
Abstract
Objectives
If prostate cancer screening practices relate to occupation, this would have important implications when studying the aetiological role of workplace exposures on prostate cancer. We identified variations in screening by occupation among men in Montreal, Canada (2005–2012).
Methods
Prostate specific antigen testing and digital rectal examination (ever-screened and frequency of screening, previous five years) were examined among population controls from the Prostate Cancer & Environment Study. Face-to-face interviews elicited lifestyle and occupational histories. Multivariable logistic regression was used to estimate the odds of ever-screening for the longest-held occupation, adjusting for potential confounders. Negative binomial models were used to examine relationships with screening frequency.
Results
Among 1989 controls, 81% reported ever having had a prostate specific antigen test, and 77% a digital rectal examination. Approximately 40% of men reported having a prostate specific antigen test once a year, on average. Compared with those in management or administrative jobs, men in primary industry (odds ratio 0.26, 95% confidence interval 0.10–0.65), construction (0.44, 0.25–0.79), machining (0.45, 0.21–0.97), and teaching (0.37, 0.20–0.70) were less likely to have undergone prostate specific antigen screening. Results were similar when considering the most recent job.
Conclusions
Our findings highlight substantial variations in prostate cancer screening by occupation. Men in occupations where carcinogen exposures are more common are less likely to participate in prostate screening activities. This could be an important source of bias, and occupational studies of prostate cancer should account for screening practices.
Introduction
Occupational epidemiological studies play a critical role in identifying cancer causes, partly because of the higher levels of exposure to carcinogens that occur in workplaces, facilitating their assessment. 1 Many ‘classic’ human carcinogens (e.g. exposures such as arsenic, mustard gas, chromium, and vinyl chloride) were first identified through occupational studies. 2 A compelling instance of occupational epidemiology providing key insights on human cancer risks is that of radon exposure among uranium miners. The risk models developed via those studies are the basis for our understanding of the vast public health impact of radon exposure on lung cancer. 3 Similarly, the realization that asbestos causes lung and other cancers was made possible through epidemiological investigations of asbestos factory workers in the 20th century. 4 The methods established for explaining higher cancer risk among workers have been used to identify new and emerging carcinogens, and have improved our understanding of the aetiology of many cancer sites.
It has long been suspected that most prostate cancers have environmental and occupational origins. 5 Several studies have documented elevated risks in occupational groups such as firefighters, farmers, white collar, and military workers.6–10 Additionally, specific occupational agents have been identified, including toxic metals, polychlorinated biphenyls, and polycyclic aromatic hydrocarbons, that may increase prostate cancer risk. 11 Methodological issues have hampered progress in understanding the potential occupational causes of prostate cancer, including the inability to account for the role of screening in observed associations.
For cancer sites that have screening tests available to detect cancer or pre-clinical abnormalities at earlier stages, where treatment could be more effective, some complications can arise for occupational investigations of cancer causes. If screening is related both to the likelihood of a cancer diagnosis and an occupational exposure of interest, then the results of the study are subject to screening bias. 12 In population-based studies, occupational exposures are often first studied using information on job title, which is also a marker of a wide variety of other sociodemographic factors that may influence screening behaviours.
