
Abstract
Objective
To describe how three English breast screening services responded to the 2018 Patient Notification Exercise, a national intervention whereby women who had potentially missed their final screening invitation were offered new appointments. To compare key performance indicators for women thus invited with key performance indicators for women invited routinely in the same period.
Methods
Uptake, assessment and cancer detection for 9439 women aged over 70 in the Patient Notification Exercise were compared with key performance indicators for 14,824 women, of similar age, who were routinely invited in the same period, using chi squared (χ2) tests. Invitation cancellation and attendance levels were also compared.
Results
Uptake was significantly lower among Patient Notification Exercise women sent a new, timed appointment than for women who were routinely invited (67.3% and 70.8%, respectively, p = 0.001). Assessment rates were higher for Patient Notification Exercise women (5.2% vs. 4.4%, p = 0.192) as were cancer detection rates (1.87% vs. 1.28%, p = 0.080). Services achieved national round-length standards for routine invitations during and after the Patient Notification Exercise but screen-to-assessment standards were breached (80%) in the smallest service. More Patient Notification Exercise women than routinely invited women rebooked appointments (43.6% and 33.2%, respectively); they were also slightly more likely to miss their appointments (24.5% vs. 21.2%).
Conclusions
Screening invitation performance can be maintained whilst responding to an additional demand of ∼5%. Larger services that cover a compact geographical area may find it easier to respond. Women affected by the incident are not more likely to attend but may require relatively more assessment capacity in incidents where invitations have been delayed.
Introduction
The NHS breast cancer screening programme (NHSBSP) in England and Wales was established in 1988 to reduce morbidity and mortality from breast cancer. An independent review of evidence, published in 2013, estimated that breast screening in women over 50 years of age reduced mortality from breast cancer by 20% (corresponding to one breast cancer death prevented for every 235 women of age 50 years who are invited to screening for the next 20 years). 1 The NHSBSP currently invites women aged between 50 years and their 71st birthday for digital screening mammography every three years, at one of 78 local screening services. In addition, around 50% of women aged 71–73 are also invited as part of an age-extension (AE) trial. Other women over 70 years may optionally contact the service for a “self-referred” (SR) screening appointment.
In 2018–2019 the NHSBSP invited 2.93 million women in England for a screening mammogram at their local breast screening service 2 but during this period significant problems were encountered as a result of a perceived failure in the programme. On 2 May 2018, the then Secretary of State for Health and Social Care, Jeremy Hunt, announced in the House of Commons that there had been ‘a serious failure … in the national Breast Screening Programme’, 3 impacting all screening services in England and affecting women who may have missed their final invitation to screening between their 68th and 71st birthday. He suggested that between 135 and 270 women may have had their lives shortened as a result of the mistake. 3 The advisory group set up at the time estimated that between 150,000 and 200,000 women were affected by the incident. Local breast screening units were made aware of this via a formal notification on the day of the announcement. This notification set out deadlines for local units to ensure that all the women affected would receive their screening as quickly as possible. Screening services were asked to ensure that they had capacity available for inviting affected women, although the actual demand for screening in each service did not become clear for a further two weeks. Weekly ‘capacity and progress’ meetings were held between breast screening service providers and local commissioning teams. The response to this incident was known as the ‘Patient Notification Exercise’ (PNE).
All breast screening services were tasked with offering additional screening to women identified as having missed their final invitation, 4 with the additional expectation from NHS England and Improvement (NHSEI) that the response should not compromise the core service and performance for routinely invited women. The main KPIs likely to be affected were: round length (ensuring that women are invited within 36 months of their previous screen), uptake (ensuring that at least 70% of women invited attend their screen), and time from screen to assessment for women requiring further tests (must be within three weeks of the screening date). 5 In addition, the public announcement of the incident was expected to generate increased public awareness of screening, which might lead to an increased number of women (not affected by the screening incident) contacting the screening service for an optional SR appointment.
Two different cohorts were selected by NHS Digital in May 2018 to include women identified by Public Health England as having missed their final invitation for screening (see Annex C of Thomas et al.
4
for details of the selection algorithm):
women aged 70+ who had not reached their 72nd birthday on 1 April 2018 (<72 cohort) women over the age of 72 but not yet reached their 80th birthday on 1 April 2018 (72+ cohort).
