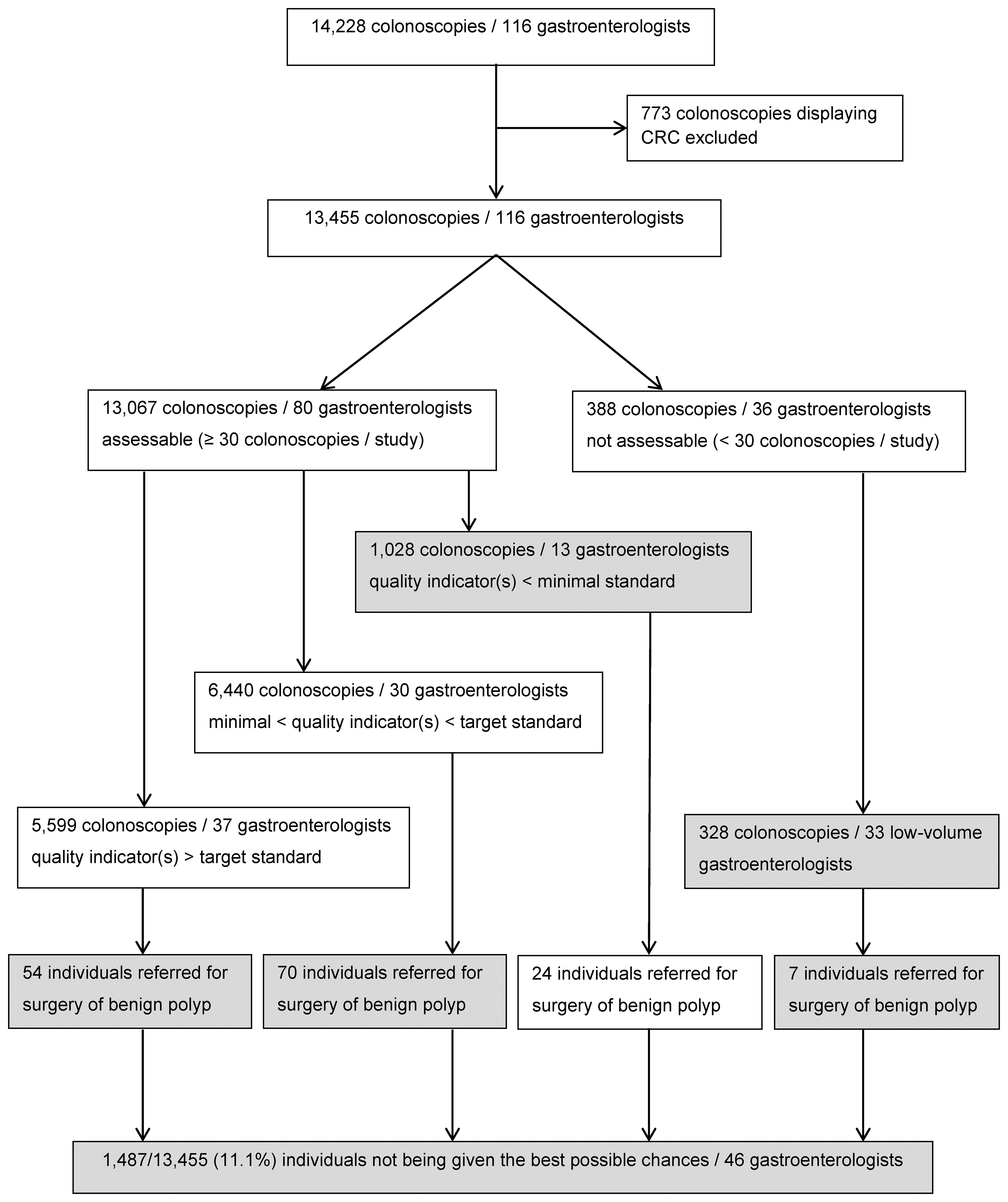
Flow chart of study.
