
Abstract
Background and aims
Colonoscopy following positive fecal occult blood screening may detect non-malignant polyps deemed to require major large bowel resection. We aimed to estimate the major inpatient morbidity and mortality associated with major resection of non-malignant polyps detected at colonoscopy following positive guaiac fecal occult blood screening in Ontario's population-based colorectal screening program.
Methods
We identified those without a diagnosis of colorectal cancer in the Ontario Cancer Registry ≤24 months following the date of colonoscopy prompted by positive fecal occult blood screening between 2008 and 2017, who underwent a major large bowel resection ≤24 months after the colonoscopy, with a diagnosis code for non-malignant polyp, in the absence of a code for any other large bowel diagnosis. We extracted records of major inpatient complications and readmissions ≤30 days following resection. We computed mortality within 90 days following resection.
Results
For those undergoing colonoscopy ≤6 months following positive guaiac fecal occult blood screening, 420/127,872 (0.03%) underwent major large bowel resection for a non-malignant polyp. In 50/420 (11.9%), the resection included one or more rectosigmoid or rectal polyps, with or without a colonic polyp. There were one or more major inpatient complications or readmissions within 30 days in 117/420 (27.9%). Death occurred within 90 days in 6/420 (1.4%).
Conclusions
Serious inpatient complications and readmissions following major large bowel resection for non-malignant colorectal polyps are common, but mortality ≤90 days following resection is low. These outcomes should be considered as unintended adverse consequences of population-based colorectal screening programs.
Keywords
Introduction
In 2008, Ontario introduced a population-based colorectal screening program, ColonCancerCheck (CCC), recommending biennial guaiac fecal occult blood testing (gFOBT) for asymptomatic persons 50–74 years of age without a first degree relative affected by colorectal cancer (CRC) in response to national guidelines 1 , 2 issued following publication of the meta-analysis of trials showing a reduction in CRC mortality with gFOBT screening. 3 Components and performance measures of CCC have been previously published. 4 , 5 CCC advises primary care physicians to refer patients with positive gFOBT results for diagnostic colonoscopy.
Among patients with positive gFOBT screening tests who are followed up with a diagnostic colonoscopy, many more will be found to have non-malignant colorectal neoplasia than to have CRC. In the first round of the Nottingham randomized trial, 0.21% of 40,214 screened had CRC detected compared to 0.77% who had adenoma detected: 3.7 screenees were detected with adenoma for every screenee detected with CRC. 6 In the first gFOBT screening round of the Scottish demonstration pilot, 0.21% of 167,415 had CRC detected whereas 0.65% had one or more adenomas detected: 3.1 persons were found to have adenoma for every person found to have CRC. 7 In initial screens performed by the English Bowel Cancer Programme, 0.185% (95% confidence interval (CI) 0.181%, 0.189%) of 4,218,309 screenees had CRC detected, whereas 0.542% (95% CI 0.535%, 0.549%) had high-risk adenoma and 0.308% (95% CI 0.302%, 0.313%) had low-risk adenoma detected: 4.59 persons were found to have adenoma for every person found to have CRC. 8 Non-adenomatous polyps were not tabulated in either study.
Three European gFOBT-based population-wide colorectal screening programs have described the frequency of major large bowel resection for gFOBT-detected non-malignant polyps. Le Roy et al. 9 report that 175/4251 (4.1%) persons with polyps, detected by a regional population-based gFOBT screening program between 2003 and 2012, proceeded to major large bowel resection, 24.0% of whom experienced postoperative complications and 0.5% of whom died postoperatively. Lee et al. 10 report that 121/557 (21.7%) persons with gFOBT-detected polyps between 2006 and 2009 by the English Bowel Cancer Screening Programme underwent surgical management, 25/121 (20.7%) of whom were found to have cancer in the surgically resected polyp. Postoperative complications were reported in 12/121 (9.9%) and postoperative death for 1/121 (0.8%). Marres et al. 11 report the early impact of the initiation of the fecal immunochemical test-based national bowel cancer screening program in the Netherlands on the frequency of surgical resection of non-malignant polyps. Between 2009 and 2013 there were 47 cases over five years; however, in the year of screening program initiation, there were 29 cases in a single year, which they attribute to the onset of screening. Over the entire six-year period, 9/76 (11.8%) experienced a serious postoperative complication and there were 2/76 (2.7%) postoperative deaths.