Studies of prostate cancer are at particular risk of screening bias because a large portion of these cancers can remain asymptomatic for long periods of time. Prostate cancer is the most diagnosed cancer among Canadian men (after non-melanoma skin cancer), and the third leading cause of cancer death. 13 Screening guidelines for prostate cancer have evolved considerably over the past 25 years. Prostate specific antigen (PSA) testing was introduced in Canada in 1993, with further emphasis on the importance of screening in 2001, when news spread that Allan Rock, then Canada’s Minister of Health, was diagnosed with early prostate cancer as a result of serial PSA testing. 14 This, combined with the fact that the province of Quebec has free, universal access to healthcare, including PSA testing, contributed to high screening rates in the years that followed. A decline in screening ensued following changes in provincial recommendations. 15 In response to over-diagnoses, the U.S. Preventive Services Task Force released recommendations in 2008 advising against PSA screening in men over age 75, and in 2011 advising against PSA screening for asymptomatic men of all ages. In 2014, the Canadian Task Force on Preventive Health Care followed with recommendations against PSA screening for healthy men of any age. Despite these recommendations, PSA screening remains common in Canada. About half of men aged 35 and over reported having had a PSA test in 2012. 16 Digital rectal exam (DRE) has also been commonly used in Canada for prostate cancer screening, alone or in combination with PSA testing, despite its limited sensitivity and specificity. 17
The lack of information on prostate cancer screening practices in many large epidemiological studies, and how these practices differ by occupation, may have complicated our understanding of the relationship between exposure and disease.18,19 For example, in a study of Finnish ferrochromium workers, the authors attributed an increased prostate cancer risk to increased PSA testing, but this was speculative, as they did not have information on screening. 20 The inconsistencies in the aetiological occupational literature on prostate cancer could be partly due to confounding, if the likelihood of having a PSA test is associated with an exposure of interest, which is generally linked to job title. 21
The aetiology of prostate cancer remains largely unknown, and overlooking screening patterns can compromise the interpretation of studies aimed at identifying modifiable risk factors.12,22,23 Past work has shown that the decision to undergo prostate cancer screening is influenced by age, ethnicity, and family history. 24 Geographic location, perceived health status, being married, and regular access to a family physician are also important factors that determine screening practices. 25 Higher income and education are consistently linked with a higher propensity to seek out PSA screening tests.26–28 Lower social deprivation has also been associated with greater uptake of breast, cervical, and bowel screening among women. 29 Decisions around whether to undergo screening are also likely to be related to each other, and these characteristics may not be distributed evenly across different social strata or occupational groups. We know of no study that has investigated how screening practices relate to occupation specifically.
This study aimed to evaluate the role of occupational characteristics on screening for prostate cancer. This will help to fill the gap in our understanding of how screening practices may have influenced the interpretation of previous findings in prostate cancer studies.
Methods
The Prostate Cancer & Environment Study (PROtEuS) was a case–control study conducted in Montreal, Canada in 2005–2012. Details of this study have been provided elsewhere.30–33 Incident cases of prostate cancer in men aged 40–75 were ascertained across seven French-language hospitals in Montreal. Concurrently, a population control series was constituted by randomly sampling French speaking men residing in Montreal from the provincial permanent electoral list, and frequency matching them to cases by age (±5 years). Eligible controls had no history of prostate cancer. Current analyses were restricted to controls from PROtEuS, as nearly all cases had undergone screening. In all, 2036 controls were recruited (response rate 56%). Reasons for non-participation were refusal (86%), unable to trace (11%), death with no proxy respondent available (1%), language barrier (1%), and too sick to participate (1%). Comparisons of participants and non-participants based on census-derived variables (family income, education level, per cent of recent immigrants, and per cent of unemployment) indicated minimal differences between the two groups, alleviating concerns about selection bias and lack of representativeness of the base population.
Data on sociodemographic and lifestyle factors, and screening behaviours, were collected retrospectively via in-person interviews by trained personnel. Information was elicited for each job held for at least one year, including task descriptions, dates, and industry. Participants were asked first if they had ever had a medical examination or a test to detect if they had prostate cancer, and second whether or not they had ever had a ‘blood test to detect prostate cancer (PSA)?’, as well as if they were ever-screened by DRE. Frequency of PSA and DRE tests in the previous five years was also reported. Questions about the two testing approaches were asked separately, precluding differentiating whether they were performed alone or in combination.
Due to our primary interest in occupational factors, we examined bivariate relationships between screening variables and occupation, defined by 17 groups. These groups were based on the first two digits of the 1971 (updated to 1980) Canadian Classification Dictionary of Occupations (CCDO) code assigned by industrial hygienists from the workers’ task descriptions.34,35 Additionally, we examined a more detailed job classification, also based on the CCDO codes, that was developed by a study hygienist to represent better the types of tasks that workers might perform, and to group CCDO codes accordingly. This classification included 94 different codes.
Potential confounders for screening considered for inclusion in the models included: family history of prostate cancer, regular alcohol drinking, regular smoking, marital status (married/single/widowed), ancestry (European, Black, Asian, other/don’t know), attained education (<high school, high school graduation, some college, some university or more), household income (categories), physical activity at work and leisure (not very, moderately, very active), age, and body mass index (normal, overweight, obese). Bivariate relationships between these sociodemographic and lifestyle factors and ever-screened for prostate cancer were tested for differences using the chi-square statistic for categorical variable comparisons, t-tests for differences in means by categories, and non-parametric statistical tests where assumptions of normality of the data were not met.
