
Abstract
Objective
To estimate the proportional incidence (PI) of first- and second-year interval breast cancer among women aged 45–49.
Methods
In the Emilia-Romagna Region (northern Italy), women aged 45–49 are invited to mammography screening annually, and women aged 50–74 biennially. For younger ones, the proportional incidence of interval cancer in the first and unique interval year was calculated using standard methods. For the second, hypothetical year, it was estimated using two different estimates of the ratio between the second- and the first-year proportional incidence observed among women aged 50–54. Overall, 567,151 negative mammography records were used.
Results
In the first interval year, the observed proportional incidence of interval cancer among women aged 45–49 was 0.27 (95% confidence interval (CI), 0.22–0.33), within the European limit considered desirable for women aged 50–69 (<0.30). In the second, hypothetical interval year, the estimated proportional incidence ranged from 0.61 (95% CI, 0.43–0.86) to 0.48 (95% CI, 0.31–0.76) depending on whether the estimate was based on data from the pre-digital or digital era, respectively.
Conclusion
The more up-to-date estimate of 0.48, slightly below the maximum limit considered acceptable for women aged 50–69 (<0.50), suggests that a screening interval of two years may also be an acceptable option for women aged 45–49.
Introduction
For women aged 45–49 at average risk of breast cancer, the recent guidelines from the European Commission Initiative on Breast Cancer (ECIBC) recommend either triennial or biennial mammography over annual mammography. 1 This recommendation, referred to as a conditional one, is based on a ‘… very low …’ level of evidence. According to the ECIBC Guidelines Development Group, little information is available – in particular – on interval cancer. The conclusion is that ‘… this information should be shared’. We interpret these words as an invitation to all who have observational data on this topic to make them known. We briefly report a study on the proportional incidence (PI) of interval breast cancer among women aged 45–49 in an Italian mammography screening programme.
Methods
Since 1996, after some small pilot studies in 1995, women aged 50–59 living in the Emilia-Romagna Region (northern Italy) have been targeted by a biennial mammography screening programme. The PI of interval cancer has been the subject of two previous large studies.2,3 In 2009, in accordance with the Italian guidelines, 4 women aged 45–49 were included in the target population with a screening interval of 12 months. Invitation letters began to be sent in 2010. 5 An overview of performance measures of the screening process among newly invited women has been published. 6
The PI of interval cancer, or the ratio between the number of cancers observed in the inter-screening interval after a negative mammography result and the number of cancers that would be expected in the absence of screening, provides an approximation of one minus mammography sensitivity. The study was designed based on two considerations: (1) the PI in the second interval year increases invariably because mammography sensitivity for cancers in the penultimate year of their preclinical phase is lower; and (2) the ratio between the PI in the second versus the first interval year in the adjacent age group of 50–54 provides an acceptable estimate of the increase that would occur in the second interval year among women aged 45–49 if these were invited to screening biennially.
The objectives of the study were (1) to calculate the PI in the first interval year for women aged 45–49 using standard methods, (2) to estimate the PI in the second, hypothetical interval year using the PI observed among women aged 50–54, and (3) to contrast the two figures with the standards put forth by the European guidelines of 20067 (not yet updated by the ECIBC). We performed a sensitivity analysis according to different scenarios. For women aged 50–54, we calculated three sets of PI data. Two of these were based on the same datasets of our previous studies, covering the years 1997–20022 and 2003–2008. 3 The third one was based on newly collected data for the years 2010–2015. We calculated three ratios between the second- and the first-year PI. Finally, we multiplied the highest and lowest ratios by the first-year PI observed among younger women in 2010–2015. In this way, we obtained an estimate of the hypothetical second-year PI.
For the years 1997–2002 and 2003–2008, we retrieved the two original datasets. For the years 2010–2015, we collected the data according to the same methods in a sample of 4/11 screening centres. We created three datasets with a total of 567,151 negative mammography records. In all of these time periods, interval cancers were identified through record linkage between the original screening mammography files and the regional breast cancer registry. Local screening centres were asked to run manual data checks against the service databases for failed matches, partial matches, successful matches with contradictory information, and multiple matches. Extensive details can be found in one of the previous studies. 2 The study protocol was approved by the Ethics Committee at the Romagna Cancer Institute (ID: IRST100.37).
Data analysis was based on the same methods as in our previous studies except for the calculation of the expected incidence. In the first study, we used the pre-screening rates (1991–1995). 2 In the second study, we used the regional incidence rates generated by a model (MIAMOD) from the Italian National Institute of Health, which is based on a back-calculation approach to project the incidence of chronic diseases from mortality and patient survival. 3 In the present study, considering the length of screening exposure, the expected incidence among women aged 50–54 was estimated by analysing the annual rates in the years 1986–2014 with an age-period model (negative binomial regression) in which the period effect was enforced to be linear. As regards the estimate of expected incidence among women aged 45–49 in their first and unique interval year, the rates in the years 1995–2009 were analysed with a log-linear Poisson model. To determine the expected number of cancers, the expected incidence rates were multiplied by the appropriate number of woman-years. The observed number of interval cancers was divided by the expected number to obtain their PI. The 95% confidence interval (CI) around the observed:expected ratio was estimated using Byar’s approximation. The ratios between the second-year and the first-year PI were calculated using standard methods.