A letter was sent by Public Health England to each woman affected outlining the problem that had arisen. Separate files (known as ‘batches’) of the women in each cohort were sent to the relevant local screening service by NHS Digital so that women could receive their missing invitation from the correct screening service. It was determined that younger women (<72) would receive an automatic invitation to re-screening whereas those older (72+) should be offered the choice of a re-screen and could call the national helpline to request an appointment.
The result of the announcement was to trigger:
considerable pressure to increase and accommodate the anticipated additional workload as soon as possible, increased capacity planning and scheduling, increased administrative work, screening and assessment activities.
Previous changes in the NHSBSP have resulted in larger, long-term increases in screening workload. For example, Patnick et al. report that the move from single to double view mammography required ∼15% additional capacity but this was phased in over a longer period (September 2000 to December 2003) and new methods of working were able to be introduced. 6 The NHSBSP has never previously been asked to respond at short notice to a nation-wide incident as large as that which triggered the PNE. The authors are not aware of any other studies that have looked at the impact on capacity planning and performance of an incident of this magnitude on a national breast screening programme (or any other fully operational, population-based screening programme).
The objective of this paper is to describe how three local breast screening services, from different parts of England, responded to the increased demand arising from the PNE and to compare the KPIs for women invited as part of that intervention (PNE cohorts) to women invited routinely in the same period. Similarly, the invitation cancellation and re-booking behaviour of women in that period is analysed to see whether the PNE women required a different degree of re-booking support.
Methods
Participants
We reviewed and examined three breast screening services from three different regions: London, South East England and South West England. They were managed by the same NHS Breast Screening Service provider and whilst locally they were clinically led, had the same internal incident management response team, resources and support available to them.
The three breast screening services were:
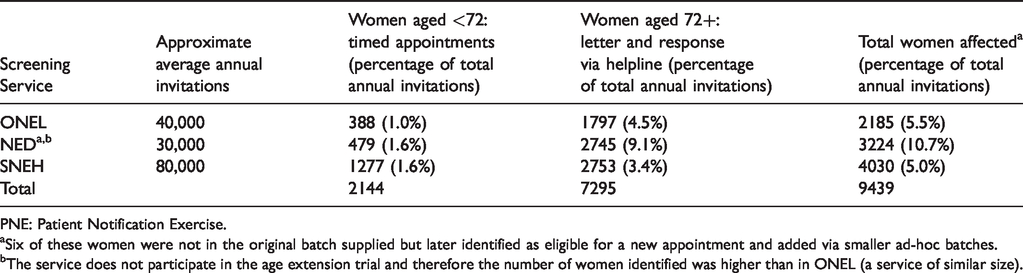
Outer North East London (ONEL), which provides breast screening for women on behalf of primary care services for Barking and Dagenham, Redbridge and Havering. This service invites ∼40,000 women aged between 47 and 73 from this predominantly urban area for breast screening each year. To enable women to be screened closer to home, breast screening is carried out at five sites across the region; three of these sites are static (permanent buildings) and two sites are served by a single mobile screening van. This service participates in the NHSBSP Age Extension (AE) trial, which involves inviting a random sample of 50% of women over the age of 70 for an extra three yearly mammogram before their 73rd birthday. Therefore, around 50% of the women potentially affected by the PNE incident had already been invited for an additional screen, reducing the potential total number affected. Numbers of women affected by the PNE for each service.
a
PNE: Patient Notification Exercise. aSix of these women were not in the original batch supplied but later identified as eligible for a new appointment and added via smaller ad-hoc batches. bThe service does not participate in the age extension trial and therefore the number of women identified was higher than in ONEL (a service of similar size).
Surrey & North East Hampshire (SNEH), commonly known as ‘the Jarvis’. This service is one of the largest in England and provides breast screening for women living in Surrey and North East Hampshire, inviting ∼80,000 women each year (aged 47–73) and covering a predominantly semi-rural population, with a lower average level of deprivation than either of the other participating screening services. Breast screening is carried out at the main static unit or in one of five mobile vans, which move around the area on a three yearly rotation across 19 different sites. Like ONEL this service participates in the AE trial.
Table 1 provides an overview of the number of women affected by the PNE at each of the three participating services.
