
Abstract
Objective
In the United States, colorectal cancer incidence has increased in adults under age 55. Although debate remains about whether this rise is a result of increased detection because of more colonoscopy utilization, population-based trends in colonoscopy among this age group are unknown. We examined changes in colonoscopy rates, as well as colorectal cancer incidence, among adults aged 40–54, using nationally representative data.
Methods
Recent (past year) colonoscopy rates were computed among 53,175 respondents aged 40–54 in National Health Interview Survey data from 2000 through 2015 by five-year age group. Colorectal cancer incidence rates and incidence rate ratios were estimated from 18 population-based Surveillance Epidemiology and End Result registries during the same period.
Results
Among respondents aged 40–44, past-year colonoscopy rates were stable during 2000–2015, and ranged from 2.3% to 3.5% (p-value for trend = 0.771). In contrast, colonoscopy rates increased from 2.5% in 2000 to 5.2% in 2015 among ages 45–49, and from 5.0% to 14.1% in ages 50–54 (test for trend p-values < 0.001). During 2000–2015, colorectal cancer incidence rates increased by 28% in people aged 40–44 (incidence rate ratio = 1.28, 95% CI 1.20, 2.37), 15% in those aged 45–49 (incidence rate ratio = 1.15, 95%CI 1.10, 1.21), and 17% in those aged 50–54 (incidence rate ratio = 1.17, 95%CI 1.13, 1.21), respectively.
Conclusion
Increases in colonoscopy rates were confined to ages 45–54, whereas colorectal cancer incidence rates rose in those aged 40–44, 45–49, and 50–54. Colonoscopy trends do not fully align with colorectal cancer incidence patterns.
Introduction
In the United States, colon cancer incidence has increased by 1.3% per year since the mid-1990's, and rectal cancer has increased by 2.3% since the early 1990's among people in their 40's. 1 These patterns contrast with those aged 55 and over, among whom colon and rectal incidence rates have been declining since the mid 1980s and mid 1970s, respectively, with accelerated declines in the early 2000s, in part due to increased colonoscopy utilization. 2 Several public health organizations have long standing recommendations to screen average-risk adults for colorectal cancer (CRC) with sigmoidoscopy (every five years), stool-testing (annually), and/or colonoscopy (every 10 years) beginning at age 50.3, 4 CRC screening prevalence escalated in the early-to-mid 2000s after Medicare, the health insurer of most individuals aged 65 and older, began covering colonoscopy for average risk beneficiaries in July, 2001. 5 Nationwide self-reported colonoscopy (in the past 10 years) rose from about 20% in 2000 to 47% in 2008, and further increased to 59% in 2015 among adults aged 50–75. 6 This trend may have spilled over to younger ages, including those under age 50, where routine screening is recommended among those with a family history of CRC or polyps (beginning at age 40) and black individuals (beginning at age 45). 7 Diagnostic colonoscopy may have also increased in this age group.
There remains debate about whether the rise in CRC incidence rates among younger adults reflects increased disease occurrence, or detection (i.e. lead-time bias) as a result of a more colonoscopies being performed over time. 8 Previous studies have reported modest temporal increases in ever undergoing endoscopy (sigmoidoscopy or colonoscopy) under age 50. 1 In an employer-based claims study, annual colonoscopy rates increased between 2001 and 2009, then declined slightly through 2014, among enrollees aged 40–49, 8 and colonoscopy rates increased between 1999 and 2010 among enrollees aged under 50 in integrated health systems. 9 Much less is known about nationally representative patterns in colonoscopy rates among those aged under 50 in the past year, which would more closely correspond to annual CRC incidence. We examined past-year colonoscopy, as well as other CRC tests, among a nationally representative sample of adults aged 40–54 by five-year age group during 2000–2015. CRC incidence during the corresponding period was also assessed using population-based cancer registry data.