CIR and neoplasia-related indicators (Table 1)
For the assessment of quality indicators, 773 (5.4%) colonoscopies displaying a CRC were excluded. Another 388 (2.7%) colonoscopies were excluded because they were performed by 36 (31.0%) non-assessable endoscopists. Thus, 13,067 (91.8%) colonoscopies performed by 80 (69.0%) endoscopists were analysed. The overall CIR was 97.9% (mean 97.5%; SD 2.4%). It varied from 84.2 to 100% depending on the endoscopist. It was ≥90% for (79/80) 98.8% of endoscopists. The overall ADR was 57.6% (mean 56.5%; SD 10.2%). It varied from 27.8 to 81.0% depending on the endoscopist. It was ≥45% for (70/80) 87.5% of endoscopists. The overall ProxSLDR was 7.6% (mean 7.7%; SD 5.5%). It varied from 0 to 25.3% depending on the endoscopist. It was ≥1% for (75/80) 93.8% of endoscopists. Five (6.3%) endoscopists never detected proximal serrated lesions.
Performances of 80 assessable endoscopists who performed 13,067 colonoscopies: caecal intubation rate and neoplasia-related indicators.

ADR: adenoma detection rate; CIR: caecal intubation rate; n Colo: number of colonoscopies; n E: number of endoscopists; ProxSLDR: proximal serrated lesion detection rate.
Among 13,067 individuals, 1028 (7.9%) had their colonoscopies performed by 13/80 (16.3%) low-performing endoscopists (≥1 quality indicator below minimal standards), 6440 (49.3%) by 30/80 (37.5%) endoscopists whose quality indicators were situated between minimal and target standards, and 5599 (42.8%) by 37/80 (46.3%) endoscopists whose quality indicators were all above the target standards (Figure 1).
Polypectomy competency (Table 2)
Overall, 9133/14,228 (64.2%) individuals harboured one or more polyps. Among them, 155 (1.7%) had unwarranted surgery for a benign polyp. Direct referral for surgical resection of a benign polyp was observed in 124/8371 (1.5%) individuals whose endoscopy was performed by 67 endoscopists with quality indicators that were all situated above the minimal standards. This proportion was significantly lower than observed in 31/762 (4.1%) individuals referred to surgery for the same reason by 13 low-performing and 36 non-assessable endoscopists (p < 0.001).
Direct referral of benign appearing polyp for surgical resection.
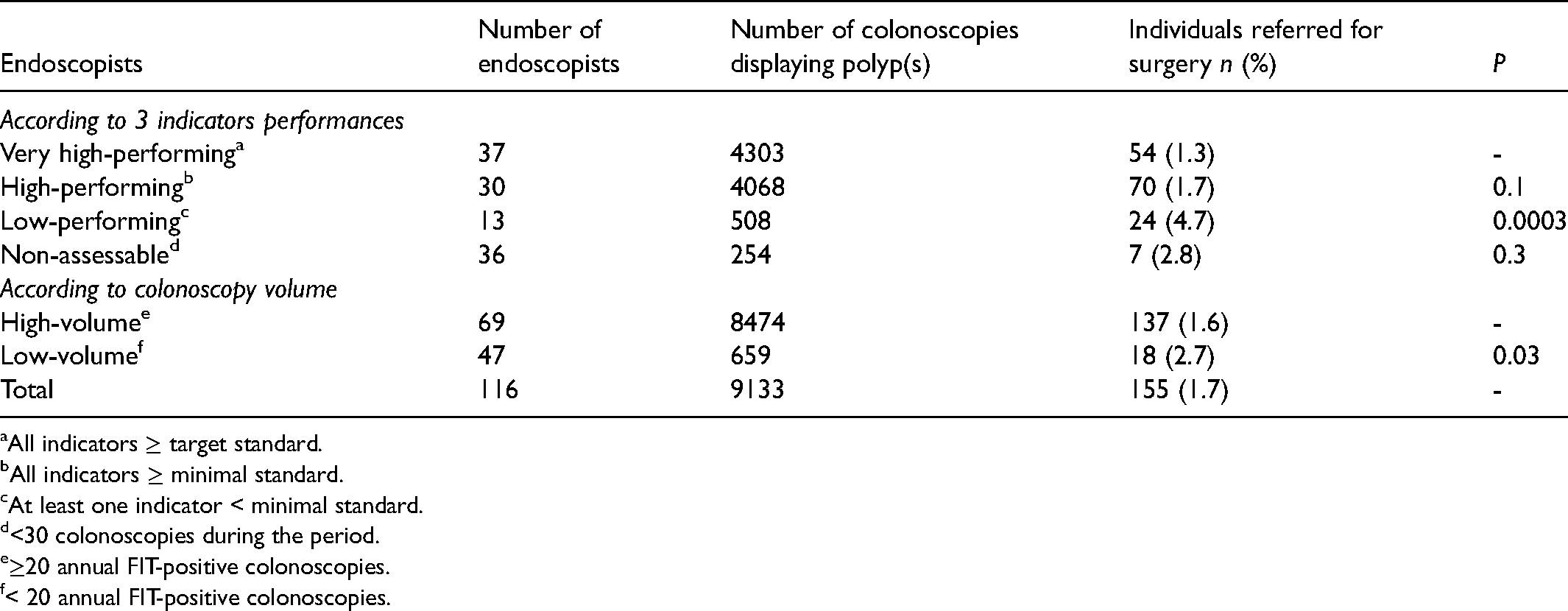
All indicators ≥ target standard.