Results
In their first and unique interval year, the PI of interval cancer for women aged 45–49 was 0.27 (95% CI, 0.22–0.33).
Table 1 shows the observed PI of first- and second-year interval cancer for women aged 50–54. For both measures a decrease occurred over time, with values of 0.19 and 0.34 in 2010–2015 – the period in common between the two age groups. Also shown in Table 1 are the three ratios between the second- and the first-year PI. The highest ratio was 2.24 and the lowest, which was based on the most recent screening period, was 1.79. These were multiplied by the first-year PI observed among women aged 45–49. The resulting estimates of the second-year PI, as shown in the right-hand column of Table 1, were 0.61 and 0.48, respectively.
First- and second-year proportional incidence (PI) of interval breast cancer among women aged 50–54 and estimation, under two scenarios, of the second-year PI that would be expected among women aged 45–49 if they were invited to screening biennially.
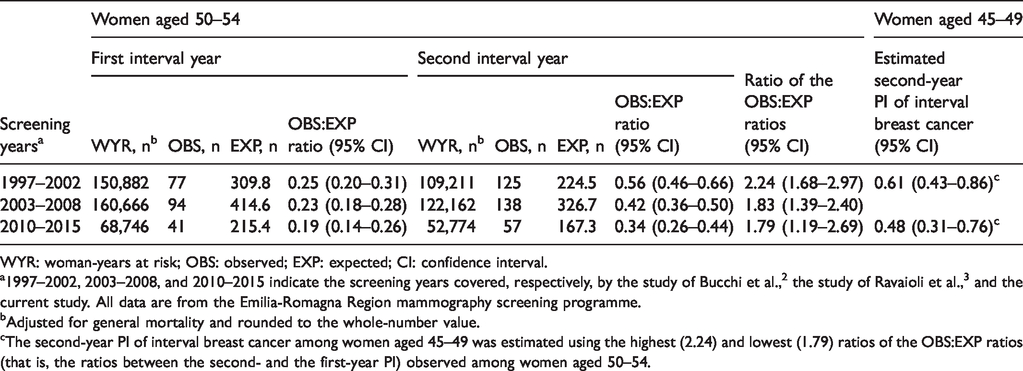
WYR: woman-years at risk; OBS: observed; EXP: expected; CI: confidence interval.
a1997–2002, 2003–2008, and 2010–2015 indicate the screening years covered, respectively, by the study of Bucchi et al., 2 the study of Ravaioli et al., 3 and the current study. All data are from the Emilia-Romagna Region mammography screening programme.
bAdjusted for general mortality and rounded to the whole-number value.
cThe second-year PI of interval breast cancer among women aged 45–49 was estimated using the highest (2.24) and lowest (1.79) ratios of the OBS:EXP ratios (that is, the ratios between the second- and the first-year PI) observed among women aged 50–54.
Discussion
In the time period in common, the PI of first-year interval cancer at age 45–49 was greater than at age 50–54, i.e., 0.27 versus 0.19, but still within the limit considered desirable by the European guidelines of 2006 for women aged 50–69, i.e., <0.30. 7 In the second, hypothetical interval year, the estimate varied from 0.61 to 0.48. These figures are above and, respectively, slightly below the maximum limit considered acceptable for women aged 50–69, i.e., <0.50. A key finding was that the PI of interval cancer among women aged 50–54 decreased over time, most probably resulting from the gradual transition to digital mammography, 8 a process which was completed in 2010. It appears that the estimate of 0.48 is more up-to-date, but of course further confirmatory data are needed. At present, we are not aware of any other published study that has dealt with the topic of incidence of first- and second-year interval breast cancer in women aged under 50.
As regards the study design, we expected that the large increase in mammographic workload, which is described elsewhere, 5 would cause a substantial phenomenon of delays in the invitation schedule. Consequently, we planned to calculate the second-year PI of interval breast cancer in a direct manner rather than with an estimate. The frequency of delays, in fact, was too low and their duration too short. This prevented us from using this approach.
In addition to the general limitations of PI data discussed elsewhere, 3 two methodological issues deserve a mention. First, we estimated the expected incidence using different methods depending on the different lengths of screening exposure. In the early study, 2 covering the first years of the programme, the approach of using pre-screening rates was sufficiently robust. In the second study 3 and in the present one, performed many years later, we decided to use modelling methods. In any case, the expected incidence remains a problematic issue in this type of design. 3 Second, we assumed for younger women that the rate of increase in PI in the second interval year, if they were invited to screening biennially, would be comparable with that observed in the adjacent age group. This implies similar growth rates for cancers undetected by mammography. Some studies provide evidence against this assumption,9,10 but they compared very large age groups – for example, 40–49 years versus 50–79. 10 Within an age range as narrow as from 45 to 54, the gradient of tumour behaviour is necessarily much less pronounced.
In conclusion, annual screening of women aged 45–49 has a satisfactory level of sensitivity, and a screening interval of two years appears to be an acceptable option. It must be noted that this study is only an initial contribution to bridge the knowledge gap on this topic.
Footnotes
Acknowledgements
The authors acknowledge the contribution made by the Emilia-Romagna Region Workgroup for Mammography Screening Evaluation in conducting the previous two studies,2,3 the results of which were partly used for the present estimates. The membership of the Emilia-Romagna Region Workgroup for Mammography Screening Evaluation is reported elsewhere. 6
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.