We used unconditional logistic regression to model the odds of having ever been screened for prostate cancer (examined separately by type of screening test, PSA or DRE, as well as by either test) by occupational group (for the longest-held job). We considered the covariates listed above in these models using backwards stepwise regression and retained in the final model those covariates with a p-value of less than 0.2. We used negative binomial regression to examine the frequency of PSA testing in the five years before interview (as we could not assess frequency of DRE and PSA used together). Count data are often modelled with Poisson regression, but as these data were overdispersed, an alternative with similar interpretation is the negative binomial model. 36 The same potential confounders were considered in this model as for the logistic model for ever-screened by PSA. The most recent job, rather than the longest job held, was also examined in relation to prostate cancer screening. DRE was also considered, as was ever-screening by either test.
Results
Overall, 1969 controls (97%) with complete data on demographic, lifestyle, screening, and occupational information were included: 81% of men had ever been screened using PSA and 77% with DRE (71% had been screened using both, and 90% with at least one type of test). Mean age was 64.8 years (standard deviation 6.9). Approximately 40% of men reported having a PSA once a year, on average, which was the most commonly reported screening frequency. The DRE was also most often reported once per year, on average (522 men, or 22%). A substantial proportion of men could not remember the frequency of PSA (22%) or DRE (24%) tests they had had. Few reported screening more than once per year, on average (3 and 6% for DRE and PSA, respectively), which could have reflected repeated tests following initially elevated results.
Table 1 shows the distribution of characteristics for the study population, as well as the bivariate relationships between ever-screening for prostate cancer by PSA and the various occupational, lifestyle, and demographic variables available. While the majority of men had undergone PSA screening (1604 of 1969), the proportions differed by main job title. About 58% of workers in primary industry (farming/forestry/fishing/mining) had undertaken a PSA test, ranging up to over 90% of those men in management jobs.
Frequency distribution of characteristics based on prostate specific antigen (PSA) screening behaviours.

ap-value is for the comparison between the screened and unscreened men.
bDefinition of job groups: Art, literature, sport: CCDO codes 33, 37; Clerical: CCDO code 41; Construction: CCDO code 87; Farming, forestry, fishing, mining: CCDO codes 71, 73, 75, 77; Machining: CCDO code 83; Management, administration: CCDO code 11; Material handling: CCDO codes 93, 95; Medicine, health: CCDO code 31; Natural sciences, engineering: CCDO code 21; Processing: CCDO codes 81, 82; Product fabrication, repair: CCDO code 85; Sales: CCDO code 51; Service: CCDO code 61, EXCEPT Firefighting and police work, which were separated out as their own category; Social sciences and religion: CCDO codes 23, 25; Teaching: CCDO code 27; Transport equipment operators: CCDO code 91.
cRegular smoker: reported smoking at least 100 cigarettes in their life, in addition to smoking at least one cigarette per week for at least one year.
dRegular drinker: reported ever drinking alcohol at least once per month for at least one year.
Results of the final logistic regression model for ever-PSA screening are presented in Table 2 for the 17 broad occupation types. The overall R2 value for this model was 0.104, which shows that the model explained approximately 10% of the variance. Compared with men holding management occupations, those involved in teaching (Odds Ratio [OR] 0.37, 95%Confidence Interval [CI] 0.20–0.70), primary industry (farming, forestry, fishing, mining) (OR 0.26, 95%CI 0.10–0.65), construction (OR 0.44, 95%CI 0.25–0.79), and machining (OR 0.45, 95%CI 0.21–0.97) had lower odds of screening after considering potential confounders. Results for similar models with ever-screened by DRE or either test are shown in Supplemental Tables 1 and 2, respectively. No substantive differences in findings between these screening tests were found.
Adjusted a odds of having ever been screened by prostate specific antigen (PSA) test according to the longest job held.