All indicators ≥ minimal standard.
At least one indicator < minimal standard.
<30 colonoscopies during the period.
≥20 annual FIT-positive colonoscopies.
< 20 annual FIT-positive colonoscopies.
FIT-positive colonoscopy volume
Annual FIT-positive colonoscopy volume varied from 1 to 151 depending on the endoscopist (mean 33; SD 32; median 24). Of 116 endoscopists, 47 (40.5%) were considered low-volume (<20 annual FIT-positive colonoscopies) and performed 1077/14,228 colonoscopies (7.6%). Performance was assessable in 14 low-volume endoscopists and in 66 high-volume endoscopists; all non-assessable endoscopists were low-volume except three high-volume endoscopists who retired during the study period. Performance level was low in 8/14 (57.1%) low-volume endoscopists and in 5/66 (7.6%) high-volume endoscopists; the difference was highly significant (p < 0.001).
Loss of chance
Overall, 1152 (1028 + 54 + 70) of 13,455 individuals (8.6%; 95%CI 8.1–9.0) were not given the best possible chances by 13 (11.2%) low-performing endoscopists. In addition, 328 (2.4%; 95%CI 2.2–2.7) others were managed by 33 (28.4%) non-assessable low-volume endoscopists. Adding seven individuals directly referred to surgery for benign polyps by non-assessable endoscopists, a total of 1487/13,455 individuals (11.1%; 95%CI 10.5–11.6; i.e. one in nine individuals) were not given the best possible chances. By contrast, 5545 (5599–54) individuals (41.2%; 95%CI 40.4–42.0; i.e. one in 2.4 individuals) were given the best possible chances by 37 (31.9%) endoscopists with quality indicators that were all above target standards.
Discussion
Main findings
The main findings of this study are that: (1) at the French organised CRC screening programme level, the three key performance indicators evaluated, namely CIR, ADR and ProxSLDR, largely exceeded the target standards; however (2) at the individual level, at least one in nine individuals was not given the best possible chances during FIT-positive colonoscopies, as these procedures were performed either by a minority of endoscopists who were low-performing (11%) or low-volume and non-assessable (28%). By contrast, the best possible chances were offered to one in 2.4 individuals by a third of the endoscopists whose performances exceeded target standards.