Methods
The National Health Interview Survey (NHIS), a nationally representative, in-person household survey among non-institutionalized individuals was used to estimate the prevalence of CRC screening and risk factors, as well as sociodemographic characteristics, in the United States. Respondents aged 40–54 were selected from the 2000, 2003, 2005, 2008, 2010, 2013, and 2015 NHIS (n = 56,818); these surveys had respective response rates of 72.1%, 74.2%, 69.0, 62.6%, 60.8%, 61.2%, and 55.2%. 6
The primary outcome was self-reported colonoscopy in the past year for any reason, which was queried every 2–3 years among respondents aged 40 and older, beginning in the 2000 NHIS. Secondary outcomes included stool-based testing, sigmoidoscopy, or any CRC testing (stool, sigmoidoscopy, and/or colonoscopy) in the past year, to determine if there were changes in receipt of other tests. Stool-testing and sigmoidoscopy can detect polyps and CRCs, but follow-up with colonoscopy is required for polyp and/or tumor removal. Colonoscopy was, therefore, the main focus of the current study. 10 The self-reported reason for testing (routine, due to a problem, and other reason) was also examined among respondents with a recent colonoscopy. People who reported a previous CRC diagnosis (n = 126) or were missing CRC testing data (n = 3,517) were excluded, resulting in an analytic population of 53,175 adults (aged 40–44, n = 18,296; aged 45–49, n = 17,718; aged 50–54, n = 17,161).
The proportions of respondents with past-year CRC testing were stratified by five-year age group (40–44, 45–49, and 50–54). Cochran–Mantel–Haenszel tests for linearity were used to measure the significance of trends from 2000 to 2015. Absolute differences and rate ratios (RRs), which compare the relative change in past-year CRC screening rates between successive survey years (e.g. 2005 vs. 2003), and 95% Confidence Intervals (CIs) were calculated using logistic regression models with predicted marginal probabilities. 11 Changes in these sociodemographic characteristics (sex, race/ethnicity, and educational attainment), insurance, and CRC risk factors (smoking, alcohol, excess body weight, and family history of CRC) were examined over time. We also examined whether these factors were associated with recent colonoscopy using Chi-squared tests and adjusted rate ratios (aRR). Family history data were only available in the 2000, 2005, 2010, and 2015 surveys. Survey data analyses were conducted in SAS-callable SUDAAN, version 9.4, and NHIS survey weights were applied to ensure its representativeness and to account for sample selection, mitigating non-response bias.
Data on invasive CRC incidence in adults aged 40–54 during 2000–2015 were obtained from 18 population-based registries participating in the National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) program, covering 28% of the US population. 12 Annual delay-adjusted CRC incidence rates, as well as annual percent changes, were calculated for all stages combined, and by SEER Summary Stage (localized, regional, distant, and unstaged). Tests for parallel annual percentage changes (i.e. slopes) according to age group were also computed. Incidence rate ratios (IRR) comparing 2014–2015 versus 2000–2001 rates were computed according to age group and stage. Analyses of CRC incidence data were conducted with SEER*Stat and Joinpoint Software.13, 14
Results
Survey respondent characteristics
During 2000–2015, most survey respondents aged 40–54 were white (70.9%), privately insured (73.1%), overweight or obese (67.5%), never smokers (56.1%), and did not report a family history of CRC (94.1%) (Supplemental Table 1). The proportion of respondents who were Hispanic, college-educated, never smokers, and obese increased between 2000 and 2015.
Trends in CRC testing
Among respondents aged 40–44, 2.3–3.5% reported a recent colonoscopy between 2000 and 2015, with no significant linear trend during this time period (absolute difference = 0.1, p = 0.771) (Figure 1 and Table 1), and the only significant difference between successive survey years was a decline between 2010 and 2013 (Table 2). Among respondents aged 45–49, unadjusted past-year colonoscopy rates increased from 2.5% in 2000 to 5.2% in 2015, with an absolute difference of 2.7% (test for trend p-value <0.001) and RR of 2.06 (95% CI 1.47, 2.91) (Table 1). When successive survey years were compared in this age group, colonoscopy rates significantly increased between 2005 and 2008 and declined between 2008 and 2010, but were otherwise stable (Table 2). In respondents aged 50–54, colonoscopy rates increased from 5.0% in 2000 to 14.1% in 2015, an absolute difference of 9.1% (test for trend p-value < 0.001) and a relative increase of 2.82 (95% CI 2.11, 3.59). When successive survey years were compared, rates increased between 2000 and 2003 and between 2005 and 2008, but were otherwise stable in ages 50–54 (Table 2). Stool testing in past year significantly declined between 2000 and 2015 in all age groups, with absolute differences of 2.9%, 4.4%, and 6.9% in respondents aged 40–44, 45–49, and 50–54, respectively (p <0.001) (Table 1). Recent sigmoidoscopy was uncommon (<3%) and appeared to decline, though estimates were unstable for several survey years (Supplemental Table 2). In respondents aged 40–44, the non-significant rise in colonoscopy rates coupled with declines in stool-testing lead to a 3% absolute reduction, or 45% relative reduction (RR = 0.55, 95% CI 0.41, 0.75) in any CRC testing during the 15-year study period. Past-year CRC testing significantly declined in respondents aged 45–49 (absolute difference=-2.1, p < 0.001; RR = 0.78, 95%CI 0.62, 0.99) and were stable in respondents aged 50–54 (Table 1).