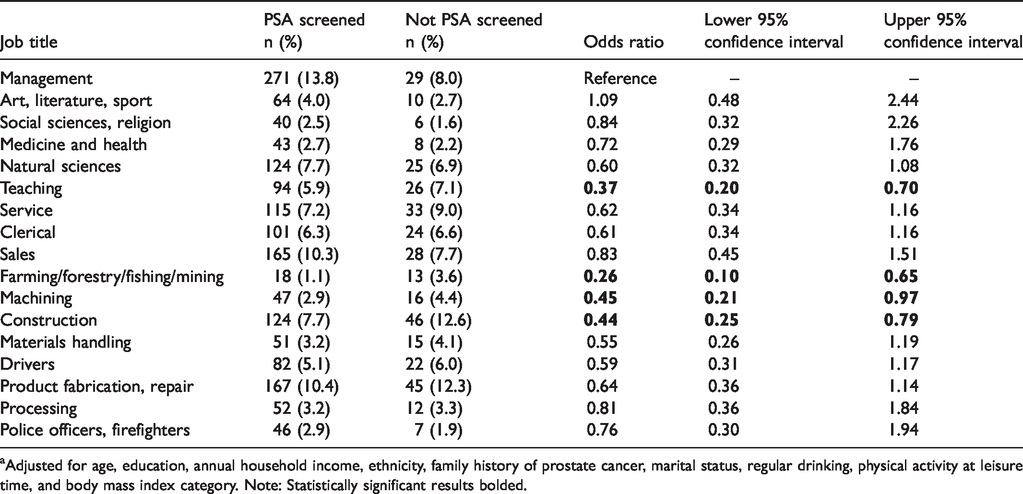
aAdjusted for age, education, annual household income, ethnicity, family history of prostate cancer, marital status, regular drinking, physical activity at leisure time, and body mass index category. Note: Statistically significant results bolded.
Results using the most detailed task-based job classification are shown in Table 3. Data are presented where at least 10 PSA-screened men were present in each category. This reduced the number of job classifications in this scheme from 94 down to 31. Due to the lower number of subjects in each job category, this model was adjusted for a minimal set of potential confounders: the first model adjusted for age only, and the second for age, income, and educational attainment. Based on the second model, several occupational groups were less likely to have been screened than administrators and managers. These included construction workers, electrical power workers, farmers, janitors, physical scientists, sheet metal workers, and teachers. The overall R2 value for the fully adjusted model was 0.079, which shows that the model explained approximately 8% of the variance.
Adjusted odds of having ever been screened by prostate specific antigen (PSA) test according to the longest job held, by detailed job classification. a
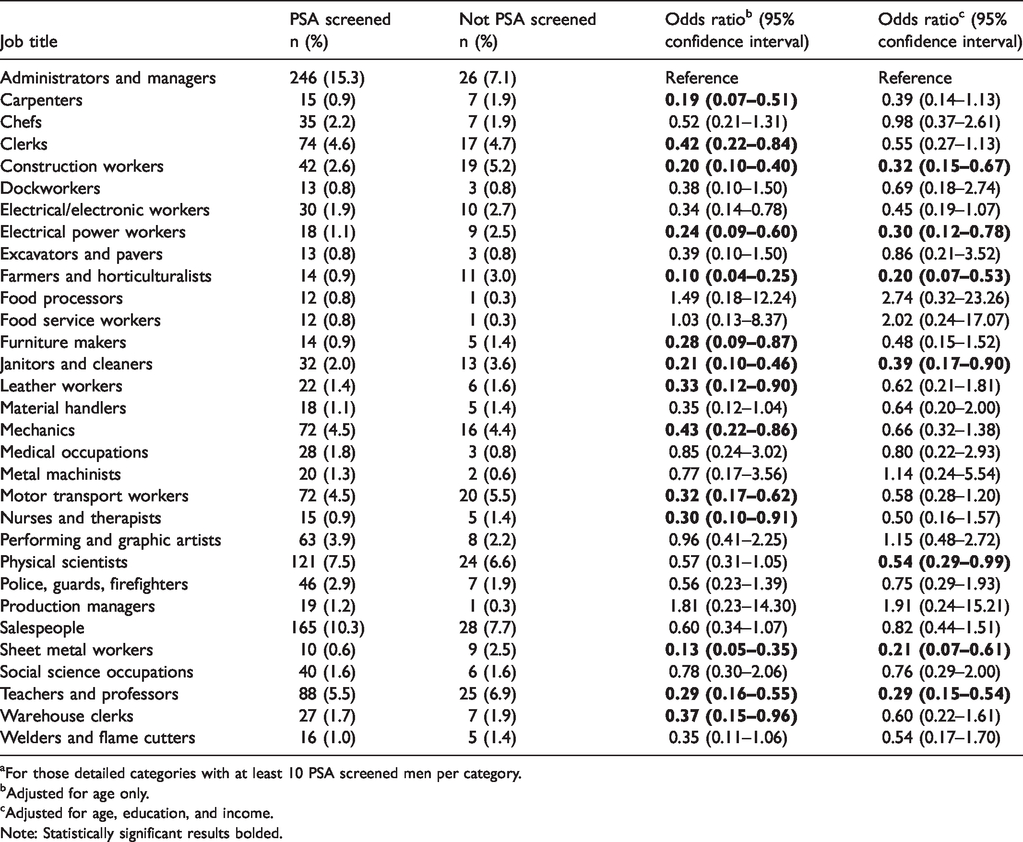
aFor those detailed categories with at least 10 PSA screened men per category.
bAdjusted for age only.
cAdjusted for age, education, and income.