Detection competency
There is no evidence-based benchmark established for FIT screening. The US Multi-Society Task Force on CRC recommended a benchmark of 45% in men and 35% in women for FIT-positive colonoscopies (positivity threshold 20 µg/g). 23 French recommendations adopted a minimal benchmark of 45% based on our first FIT round. 9 Low ADRs are commonly observed in a non-negligible proportion of endoscopists in all countries and screening programmes, from around 6% for accredited endoscopists in the English BCSP to 37% in Austrian private practices, as compared with our 12.5% rate.11,19
The ability of endoscopists to detect proximal serrated lesions varies greatly, significantly more than for conventional adenomas. 21 This is why some authors proposed to assess separately adenoma and serrated lesion detection rates and to measure ProxSLDR as an easy-to-measure proxy for the detection of clinically relevant serrated lesions, a rate that ignores recto-sigmoid hyperplastic polyps and avoids pathology interpretation difficulties. 21 The US and the European Society of Gastrointestinal Endoscopy guidelines do not recommend measuring this indicator,6,7 whereas the British guidelines recommend a minimum rate of 5% and French guidelines set a minimal level at 1% and a target standard at 5%.9,21 One must recognise that today there is no evidence that low ProxSLDRs are associated with post-colonoscopy CRC risk. Like others, we observed quite a good correlation between ADR and ProxSLDR. 24 However, out of ten low-ADR endoscopists, only two had low ProxSLDRs, and of five low-ProxSLDR endoscopists, only two had low ADRs, giving an argument for measuring the two indicators separately.
Loss of chance
French endoscopists’ competency related to colonoscopy completeness is good (only one low performer) and similar to that of other population-based studies.6,7 Taking into consideration three key performance indicators, that is, CIR, ADR and ProxSLDR, we considered that 11% of endoscopists did not give their patients the best possible chances as low CIRs and ADRs are associated with higher risk of post-colonoscopy CRC and serrated lesions might represent 10–25% of colorectal carcinogenesis.2–4,21
Polypectomy competency
There is no established indicator for the assessment of polypectomy competency. We proposed previously that the rate of patients referred to surgery for benign colorectal polyp management, an indirect reflection of polypectomy competency, should be added to the existing quality indicators of CRC screening programmes for routine measurement and reporting. 22 Unfortunately, there is no way to compare our 1.7% rate of referral to surgery with that of other programmes as this parameter is never reported. There is no established benchmark. Ideally, the rate should be close to zero as endoscopic resection of almost all benign polyps is achievable in experienced hands. 25 It should be the lowest possible in population-based programmes and was 1.5% for our high-performing endoscopists, significantly lower than the 4.1% for low-performing, low-volume and non-assessable endoscopists. This rate reflects part of the cost-effectiveness and benefit-risk balances of screening programmes since surgical resection is associated with significantly higher costs and rates of adverse events than endoscopic resection. 26 Referral to an experienced endoscopist is today insufficient as evidenced by the high rates of surgery for benign colorectal polyps observed in most countries. 27 The management of patients with benign-appearing large colorectal polyps should be discussed in a multidisciplinary setting with established locoregional referral pathways as recommended by the British guidelines. 28
Colonoscopy volume
A recent meta-analysis found that lower colonoscopy volumes were associated with lower CIRs and higher adverse events rates, particularly for perforation, without significant association with ADR and post-colonoscopy CRC risk. 29 There was no sufficient evidence to support a minimum annual colonoscopy volume benchmark. We adopted a cut-off of 20 annual FIT-positive colonoscopies as we found that the CIRs and ProxSLDRs of endoscopists performing <20 colonoscopies were significantly lower than of those performing ≥20. 24 Here, more than half of the low-volume, assessable endoscopists were low-performing. We thus considered that the patients were not being given the best possible chances when their endoscopists were non-assessable and performed <20 annual FIT-positive colonoscopies.