Almost 10,000 women were affected across the three services. Information about these women was received from NHS Digital and included the following elements:
<72 cohorts were provided to all screening services from 11 May 2018 through a single batch file. 72+ cohorts were distributed to the screening services via two routes ○ indicative numbers were shared, i.e. on 23 May 2018 ○ a single batch file was sent to the screening services, i.e. on 25 May 2018.
Data extraction
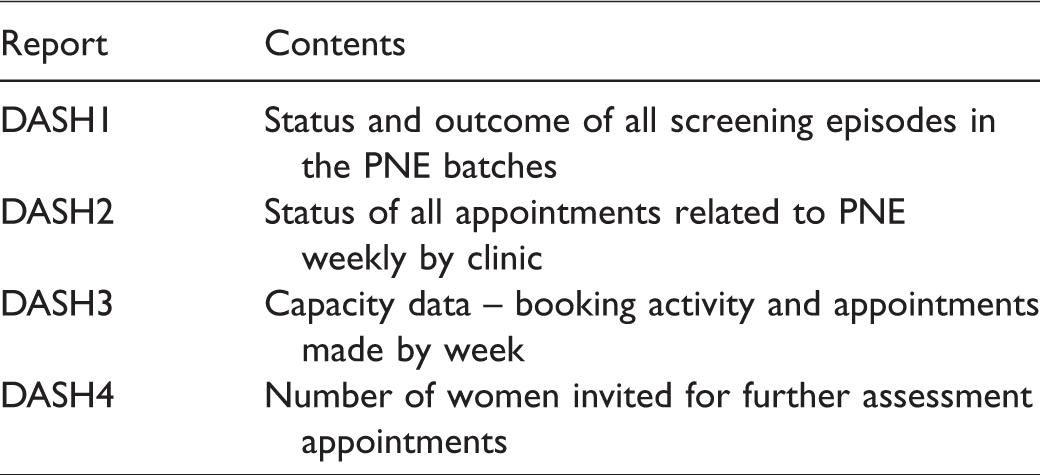
The extracts were collated centrally at NHS England and a weekly status summary “Dashboard” was provided to the Screening Services until October 2018. We used the final Dashboard dated 16 October 2018 as the main data source for PNE women in this paper.
Alongside this, we created one-off data extract reports which were run at each of the three screening services to extract summary data on the PNE and non-PNE screening invitations, for screening episodes where the date of the first offered appointment was in the period 01 April 2018 to 31 March 2019. This was done to allow a more detailed comparison of PNE and non-PNE activity.
We collected nationally published statistics 2 for the participating screening services for the two quarters during and following the PNE incident, i.e. July–September (Q2) and October–November (Q3), to show possible impact on round length and ‘screen to Date of First Offered Assessment (DOFOAss)’ performance.
Measures
The following key measures were calculated for each of the PNE cohorts and for the routinely invited screening women in each of the three participating services for the period 01 April 2018 to 31 March 2019 (unless stated):
Percentage of attendance (known as uptake, the number of eligible women with technically adequate screen, within six months of the date of their first offered screening appointment) – the proportion of all women with a first invitation date in the same period (acceptable national standard ≥70.0%; achievable level: ≥80.0%).
5
Quarterly round length, July–December 2018 – the percentage of women (age 50 to <71) whose first offered screening appointment is within 36 months of their previous screen (acceptable standard >90%; achievable level 100%).
5
Screen to DOFOAss, July–December 2018 – the percentage of women who require further tests, offered an assessment appointment within three weeks of attendance for the screening mammogram (acceptable standard >98%; achievable level 100%).
5
Referral to assessment rate – the proportion of women with a technically adequate screen who are referred for assessment (acceptable standard <7%; achievable level <5%).
5
Cancer detection percentage – the proportion of women screened in each cohort who were found to have breast cancer. Routine screening invitations – the number of non-PNE women who were invited for routine screening each month. Self-referral episodes – the number of non-PNE women (outside the normal invitation age range) who contacted the screening service each month for an optional screen.
Analysis
We complied a monthly breakdown of activity during the main phase of PNE and its aftermath (May to December 2018) to show how each of the screening services responded in terms of number of invitations per month, with activity broken down into the type of invitation (PNE, routine), and to give a comparison with the volumes of non-PNE self-referrals received per month.