In the present study, we have undertaken to identify major large bowel resections for non-malignant polyps detected by gFOBT during the first 10 years of Ontario's CCC, in order to obtain more stable estimates of serious postoperative complications and postoperative mortality in a large cohort than are currently available in the published literature. These outcomes are harms potentially attributable to a population-based colorectal screening program.
Methods
This study was approved by the Research Ethics Board of Sunnybrook Health Sciences Centre, Toronto, Ontario (REB 396-2017). The work was performed at ICES (previously known as the Institute for Clinical Evaluative Sciences), where datasets described below were linked using unique encoded identifiers for analysis.
ICES received a database from Cancer Care Ontario containing all the gFOBT results from the CCC program, from its inception in 2008 to 2017. Among the individuals aged 50 to 74 whose records were contained in the database, we searched for the first ever record of a positive gFOBT result. We ascertained the sex of each person by linkage via encrypted personal identifiers with the Registered Persons Database (RPDB) maintained by the Ontario Health Insurance Plan (OHIP), operated by the government of Ontario and providing coverage to all permanent residents of the province. Further data linkage included the Ontario Cancer Registry, the Ontario Crohn's and Colitis Cohort Database, and the Canadian Institute for Health Information inpatient Discharge Abstract Database (CIHI DAD) of intervention codes and diagnosis codes.
We sought to identify those with a positive result who underwent colonoscopy within six months following the date of the positive gFOBT from the OHIP billing claims database, who ultimately underwent a major large bowel resection for benign colorectal polyp (International Classification of Diseases version 10 (ICD10) diagnosis codes D12.0, D12.2, D12.3, D12.4, D12.5, D12.6, D12.7, D12.8). Further criteria included the absence of colonic perforation at the time of colonoscopy, the absence of any other large bowel diagnosis codes at the time of resection, the absence of prior history of inflammatory bowel disease or total colectomy, and the absence of any record of CRC up to two years following the date of the first positive gFOBT.
In order to characterize the cases who underwent major large bowel resection for benign colorectal polyp, we calculated the five-year cumulative Charlson comorbidity score as of the date of the first positive gFOBT using the algorithm of the Deyo adaptation of the Charlson score for use with administrative data, which ICES has adapted for the Canadian usage of ICD10 diagnosis codes. 12 The score was dichotomized as zero versus greater than or equal to one. We determined the two-year cumulative Resource Utilization Band (RUB), a classification of health services utilization and level of morbidity, by running the Ambulatory Care Group program (www.acg) on the OHIP billing claims databases plus the CIHI databases. 13 We categorized the RUB as ‘zero utilization' (non-user) during the prior two years, plus utilization bands one to three combined (healthy users, users with low morbidity, and users with moderate morbidity) versus utilization bands four and five combined (users with high morbidity plus very high morbidity). To approximate socio-economic status (SES) of the cases, we linked residential code information from the OHIP RPDB to small area census information on rural versus urban residence, and among urban residences for the five urban quintiles of median household income. We grouped the three lowest income quintiles together and the two highest quintiles together, in order to avoid cell counts <6 for any covariate or outcome, publication of which is forbidden by the government of Ontario.