Certification/accreditation
At the programme level, the French endoscopists’ performances compared well with those of neighbouring countries (Table 3). However, at the individual level, a minority of endoscopists were low performing. We demonstrated previously that English BCSP-accredited endoscopists had significantly higher ADRs in guaiac-based FOBT-positive colonoscopies than French community endoscopists. 30 Similarly, the community endoscopists’ performances reported in the Scottish bowel screening programme were lower than those of endoscopists accredited for the English BCSP. 13 Likewise, the rate of referral to surgery for large polyps was significantly lower within the English BCSP than outside. 31 Germany and Poland also base their colonoscopy screening programmes on specific certification of participating endoscopists and/or centres.14,15 Some countries, such as Austria, propose voluntary participation in quality assurance programmes for endoscopists. 19 By contrast, within the French CRC screening programme, all certified community gastroenterologists perform the colonoscopies, without any quality assessment or control. Likewise, Italy, Scotland and Denmark do not require specific certification of endoscopists for their CRC screening programmes.12,13,32 Accreditation seems all the more desirable for FIT CRC screening programmes since the neoplasia yield of FIT-positive colonoscopies is the highest among all colonoscopy indications and the risk of adverse events is correlated with polypectomy and polyp size and number. In our screening programme, a large polyp was found in one of every 12 FIT-positive colonoscopies, i.e. 10 times more often than in the Polish colonoscopy screening programme. 22 Adverse events of colonoscopy were significantly more frequent in our FIT CRC screening programme than usually estimated. 33 Accreditation for CRC screening could be seen as equivalent to double reading of mammograms for breast cancer screening; that is, as a way to offer the best possible chances to screened individuals.
Comparison of quality indicators in faecal immunochemical test positive colonoscopies between different colorectal cancer screening programmes.
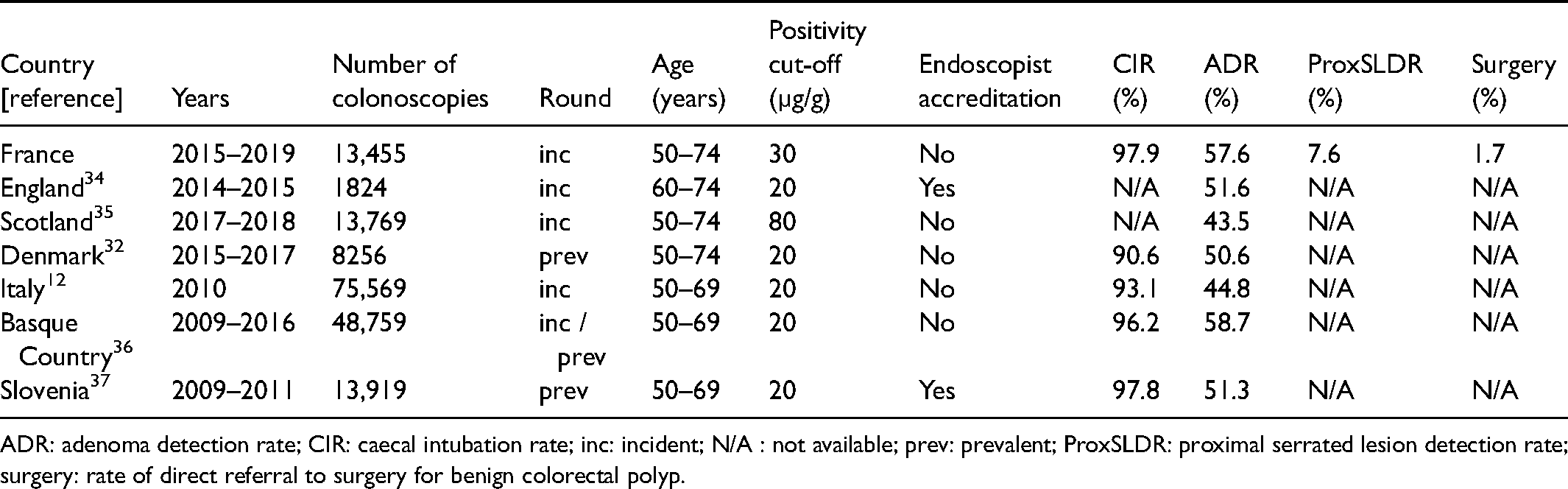
ADR: adenoma detection rate; CIR: caecal intubation rate; inc: incident; N/A : not available; prev: prevalent; ProxSLDR: proximal serrated lesion detection rate; surgery: rate of direct referral to surgery for benign colorectal polyp.