We categorised women according to whether they were routinely invited, self-referrals or whether they were in one of the two PNE cohorts (i.e. <72 or 72+). Routinely invited and self-referred women under the age of 70 were excluded from the comparative analyses so that comparisons could be made between women of a similar age. The <72 PNE cohort was compared to routinely invited women aged 70+ because the mechanism for invitation (an offer of a timed appointment) was the same. For the same reason, the 72+ PNE cohorts were compared to the group of women over 70 who self-referred. The results were further stratified by individual screening service.
We compared the overall screening behaviour and outcomes for different cohorts in terms of: percentage attended, percentage assessed and percentage of cancers detected. Pearson's chi-squared tests (χ2) were carried out to test the null hypothesis that there were no differences in these measures between women in the PNE batches and women routinely invited. In all the analyses, we considered statistical significance (2-sided) at p-value < 0.05. All analyses were conducted in MS Excel.
Women may cancel and rebook several appointments before they finalise their screening. Therefore, we also compared the individual appointment status (attended, cancelled) for women in the PNE cohorts with the booking and attendance behaviour of women routinely invited in the same age group (70+) and also with women routinely invited who were younger (<70) by calculating the proportions of appointments that were: not attended (did not attend, DNA), cancelled and re-booked in each group.
Results
KPIs for a total of 9439 PNE women were compared to KPIs for 14,824 women, of similar age, who were routinely invited in the same period.
Overall uptake of 67.8% was significantly lower among PNE women <72 sent a timed appointment, than for women of a similar age who were routinely invited (70.8%); χ2 (degrees of freedom (df) = 1, n = 11,432) =10.4, p < . 001. This pattern of uptake difference was repeated in each individual screening service (although the difference was non-significant for SNEH) (Table 2).
Performance overview by screening service and method of invitation (01 April 2018 to 31 March 2019).
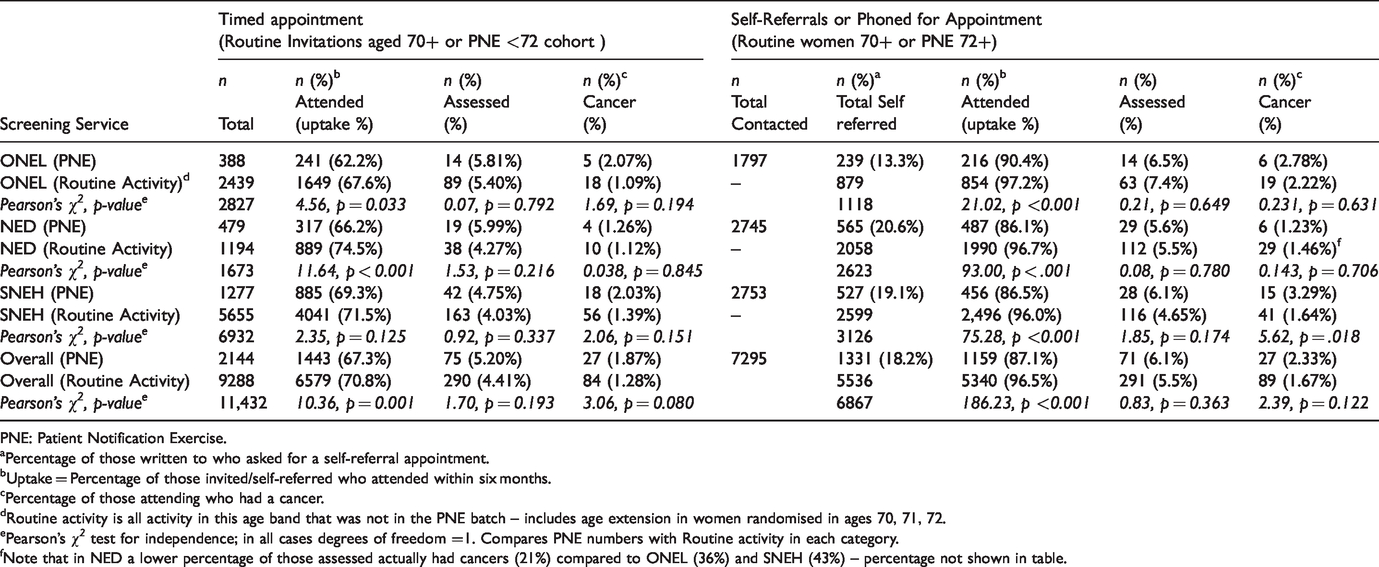
PNE: Patient Notification Exercise.
aPercentage of those written to who asked for a self-referral appointment.
bUptake = Percentage of those invited/self-referred who attended within six months.
cPercentage of those attending who had a cancer.
dRoutine activity is all activity in this age band that was not in the PNE batch – includes age extension in women randomised in ages 70, 71, 72.
ePearson’s χ2 test for independence; in all cases degrees of freedom =1. Compares PNE numbers with Routine activity in each category.
fNote that in NED a lower percentage of those assessed actually had cancers (21%) compared to ONEL (36%) and SNEH (43%) – percentage not shown in table.