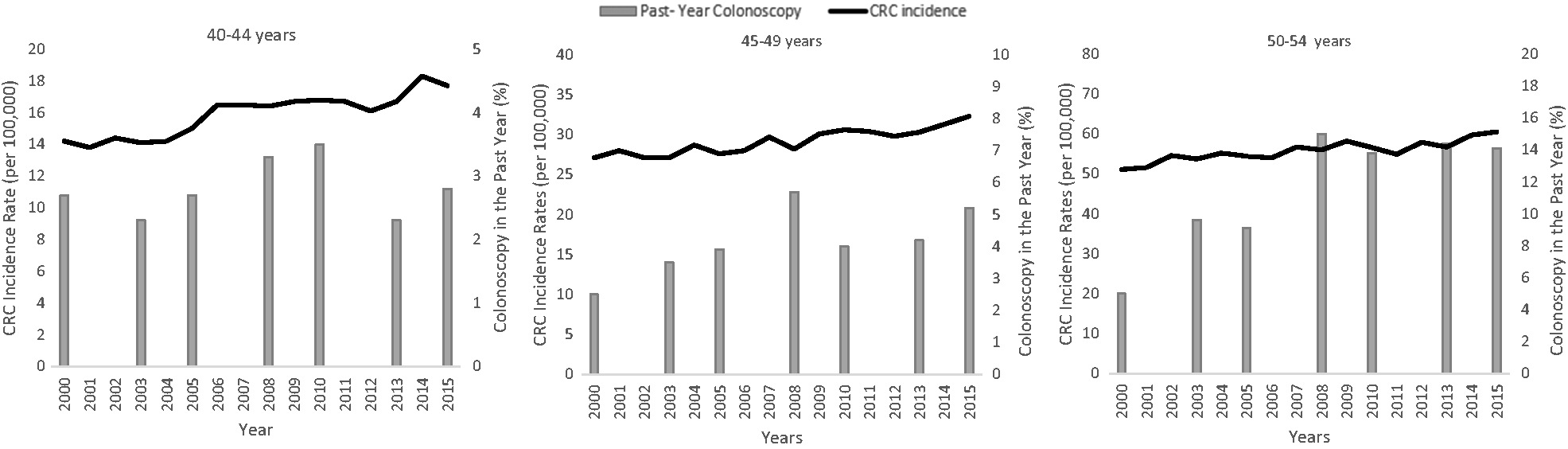
Colorectal cancer incidence and use of colonoscopy in the past year among adults 40–54 years of age, 2000–2015a. CRC: Colorectal Cancer. a. Colorectal Cancer Incidence data are from SEER-18 population-based registries, Colonoscopy data are from National Health Interview Surveys. CRC incidence rates are delay-adjusted. Annual Percent Change (APC) in CRC Incidence Age 40–44 years APC = 1.7, p-value <0.001; 45–49 years APC = 1.1 p-value<0.001; 50–54 years APC = 0.9 p-value<0.001
Unadjusted rates of colonoscopy, stool testing, and any colorectal cancer test in the past year according to survey year and age, NHIS 2000–2015.