From the index CIHI DAD admission record and from any additional acute care hospital admissions at any Ontario acute care hospital ≤30 days following the major large bowel resection, we applied the algorithm for identifying major postoperative complications managed in hospital and also identifying readmissions within 30 days following major large bowel resection defined by Baxter. 14,15 We extracted from the CIHI DAD records and the OHIP billing claims database all the components of the algorithm (Canadian Classification of Interventions CCI intervention codes, ICD10 diagnosis codes, and OHIP billing claims). The major complications captured in the algorithm were reoperation (CCI intervention codes in CIHI DAD for surgical drainage, small and/or large bowel resection, stoma creation), sepsis (ICD10 diagnosis codes), abscess requiring percutaneous drainage (OHIP billing claims), major wound disruption (ICD10 diagnosis code for dehiscence or rupture of wound in CIHI DAD or CCI intervention code in CIHI DAD or OHIP billing claim for repair of abdominal muscles), wound infection (ICD10 diagnosis code in CIHI DAD for intra-abdominal, stitch, subphrenic or wound abscess not submitted to percutaneous drainage), hemorrhage (CCI intervention code for blood transfusion or ICD10 diagnosis code in CIHI DAD), and acute circulatory disorders recorded as ICD10 diagnosis codes in CIHI DAD (venous thromboembolism, stroke or transient ischemic attack, myocardial infarction and congestive heart failure). Less serious complications arising after discharge and not requiring readmission were not captured, because at present there is no algorithm to identify them in the ambulatory setting.
We calculated chi-square tests to compare those with at least one complication or readmission ≤30 days following major large bowel resection to those without, by anatomic site of polyp resection and baseline covariates. Based on the small sample size, we did not build a multivariate regression model.
From the RPDB we identified the date of death for all those who died ≤90 days following the date of major large bowel resection. As noted above, we are unable to report cell counts <6 and therefore we could not compare baseline covariate distributions between those who did or did not die ≤90 days after resection.
Results
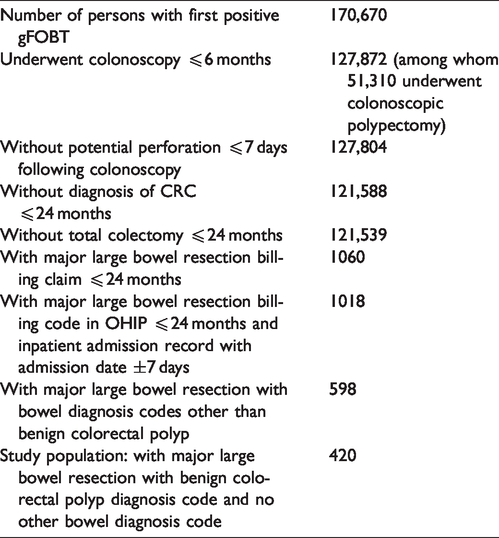
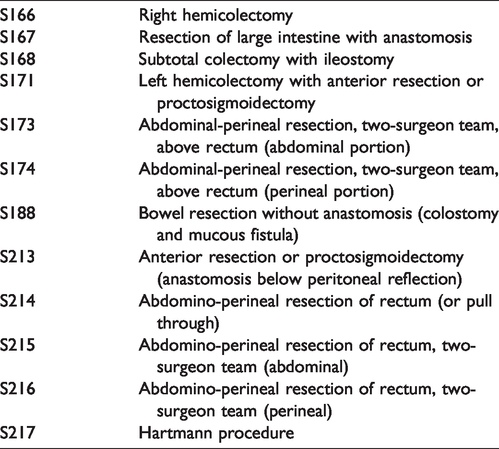
Table 1 displays the steps taken to identify the 420 persons who had a major large bowel resection for benign colorectal polyp in the absence of CRC or any other large bowel diagnoses among the 170,670 persons who had a first positive gFOBT result between 2008 and 2017, of whom 127,872 underwent colonoscopy within six months. The surgical codes for major large bowel resection are listed in Table 2. 16
Steps in identification of the study population.
Major large bowel resection billing codes.
The mean time from colonoscopy to major large bowel resection was 122.91 days (SD 126.52 days); median 80.5 days (interquartile range 96.5 days). To provide context for the 420 cases of major large bowel resection for benign colorectal polyp, we note that simple colonoscopic polypectomy (defined by OHIP billing claim Z571, excision of polyp between 0.3 and 2.9 cm in diameter) had been performed in 49,377 and complex polypectomy (defined by OHIP billing claim E685, total excision of sessile polyp >3 cm in diameter) in 1933 cases, compared to the 420 who underwent major large bowel resection. This means that the number of those proceeding to major large bowel resection represents 0.8% of all those who underwent any colonoscopic polypectomy, or, 21% of those who underwent total excision of sessile polyp >3 cm in diameter. Among those who underwent major resection, 370 (88.1%) had only colonic polyps.