Strengths and limitations of the study
This was a large population- and community-based study, which is its main strength. Other strengths include prospectively collected data and a high-quality database. Our study is not without limitations. The main is that several quality indicators were not evaluated, such as quality of bowel preparation, withdrawal time, polypectomy technique, adverse events and post-polypectomy surveillance appropriateness, so that the rate of individuals who were not being given the best possible chances was underestimated. The creation of a national colonoscopy screening database, including pathology results, is crucial to facilitate monitoring of these key performance measures.11,14–16 Another limitation is that colonoscopy completeness was ascertained from the written report only and was not checked using photo documentation, so that it could be overestimated. Moreover, the retrospective design of the study can be considered as a limitation. However, it can also be conceived as a strength owing to the fact that measures were unbiased, endoscopists being unaware that their performances were monitored. Finally, the generalisability of our results is questionable: A quick reading might suggest that our endoscopists exhibited poor performance and that our alarming message is specific to our local CRC screening programme. Such is not the case since colonoscopy series commonly report a significant proportion of low-performer endoscopists, the percentage being lower in programmes involving accredited endoscopists.2–4,11–19,32,36,37 Our results are thus generalisable to all countries where endoscopist accreditation is not the rule in CRC screening programmes, which includes the great majority of countries.12,13,19,32,36,37
Future research
Our observation that a minority of endoscopists penalise individuals who are invited to participate in the French organised CRC screening programme is not new; however no action has been taken to date to make any changes. 10 There is no certification maintenance process in France and the colonoscopy quality recommendations are non-binding. The poor quality of a number of colonoscopies is an issue in organised CRC screening programmes supposed to offer better quality assurance to screened populations than opportunistic screening. There seem to be two ways to eradicate these poor practices: a certification maintenance process and accreditation. Reduction of the percentage of low detectors should be a priority for quality improvement programmes as they are the main cause of post-colonoscopy CRC. 6 Several studies have demonstrated that it is possible to improve performance through well-designed training programmes. 38 The first step is feedback to endoscopists. In Alsace, since 2014, endoscopists are informed annually about their ADRs as measured for FIT-positive colonoscopies performed within the CRC screening programme. Their performances concerning CIR, ProxSLDR and rate of referral for surgery of benign-appearing polyps were added starting January 2021. If an accreditation process were introduced in France, it would have to include performance and volume criteria, both yet to be determined. In any case, the rather small number of colonoscopies performed by low-volume and low-performing endoscopists could be easily transferred to high-volume and high-performing endoscopists. Finally, comparison between countries is hampered by the heterogeneity of screening programmes, FIT brands and cut-offs, and the absence of consensual quality indicators, for example, for polypectomy competency assessment. A worldwide consensus on quality indicators for colonoscopy and CRC screening programmes is mandatory.
Conclusion
The overall good quality of the colonoscopies performed within the French CRC screening programme is penalised by a minority of poor-performing and/or low-volume endoscopists so that at least one in nine individuals undergoing a FIT-positive colonoscopy is not being given the best possible chances. Consequently, the benefit-risk and cost-effectiveness balances of the screening programme are significantly lowered. Our study demonstrates that colonoscopy can be a weak link in FIT-based CRC screening programmes. It gives health policy makers objective data to improve the organisation of screening programmes: mandatory endoscopist accreditation and a process of certification maintenance should be included in the specifications of any organised CRC screening programme, whatever the screening tool used.
Footnotes
Acknowledgements
The authors thank all the gastroenterologists, pathologists and general practitioners who participated in the CRC screening programme organized in Alsace. They also wish to express their deep gratitude to Dr Philippe Perrin for his invaluable assistance.
Authors’ contribution
Conceptualization: BD. Data curation, investigation: IG. Formal analysis: BD, IG, Writing: BD. Review of the analysis and of the content: all authors. Guarantor: BD.
Data sharing statement
All deidentified participant data are available upon reasonable request from IG. i.gendre@depistagecancer-ge.fr.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was performed as part of a quality assurance program within the CRC screening programme in Alsace without dedicated funding. The sources of funding of the screening programme include the French Sickness Fund (Assurance Maladie), the French Ministry of Health and the Haut-Rhin and Bas-Rhin Administrations (Conseils Départementaux du Haut-Rhin et du Bas-Rhin). They had no role in study design, data collection, analysis, and interpretation, or writing the report.