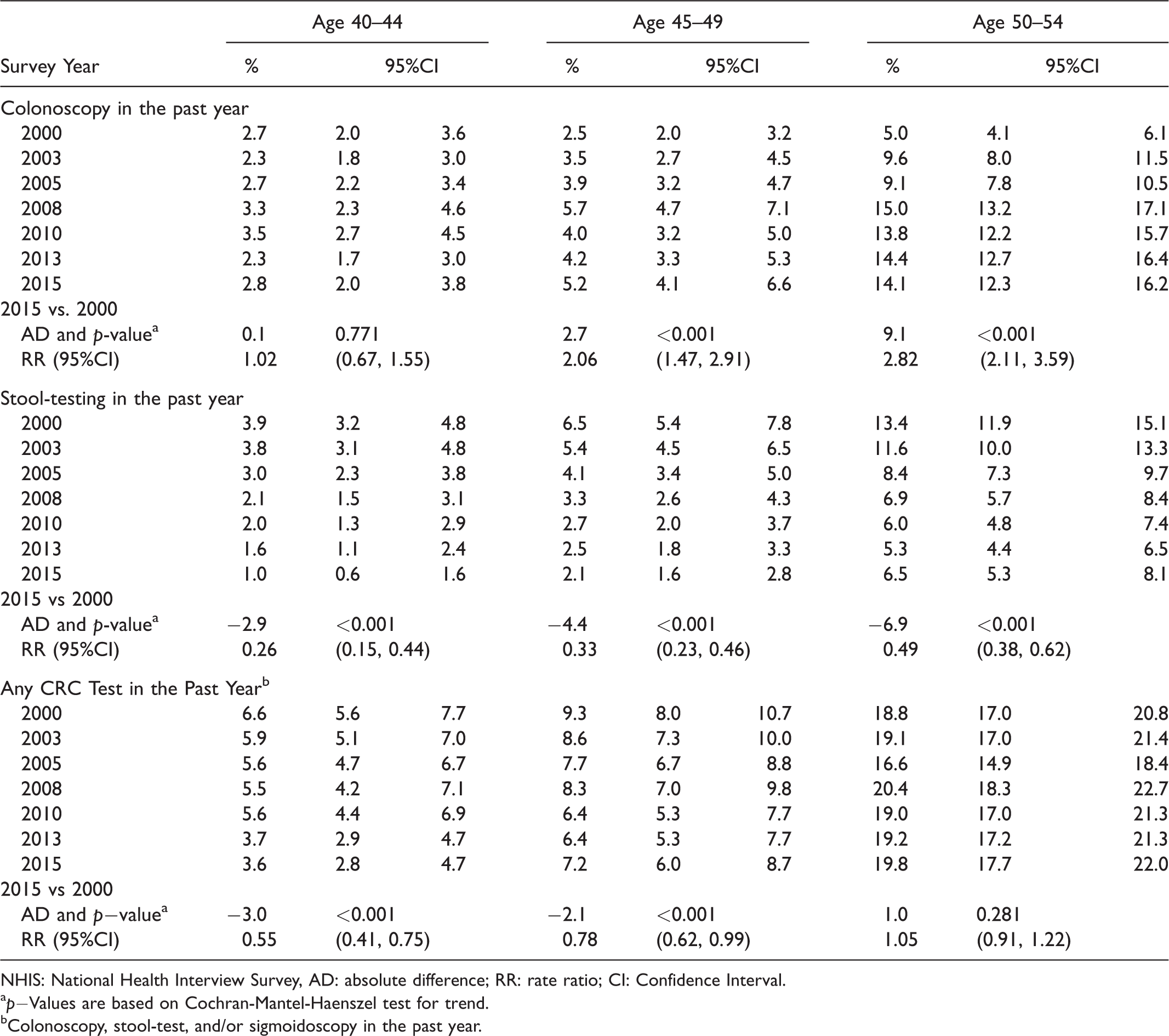
NHIS: National Health Interview Survey, AD: absolute difference; RR: rate ratio; CI: Confidence Interval.
ap−Values are based on Cochran-Mantel-Haenszel test for trend.
bColonoscopy, stool-test, and/or sigmoidoscopy in the past year.
Absolute and relative change in unadjusted colonoscopy rate in the past year over time by age, NHIS 2000–2015.