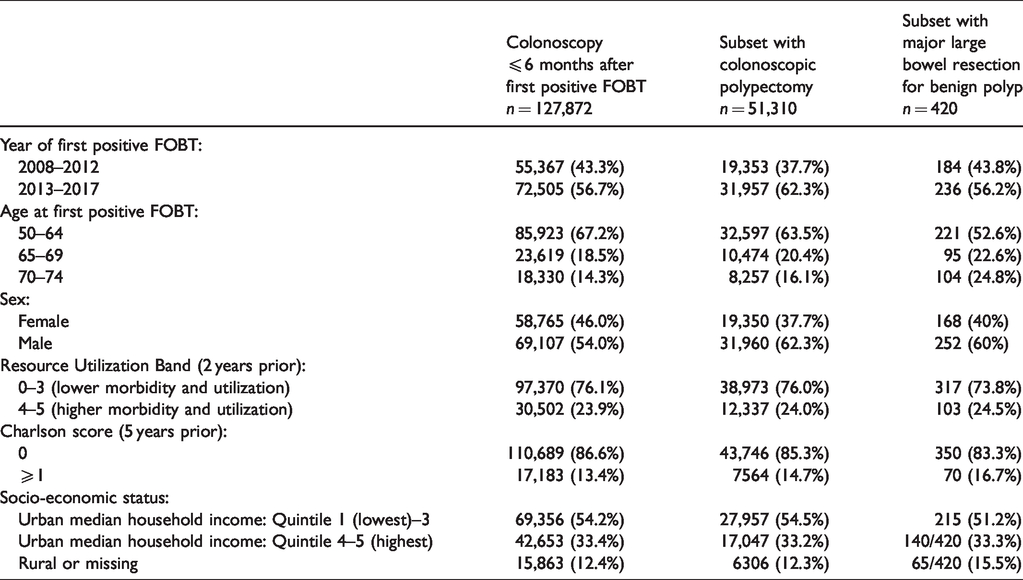
Table 3 describes the 127,872 persons who underwent colonoscopy ≤6 months after their first positive gFOBT result, the 51,310 persons who underwent colonoscopic polypectomy at the index colonoscopy, and the 420 persons who underwent major large bowel resection for benign colorectal polyp. Among these three categories, the subset with resection had the lowest percent of persons aged 50–64 and the highest percent 70–74 years. The percent of those who underwent colonoscopic polypectomy or major resection who were female was lower than the percent of females among the total population who had colonoscopy. There were numerically only minor differences in the percent of persons in the overall cohort or the two subsets for the categories of the RUB, the Charlson score, or SES.
Description of underlying population with first positive FOBT result plus colonoscopy and two subsets.
Overall, 117 (27.9%) experienced one or more major inpatient postoperative complications or readmissions ≤30 days following the date of major large bowel resection (Table 4). The most common events were major wound disruption (50, 11.9%) and readmission within 30 days following resection (46, 11.0%). Due to cell counts <6 for the following major complications individually, we cannot report: venous thromboembolism, sepsis, stroke/transient ischemic attack, myocardial infarction or congestive heart failure; however, these did contribute to the overall count of 117 cases with at least one complication and/or readmission within 30 days.
Major inpatient postoperative complications and readmissions within 30 days of major large bowel resection of non-malignant polyp.