Of PNE women contacted in the 72+ group, 1331 (18.2%) asked for an appointment (Table 2). The overall uptake of 87.1% was significantly lower than among women of similar age who self-referred routinely (96.5%); χ2 (df = 1, n = 6867) =186.3, p < . 001 (Table 2), and this was true across all services.
In contrast, assessment rates were higher among PNE women than for the routinely invited women in both invitation categories (5.2% and 4.4% overall for the younger age group and 6.1% and 5.5% for the older group, respectively; Table 2). This pattern was broadly the same across all services, although the differences between PNE and routine batches were not significant. Likewise, cancer detection rates were higher among the PNE women than routinely invited women in both invitation categories (1.87% and 1.28% for the younger age group and 2.33% and 1.67% for the older group, respectively; Table 2) but the differences were non-significant.
Despite the increase in workload, all three services achieved the nationally acceptable invitation round length for routine activities during and after the PNE (Table 3). ONEL and SNEH also achieved DOFAs standards during the whole period but NED dipped to 80% in September–December 2018. Note that the volume of PNE batches (∼10% relative to overall service volumes) in NED was relatively high in comparison to the other services (∼5%), a result of not being included in the AE trial.
Key programme performance indicators (July–December 2018).

Figure 1 shows that all three screening services were able to offer the majority of PNE women an appointment within three months of the announcement. ONEL was able to respond quickest (possibly reflecting the fact that the largely urban population is invited to static sites). Both SNEH and NED had secondary peaks that reflected van moves to a more dispersed population. At the peak of PNE activity, routine activity in all services dipped, but in each service this was followed by a compensatory increase in routine activity which ensured that there were no round length breaches.