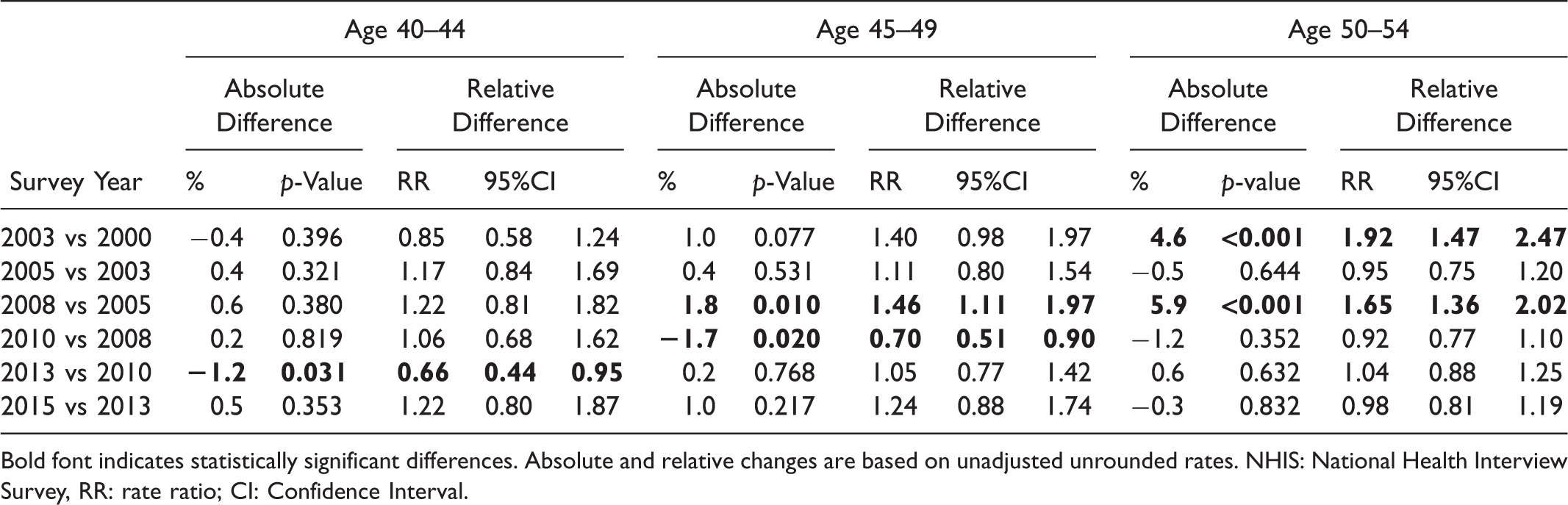
Bold font indicates statistically significant differences. Absolute and relative changes are based on unadjusted unrounded rates. NHIS: National Health Interview Survey, RR: rate ratio; CI: Confidence Interval.
Characteristics of those undergoing colonoscopy
Most respondents reporting a recent colonoscopy were white, obese or overweight, never smokers, had private insurance, and did not have a family history of CRC (Table 3). In adjusted analyses (Supplemental Table 3), people in their 40s who had a family history of CRC were three to four times as likely as those without a family history to have had a past-year colonoscopy (age 40–44: aRR = 3.90, 95% CI 2.63–5.78; age 45–49: aRR = 3.17, 95% CI 2.18–4.62), but represented only about 17% of those recently screened. Black respondents were more likely to report a recent colonoscopy compared with whites for ages 45–49 (aRR = 1.30, 95% CI 1.01–1.68). Hispanics had lower colonoscopy rates than whites (aRR = 0.62, 95% CI 0.43, 0.91) among those aged 40–44. Among respondents aged 50–54, colonoscopy rates were significantly lower in those with less than a college degree than college graduates, and higher among obese compared with normal weight respondents, and among current and former drinkers relative to lifetime abstainers. The uninsured had consistently lower colonoscopy rates compared with privately insured in all three age groups. Among respondents with a recent colonoscopy, self-reported reasons for testing is shown in Supplemental Figure 1. Less than half of respondents aged 40–44 (34.4%) and 45–49 (44.2%) indicated that their colonoscopy was part of a routine exam, compared with over three-quarters (76.4%) of respondents aged 50–54. Trends in reason for testing between 2000 and 2015 were not presented, due to unstable estimates.
Characteristics of respondents who underwent colonoscopy in the past-year, NHIS 2000–2015.