Note: Statistically significant results bolded.
The results for frequency of PSA screening in the five years before interview are presented in Table 4. Those working in the social sciences and religion had a lower rate of PSA screening in the previous five years than those in management, and those in clerical and sales jobs had a higher screening rate than managers. There were no other meaningful differences between job categories in terms of frequency of PSA screening. Associations with the most recent job, rather than longest one, were also examined with similar findings (Supplemental Table 3).
Adjusted a rate ratios for the frequency of prostate specific antigen (PSA) screening test in the five years before interview according to the longest job held.
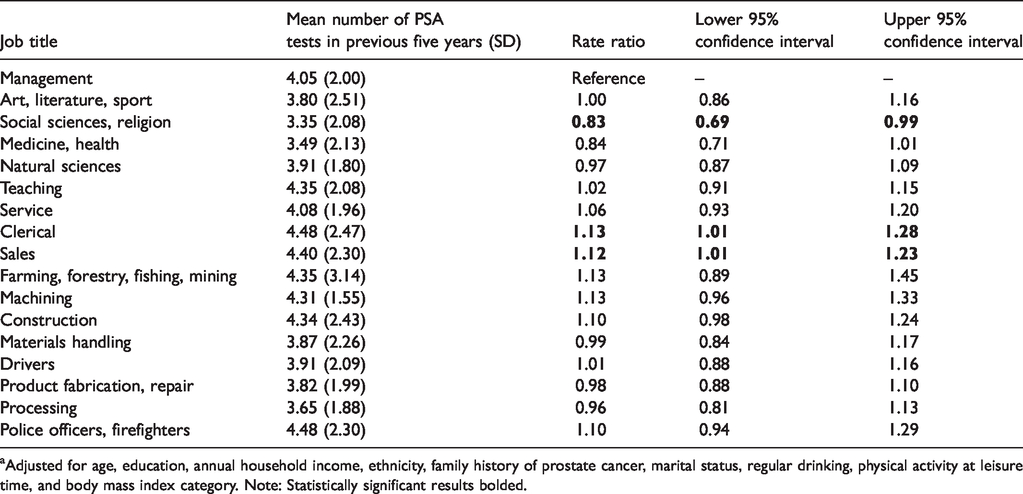
aAdjusted for age, education, annual household income, ethnicity, family history of prostate cancer, marital status, regular drinking, physical activity at leisure time, and body mass index category. Note: Statistically significant results bolded.
Discussion
We examined the relationship between occupation and prostate cancer screening among population controls in a large Canadian population-based case–control study, while controlling for personal and lifestyle factors. As PSA testing plays an important role in prostate cancer diagnosis, the associations between risk factors and prostate cancer in observational studies could be affected by detection bias. 21 This work provides the first evidence that screening behaviours can vary according to occupational groups. It has been recognized that failure to account for screening in aetiological studies has hampered progress on our understanding of prostate cancer development. 12
Our main aim was to evaluate whether occupation is associated with the likelihood of prostate cancer screening. Overall, our analyses suggest that there are differences in screening by job type that are not solely attributable to socioeconomic status. We found that men in primary industry, construction, and machining, and to a lesser extent teaching, were less likely to have ever been screened than those in management. When we examined finer job classifications, we could see that general construction workers, electrical workers, farmers, janitors, sheet metal workers, and teachers were driving these relationships. This has important implications for the interpretation of previous studies of prostate cancer, as well as for future investigations that seek to identify occupational prostate carcinogens. Men working in primary industry and manufacturing are at higher risk of exposure to occupational carcinogens, and their lower screening rate compared with men who should be at lower risk of carcinogen exposures, such as managers, could be a source of bias in prostate cancer studies. This would tend to lead to an underestimate of risk and a compromised ability to detect the influence of a workplace carcinogenic exposure.
In some cases, there were very strong inverse associations between occupation and screening. We wanted to assess how much age was influencing the results, as age is correlated with job type (moving into management as men age, for example). We performed an age-stratified analysis (results included in Supplemental Table 4), and found that the patterns by job type and magnitude of the odds ratios remained similar across all age strata, although some estimates became unstable due to small numbers.