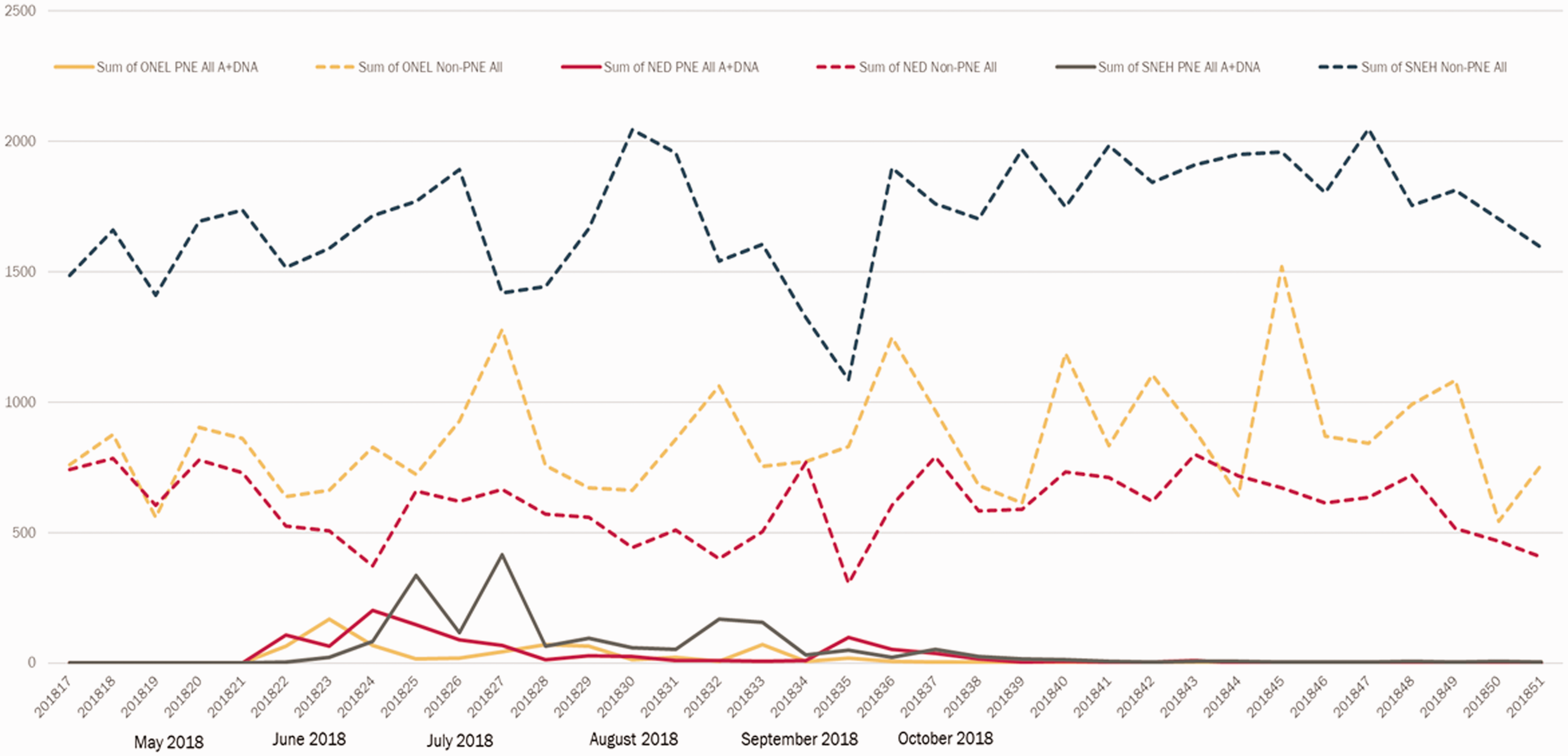
Weekly invitations for PNE women and routine activity (May–December 2018) in the three services. PNE includes women invited from both <72 and 72+ cohorts. Routine activity includes A (attended) and DNA (did not attend) appointments, and both routine invitations and self-referral appointments, of all age groups. PNE: Patient Notification Exercise.
Overall, women in the PNE batches were more likely to cancel and/or rebook their appointments than routinely invited women in the same age group (43.6% and 33.2%, respectively; Table 4). PNE women were also slightly more likely to DNA their appointments than routinely invited women in the same age group (24.5% vs. 21.2%) but much less likely to DNA than younger women who are routinely invited (37.7%; Table 4).
Appointment attendance and rebooking activity: PNE appointments and routine appointments (01 April 2018 to 31 March 2019).
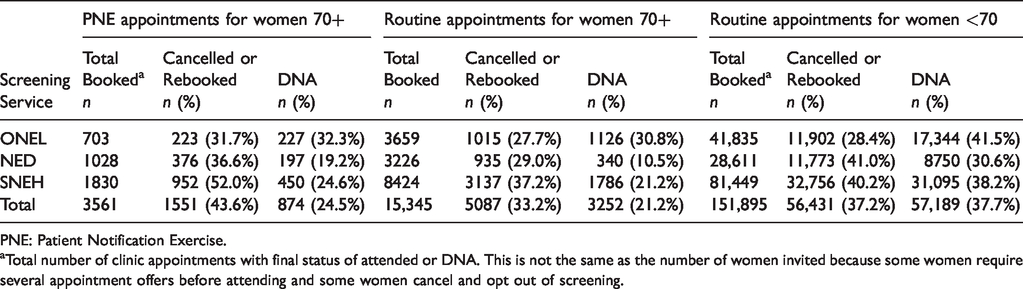
PNE: Patient Notification Exercise.
aTotal number of clinic appointments with final status of attended or DNA. This is not the same as the number of women invited because some women require several appointment offers before attending and some women cancel and opt out of screening.
After the House of Commons announcement at the beginning of May 2018, there was a small spike (∼35%) in non-affected women contacting the services for an appointment, but the number of self-referrals was back at average levels within three to four months (Figure 2).

Monthly self-referral activity (April 2018–November 2018) for all three services.