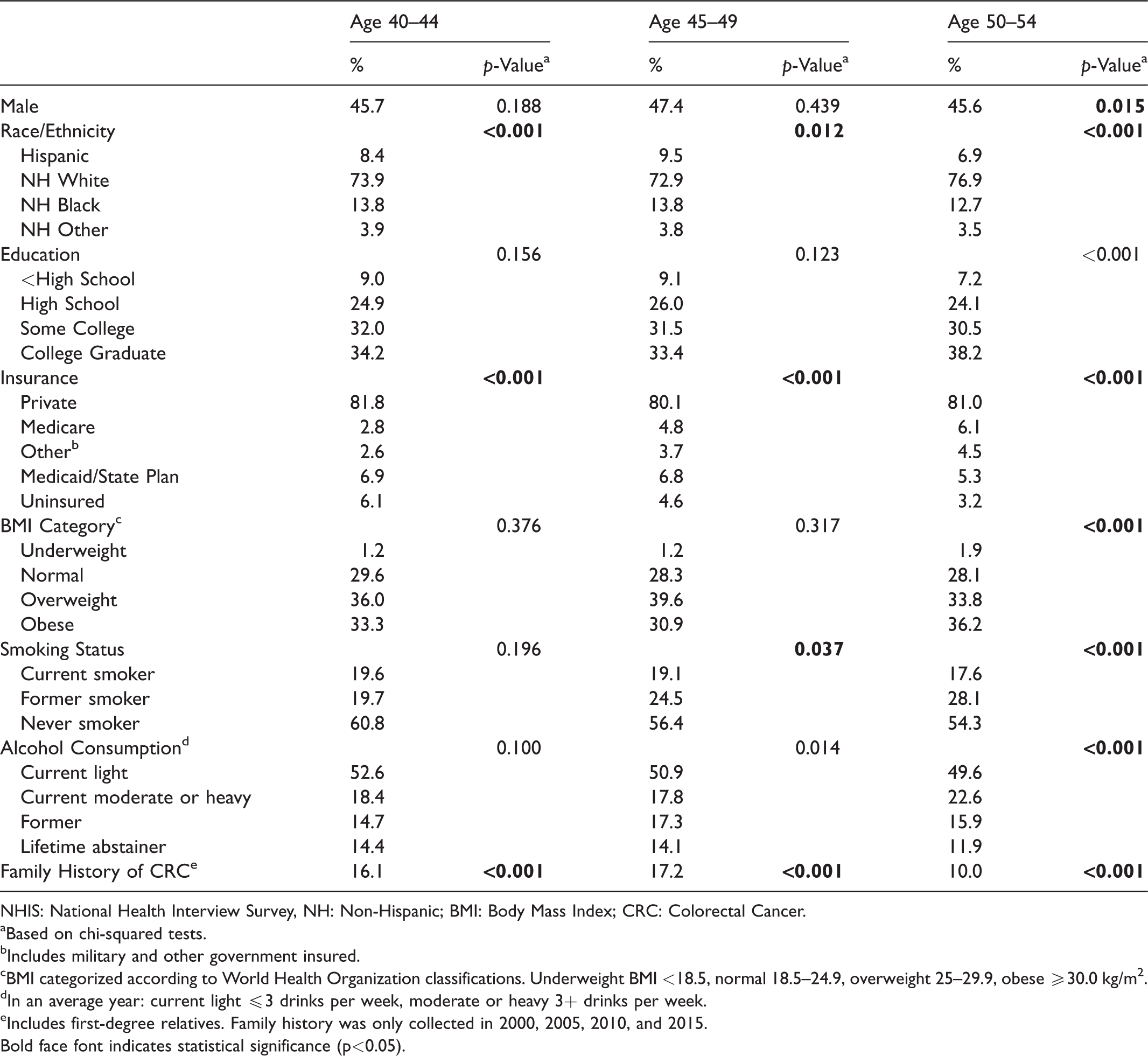
NHIS: National Health Interview Survey, NH: Non-Hispanic; BMI: Body Mass Index; CRC: Colorectal Cancer.
aBased on chi-squared tests.
bIncludes military and other government insured.
cBMI categorized according to World Health Organization classifications. Underweight BMI <18.5, normal 18.5–24.9, overweight 25–29.9, obese ≥30.0 kg/m2.
dIn an average year: current light ≤3 drinks per week, moderate or heavy 3+ drinks per week.
eIncludes first-degree relatives. Family history was only collected in 2000, 2005, 2010, and 2015.Bold face font indicates statistical significance (p<0.05).