The relationship between job and PSA test frequency in the previous five years is interesting, as we expected that the same workers identified as less likely to have ever been screened might also be screened less frequently for prostate cancer than the more traditional office workers. This was not the case. Those in social science and religious occupations had a lower screening odds ratio than managers, while clerical and sales workers had elevated odds ratios compared with those in management. In examining this finding in more detail, we noted that a greater proportion of those men with office and management jobs underwent screening once a year, on average (i.e. they reported five screening instances in the previous five years). The province of Quebec has universal and free access to healthcare, and yearly medical examinations are common. 37 We had information on the frequency of physician visits five years before the study, but there were no significant differences by job class in this variable, and including it in the model did not make a difference to the effect estimates (Supplemental Table 5). While there was no official prostate cancer screening programme in place, it appears that at the time the study was conducted (2005–2012) prostate cancer screening was often part of routine yearly medical exams. Being free of charge to all men, there is a lesser concern in this study than in some other populations that prostate cancer screening practices would reflect financial situation.
The main strengths of this study are its relatively large sample size, and detailed data including, for the first time, occupational variables that were collected allowing consideration of several predictors of prostate cancer screening behaviours. Several sensitivity analyses were undertaken to examine different definitions of occupational groups, and similar results were found. These results suggest that occupation is related to prostate cancer screening, and screening is likely to be of importance in studies examining the occupational causes of cancer. Job title was a stronger correlate of screening than many other factors, including income, ethnicity, and marital status. Failure to account for screening history could introduce significant bias.
Some limitations for the current analysis should be highlighted. The reason for PSA screening tests was not collected, which did not allow us to consider whether prostate-related symptoms prompted screening. When we examined the number of PSA tests in the preceding five years, the median number of tests was five, suggesting that men may be getting a once-yearly screening test as part of a check-up. However, it is likely that some of the men in our study underwent repeat PSA tests after an elevated result, and that prostate cancer was ruled out. This was probably the case for those men (3–6%) who had more than five tests over five years. The PSA test in particular may be prone to underreporting, as it is indistinguishable from any other blood test. Sensitivity and specificity of PSA and DRE self-reported screening were reported as both approximately 0.7 in a meta-analysis, which is reasonable, but still suggests underreporting. 38 However, trained staff in our study explained how the tests would have been done and why, which probably improved the accuracy of self-reported screening. DRE testing was reported independently from PSA, although they may have been performed in combination. Finally, the response rate among the control participants included in this analysis was 56%. This is quite consistent with other case–control studies in recent years, but we cannot rule out that participation bias may play a role.
To our knowledge, our study is the first to specifically investigate the association between prostate cancer screening behaviours and occupation. We found that the longest job held by a man was predictive of whether he had been screened for prostate cancer by PSA and/or DRE test, and that this relationship operated in addition to other known sociodemographic correlates. This is important for a disease like prostate cancer, with largely unknown aetiology, especially as there is growing interest in its potential relationship with occupational carcinogens.
Conclusion
Our results suggest that screening behaviour must be considered when conducting aetiological occupational studies of prostate cancer. Previous studies overlooking screening practices may have had a compromised ability to detect the influence of carcinogenic exposures in the workplace.
Supplemental Material
MSC902485 Supplemental material - Supplemental material for Occupation as a predictor of prostate cancer screening behaviour in Canada
Supplemental material, MSC902485 Supplemental material for Occupation as a predictor of prostate cancer screening behaviour in Canada by Cheryl E Peters, Paul J Villeneuve and Marie-Élise Parent in Journal of Medical Screening
Footnotes
Acknowledgements
We would like to thank the fieldwork team at INRS-Institut Armand-Frappier for their sustained dedication in collecting the data of the PROtEuS study and urologists who granted us access to patients.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for PROtEuS was provided by the Canadian Cancer Society (grants no. 13149, 19500, 19864, 19865), the Cancer Research Society, the Fonds de Recherche du Québec – Santé (FRQS), the Ministère du Dévelopement Économique, de l’Innovation et de l’Exportation du Québec, and the Canadian Institutes of Health Research (CIHR, grant no. PJT-159704). CEP was supported in this work by a GRePEC grant from the Cancer Research Society and from a CIHR Postdoctoral Fellowship. M-EP held career awards from the FRQS.
Supplemental material
Supplemental material is available for this article online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.