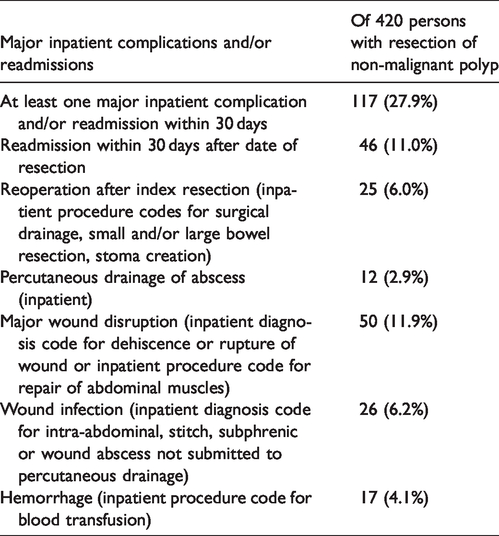
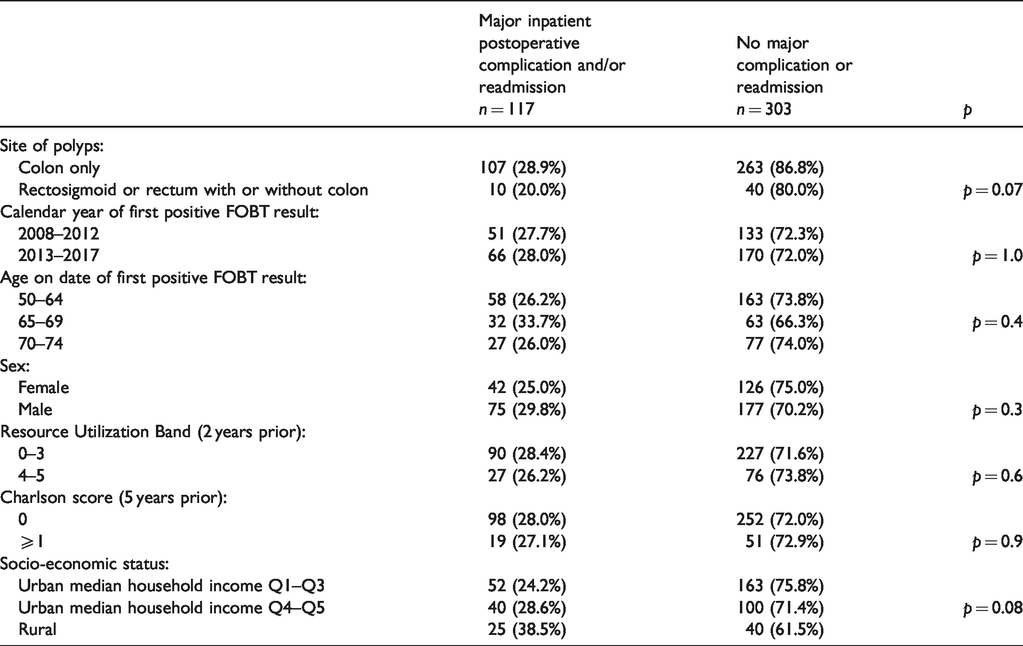
Table 5 shows the percent of persons with or without at least one major inpatient postoperative complication or readmission within 30 days of the date of resection, stratified by the limited number of covariates available. Chi-square tests on the percent of persons with at least one major complication or readmission for each covariate did not disclose any p values ≤0.05.
Any major inpatient complications and/or readmissions following major large bowel resection for benign colorectal polyp by baseline covariates.
Death within 90 days following major large bowel resection occurred in six cases (1.4%). We cannot report counts <6, so we are unable to describe the characteristics of those who died within 90 days or to report the number of deaths which occurred between 0 and 30 days after resection.
Discussion
In a population-based series larger than those previously published, we have demonstrated the occurrence of serious postoperative complications in 117 cases (27.9%) following major large bowel resection for non-malignant colorectal polyps detected by a gFOBT population-based screening program, although 90-day postoperative mortality is low (6 cases or 1.4%). Given that some of these polyps would not have evolved to CRC, or otherwise produced morbidity during the remaining life expectancy of some of the patients, the complications and mortality following major large bowel resection for non-malignant polyps may be considered a potential harm of population-based colorectal screening programs.