CRC incidence trends
CRC incidence rates according to each age group are shown in Supplemental Table 4 and overlaid with past-year colonoscopy statistics in Figure 1. Between 2000 and 2015, the annual percent change in incidence rates significantly increased in each group, by 1.7%, 1.1%, and 0.9% in ages 40–44, 45–49, and 50–54, respectively, with the greatest increases occurring in the group aged 40–44 (p-value for parallel slope = 0.018 for age 40–44 vs. 45–49 and 0.002 for age 40–44 vs. 50–54). The 2014–2015 CRC incidence rate (IR) was 28% higher in adults aged 40–44 (IRR = 1.28, 95% CI 1.20, 1.37), 15% higher in those aged 45–49 (IRR = 1.15, 95% CI 1.10, 1.21), and 17% higher in ages 50–54 (IRR = 1.17, 95% CI 1.13, 1.21) relative to the corresponding incidence in 2000–2001 (Supplemental Table 5). Statistically significant annual percentage changes and IRRs in the incidence rates between 2000 and 2015 for localized disease were confined to ages 50–54, and for regional disease were only observed in those aged 40–44 and 45–49. The annual percentage change for distant staged disease increased for each age group, by 2.9%, 2.3%, and 1.0% in people aged 40–44, 45–49, and 50–54, respectively (Figure 2 and Supplemental Table 5). The 2014–2015 distant staged CRC incidence rates were 46% (IRR = 1.46, 95% CI 1.28, 1.66) higher in ages 40–44, 40% greater in ages 45–49 (IRR = 1.40, 95% CI 1.27, 1.55) and 19% greater in ages 50–54 (IRR = 1.19, 95% CI 1.10, 1.30) compared with the corresponding rates in 2000–2001. Trends in unstaged CRC incidence rates were stable during 2000–2015 (Supplemental Table 5).
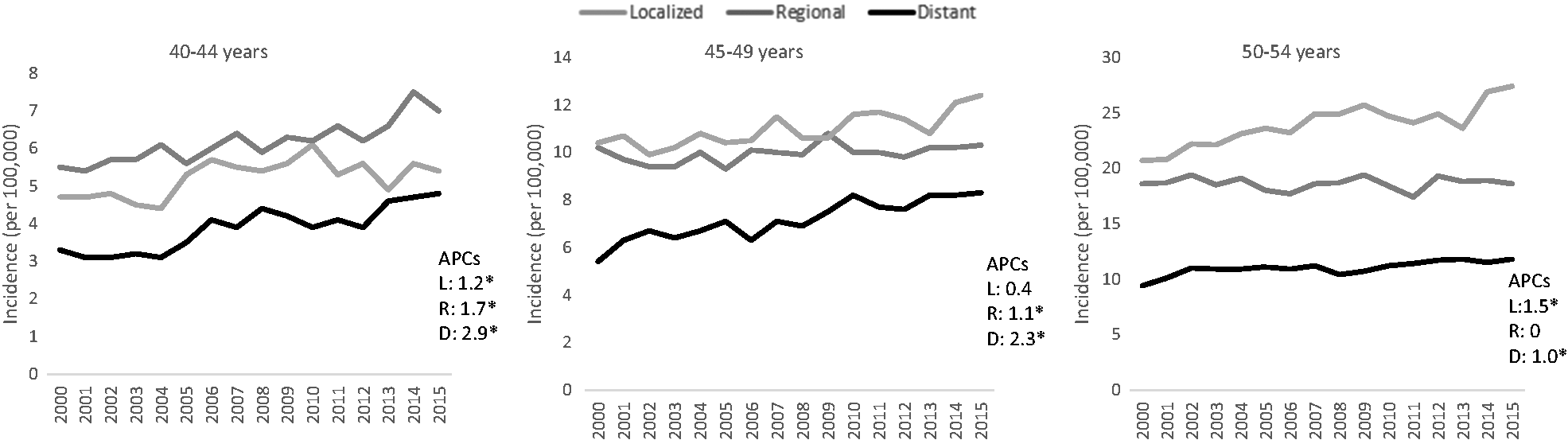
Colorectal cancer incidence by stage among adults 40–54 years of age, 2000–2015.a
Discussion
In this nationally representative study of individuals aged 40–54, the rates of self-reported past-year colonoscopy were stable in adults aged 40–44 during 2000–2015, and more than doubled in those aged 45–54. Between 2000 and 2015, CRC incidence rates increased in all age groups, by 28% in people aged 40–44, 15% in people aged 45–49, and 17% in ages 50–54, respectively.