Discussion
Despite the high-profile announcements and media coverage that accompanied the declaration of the NHSBSP screening invitation incident, 7 the uptake of appointments for women in the PNE cohorts was lower than the attendance of women of a similar age, who were routinely invited in the same year. At the same time, PNE women were more likely to change their appointment. The overall assessment rates and cancer detection rates for women in the PNE groups were higher than for routinely invited women. This is likely to be a reflection of the fact that, whilst routine women were all invited within three years of their previous screen, many of the PNE women had not received a screen for over three years (individual data not available).
Our report shows that all three services acted quickly to re-invite women affected by the PNE. Services which are mainly based around static screening units (like ONEL) may find this easier because the women can always be invited to a screening site that is within a reasonable distance from their home. The rural service, NED, was not able to offer this for all women and some invitations were delayed until August 2018 when a screening van could be moved locally. All three services were able to increase capacity to meet the additional demand without compromising the round length for women routinely invited. This was particularly onerous for NED because the number of women affected represented a larger proportion of their routine activity. However, despite the wide media coverage, <20% of the women who were contacted in the 72+ group requested an appointment, which meant that the overall impact was <5% additional activity over the year. All three services responded to a spike in PNE activity by reducing routine activity but compensated over the following months to ensure that the overall round plan was not jeopardised. This shows that well-managed services can tolerate surges in invitations of this magnitude without compromising round length and long-term stability. Stavropoulou et al. 8 in their systematic review pointed out that incidents can be more effectively managed if they have clinical ownership and are integrated within the wider organisational safety programme, and this was the case with the three services included in this study.
Assessment appointment capacity was more difficult to manage because the PNE women were more likely to require assessment and more likely to have a cancer. This resulted in local difficulties in NED where DOFOAss standards were not met in October–December 2018. (This was also exacerbated by local equipment problems and subsequent cancellation of assessment appointments.)
Immediately following the announcement of the incident, there was a moderate increase in the number of women contacting the screening services to request an optional (self-referred) appointment. However, this surge declined as public awareness declined and the rates of self-referral were back to normal within three to four months. This mirrors similar findings following other high profile cancer stories.9,10
It can be argued that in a ‘smaller’ screening service, such as NED, the impact of unplanned downtime, e.g. equipment breakdown, staff sickness, is more severe than in larger services. Local variations in service and demography also impact the magnitude of different incidents; NED assessed nearly twice as many women as ONEL (a service of similar size). This is largely because it has a slightly older local population and does not take part in the AE trial, and therefore a relatively high number of PNE women were identified as having missed their final screen. NED probably compensated by having a lower assessment rate for the 72+ PNE cohorts in comparison with the other two services, although it is not clear to what extent this is a reflection of the pressure on assessment enforcing different behaviour in the radiological team.
In the sub-analyses, the low volumes of cases and small differences between rates meant that tests of statistical significance are not very meaningful. In practice, however, small differences in assessment rates can have an important effect on the capacity requirements for clinics, and therefore analysis of a much larger number of services would be advisable when making any general recommendations. The characteristics of the cancers detected were not available, but it would potentially be of interest to compare the histopathological and tumour characteristics (e.g. size, grade, lymph node involvement) of cancers detected in the PNE cohort with those of women of the same age group who were routinely invited. The authors acknowledge that a limitation of our study is that only three breast screening services were examined, and suggest that future studies should review the impact of the PNE across all breast screening services nationally.
We also acknowledge that the PNE demand represented a relatively small overall proportion of annual screening activity (∼5% of annual capacity) and whilst some of the conclusions may be scalable to larger incidents there is still a need to review the ‘surge capacity’ of any population-based screening programme. Watson et al. 11 advocated that a comprehensive, conceptual framework is needed to enhance the readiness, responsiveness, and effectiveness of health systems in dealing with unpredicted surges.
Conclusions
To our knowledge, this is the first study to use data from the 2018 PNE to describe the local impact on three screening services and assess how well they performed during and after the incident response. We found that all services were able to absorb the additional demand, although the smaller service, using two mobile vans, found this more challenging than services with predominantly static sites. Any reduction in routine activity must be adequately compensated for during the recovery period to ensure that round length is maintained for routinely invited women. Despite the media coverage, women affected are not more likely to attend than other women, but they may require more support, e.g. to change appointments and also because they are more likely to require further assessment tests and to have cancers. Screening programmes deliver services to a large target population and their ability to respond to an unexpected, large increase in activity in a timely fashion over a prolonged period will remain a significant challenge to many providers.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.