A large US study of surgery for non-malignant colorectal polyps, without information on method of detection, has revealed increasing rates between 2000 and 2014. 17 Peery et al. ascribe this to major increases in the use of colonoscopy for all indications including screening during that interval. US studies have also demonstrated rates of major postoperative complications between 14% and 25.3%,18–20 and mortality between 0.7% and 1.0%.18–20 A report on surgery for benign colorectal polyps, without information on method of detection, between 2005 and 2015 in the Noord-Holland province of the Netherlands 21 found that the rate was stable across the period, with 318/915 (34.8%) experiencing one or more adverse events and postoperative mortality in 13/915 (1.4%). By comparison, contemporary population-based reports of postoperative complications and mortality after resection of CRC, regardless of detection by screening or symptomatic presentation, report that from 19.4% to 33.9% experience major complications22–24 depending on age and institution characteristics, and that 1.0% to 6.7% of cases result in postoperative death, depending on age and definitions of the period of observation for postoperative mortality.25–31 At present, there are no publications on overall complications and mortality following major large bowel resection for CRC in Ontario during this observation period (2008 to 2017).
There is substantial variation in the definitions of postoperative complications among the screening-program based reports as well as among the overall population reports of major large bowel resection for non-malignant colorectal polyps. This makes it difficult to make meaningful comparisons of their frequencies. Nevertheless, it appears from our findings that the occurrence of major postoperative complications, other than mortality, following major large bowel resection for non-malignant colorectal polyp, detected during the evaluation of positive colorectal screening, may be similar to that following resection of CRCs overall.22–24 However, postoperative mortality following major resection of non-malignant polyps among participants in the population-based screening program CCC is somewhat lower than following major resection of CRC;25–31 this is also consistent with publications on major resection of non-malignant polyps which are not based on population-based screening programs.18–21
Towards the end of this observation period, initiatives to improve the quality of major large bowel resections for CRC were introduced in Ontario. 32 , 33 If they are shown to be successful in the future, they would likely improve the quality of major large bowel resections for benign colorectal polyps as well.
Identification of major postoperative complications following major resection of non-malignant polyps using administrative databases is characterized by limitations as well as strengths. There is the possibility that for some subjects the codes used in our algorithm may have been assigned erroneously or omitted. On the other hand, because the administrative databases include all hospitals in Ontario, we were able to capture readmissions with complications ≤30 days following resection at any hospital in Ontario, not simply at the hospital at which the resection was performed.
We have no information about the histology, diameter, or other characteristics of these surgically resected lesions detected by the CCC program, nor about the characteristics of lesions among the persons treated by colonoscopic polypectomy following their first positive CCC gFOBT screening result. Therefore, we cannot judge whether any of the 420 cases could have been managed endoscopically, unlike others who have compared major surgical resection to colonoscopic resection in single-institution populations of patients with colorectal polyps unstratified by method of detection. 34
Conclusion
Serious complications and readmissions following major large bowel resection for non-malignant colorectal polyps are common; however, mortality ≤90 days following resection is low. These outcomes should be considered as unintended adverse effects of a population-based colorectal screening program, but may be amenable to quality improvement initiatives directed at major large bowel resections overall.
Footnotes
Acknowledgements
The opinions, results, and conclusions reported in this article are those of the authors and are independent from the funding sources. No endorsement by ICES or the Ontario MOHLTC is intended or should be inferred. Datasets were linked using unique encoded identifiers and analyzed at ICES from the Ministry of Health and Long Term Care of Ontario (RPDB and OHIP), and Cancer Care Ontario (OCR). The opinions, results, views, and conclusions reported in this paper are those of the authors and do not necessarily reflect those of the ICES, the Ministry of Health and Long Term Care of Ontario, or Cancer Care Ontario, and no endorsement by these bodies is intended or should be inferred.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: At the time of data analysis, Rinku Sutradhar, Nancy Baxter, Jill Tinmouth, and Linda Rabeneck were employees of Cancer Care Ontario, which operates ColonCancerCheck. Lawrence Paszat received an operating grant from Cancer Care Ontario to conduct this work. Jin Luo has no declaration.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health and Long-Term Care (MOHLTC). This work was funded by Cancer Care Ontario.