Trends in past-year colonoscopy do not appear to fully align with CRC incidence trends among ages 40–54 during 2000–2015. Past-year colonoscopy rates increased between 2005 and 2008 among those aged 45–54, which was concordant with a rise in CRC incidence during this period. However, discordant patterns were also observed. For example, during the 15-year study period, colonoscopy rates were stable among those aged 40–44, but this group experienced the largest relative increase in CRC incidence (annual percentage changes and IRR) of all three age groups. In addition, despite decreases in colonoscopy rates among those aged 45–49 during the economic recession between 2008 and 2010, as has been observed in other populations, 15 CRC incidence did not decrease during this time frame.
It has been suggested that increases in CRC incidence in those aged under 55 may represent lead-time bias, whereby tumors are detected earlier with testing, primarily with colonoscopy. 8 While our study did not directly link CRC incidence with screening history, our analyses, and previous studies of stage-specific CRC incidence, provide some information on this hypothesis.1,16, 17 If the growing CRC incidence trend in those aged 40–54 had been the result of CRC testing, primarily with colonoscopy, reductions in late-stage CRC incidence and mortality would be expected. However, distant stage CRC incidence rates increased between 2000 and 2015 for each age group, and nationwide data during 1998–2009 indicate that the most rapid increase among people aged under 50 was for distant stage disease. 17 Further, a previous study showed CRC mortality began rising in 2005 among people aged 40–54. 16 There was a significant increase in localized stage among screening aged individuals aged 50–54 in our study, which could represent tumors being detected earlier with screening in this age group.
Our finding of increasing colonoscopy use among people in their mid-to-late 40s is largely consistent with a study of employer-based claims, in which colonoscopy rates increased between 2001 and 2009 then declined slightly through 2014 among enrollees aged 40–49, 8 and a study of integrated health systems where colonoscopy increased between 1999 and 2010 among enrollees aged under 50. 9 A previous study of NHIS data reported an increase in CRC screening among those in their 40s with a family history between 2005 and 2010. 18 We also observed a decline in stool-testing, which is consistent with trends in other age groups. 19
Adults in their 40s with a self-reported family history of CRC were more likely to be screened than those without, consistent with long-standing recommendations for earlier screening in high-risk groups. 20 We also observed that black respondents aged 45–49 were more likely to undergo colonoscopy than whites, in accordance with the American College of Gastroenterology recommendation for screening beginning at age 45. 7 Interestingly, disparities in colonoscopy rates according to educational attainment were only observed in those aged 50–54. In 2018, the American Cancer Society lowered the recommended age to begin CRC screening for average-risk adults from 50 to 45 years.1,21, 22 Whether or not socioeconomic disparities in undergoing colonoscopy among people aged 45–49 will emerge with the newly issued American Cancer Society guideline to begin screening at age 45 is unknown. Other CRC risk factors (e.g. smoking, excess body weight) were not related to screening among adults in their 40s.
Limitations of this study include self-reported data on colonoscopy and family history of CRC, which are subject to recall bias, although the sensitivities of self-reported endoscopy (0.90) 23 and CRC family history (0.87) are relatively high. 24 In addition, declining response rates may introduce selection bias, though NHIS data were weighted to mitigate this bias. Our study also uses ecological data, therefore causality cannot be established. Despite these limitations, this study provides the first nationwide estimates of past-year colonoscopy in adults aged 40–54 and corresponding population-based CRC incidence data.
Conclusion
Past-year colonoscopy rates during 2000–2015 were stable among people aged 40–44 and increased among those aged 45–54, which does not fully align with the rise in overall and distant stage CRC incidence rates in all three age groups during the corresponding period. Future studies should examine reasons for the rising CRC incidence rates in young adults, and monitor colonoscopy rates among adults aged 45–49 to assess the impact of recent American Cancer Society guidelines lowering the age of recommended screening.
Supplemental Material
Supplemental material for Are temporal trends in colonoscopy among young adults concordant with colorectal cancer incidence?
Supplemental Material for Are temporal trends in colonoscopy among young adults concordant with colorectal cancer incidence? by Stacey A Fedewa, Rebecca L Siegel and Ahmedin Jemal in Journal of Medical Screening
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The American Cancer Society funded the analysis, interpretation, and presentation of the manuscript. Stacey Fedewa, Rebecca Siegel, and Ahmedin Jemal, are employed by the American Cancer Society, which received a grant from Merck, Inc. for intramural research, however, their salary is solely funded through American Cancer Society funds.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.