
Abstract
Objectives
Given the recent implementation of regional colorectal cancer screening programs in Portugal, understanding patterns of faecal occult blood test and colonoscopy use is essential to improve its control. We aimed to describe the use of both tests and to identify factors associated with its non- and under-use.
Methods
A sample of 7208 subjects aged 50–74 from the National Health Survey 2014 was examined. Previous experience of faecal occult blood test and colonoscopy was classified as never or ever; ever-users, who had last undergone these tests more than 2 or 10 years before, respectively, were considered under-users. We computed age- and education-adjusted prevalence ratios and corresponding 95% confidence intervals for non- and under-use.
Results
Of the individuals in the screening age range, 36.9% had never undergone either test. The prevalence of non-use was 50.7% and 62.2% for faecal occult blood test and colonoscopy, and 27.4% and 6.0% of subjects under-used each test, respectively. The lowest prevalence of non- and under-use was found in the Norte region. Low socioeconomic status and unhealthy lifestyles were significantly associated with low testing; greater use was observed for those having more recent contact with healthcare services.
Conclusions
This study identifies patterns of colorectal cancer screening use, with regional disparities that have not yet been reduced by the implementation of organised screening programmes.
Keywords
Introduction
Colorectal cancer is the third most commonly diagnosed cancer in males and the second in females, with an estimated 1.8 million new cases and almost 881,000 deaths occurring in 2018. 1 Early detection through regular screening from age 50 is effective in decreasing incidence and mortality from colorectal cancer,2–4 but high screening participation rates are essential to achieve this. The European Commission recommends two-yearly screening in men and women aged 50–74, using faecal occult blood testing (FOBT) followed by endoscopic techniques as the confirmatory test. 5 Of the 23 European Union countries that have either implemented or are in the planning phase of the programme, 11 have completed nationwide or regional rollout. 6
In Portugal, population-based programmes exist, but not in all regions. Data to 2016 7 suggest that national coverage (measured by the percentage of health centres offering screening out of the total number of health centres in a region) was 19%, ranging from 4% in the Norte, to 67% in Açores. In 2015 population coverage (measured by the percentage of the population eligible for screening who are invited to screening) reached 28%, whereas adherence to screening (measured by the percentage of the population tested out of those invited to the screening) was 64%. 8 National guidelines published in 2014 made recommendations for opportunistic screening that were similar to those for the organised programmes. 9 Previous studies using data from national health surveys have identified sociodemographic, health-related, and lifestyle factors associated with colorectal cancer screening attendance in the general population at European level (Figure 1), but none has included Portugal. This study aimed to estimate the prevalence of use of FOBT and/or colonoscopy in Portugal, and to identify the factors associated with its non- and under-use.
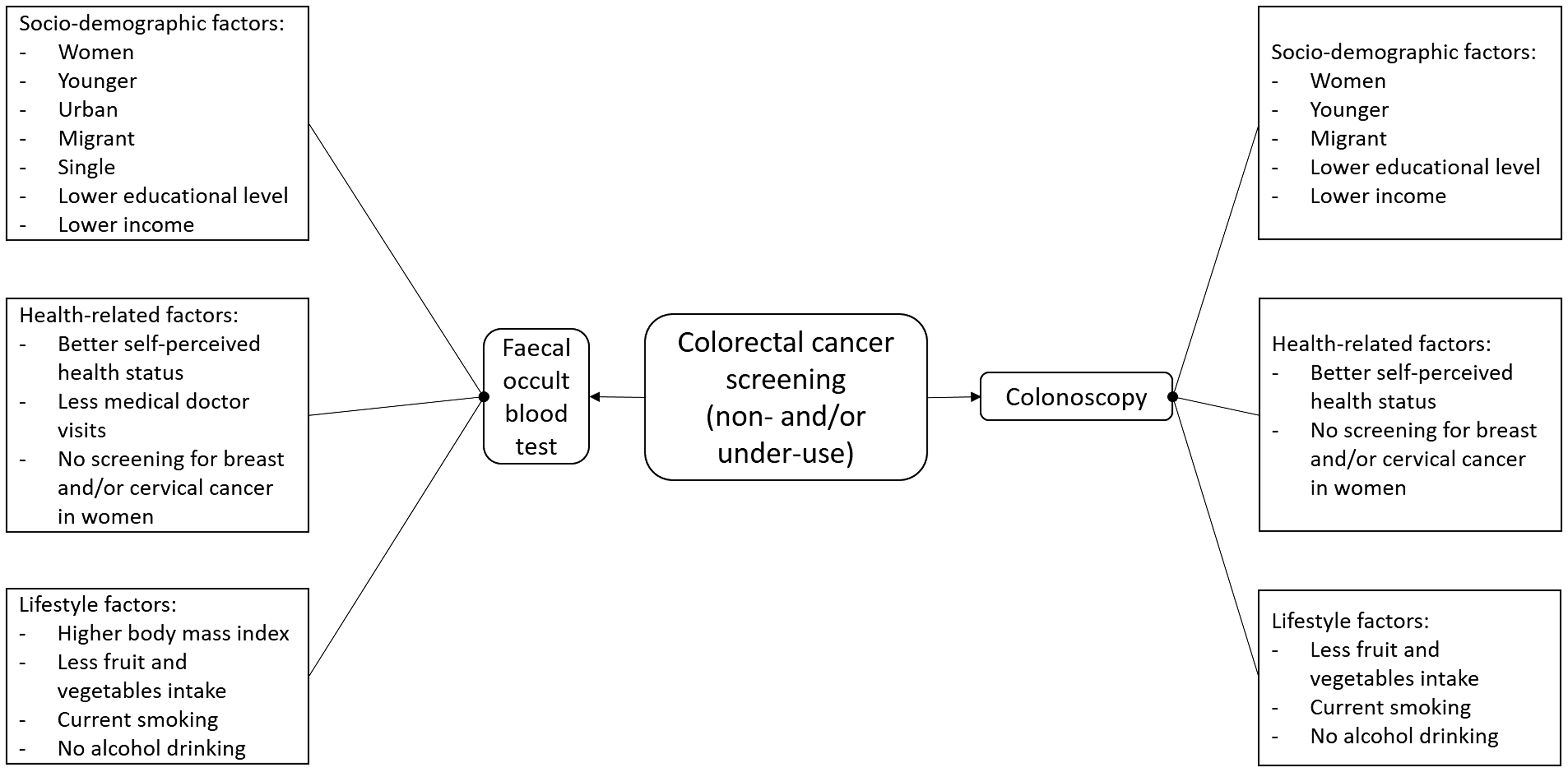
Sociodemographic, health-related and lifestyle factors that have been associated with colorectal cancer screening non- and under-use, for faecal occult blood test and colonoscopy, in previous studies using cross-sectional surveys.12-15, 17-19
Methods
Using data collected as part of the National Health Survey (NHS) 2014, this community-based cross-sectional study evaluated a sample of the Portuguese population (NUTS II – Territorial Nomenclature Units for Statistical Purposes, level II), obtained through multistage stratified and cluster sampling.10,11 The survey received ethical approval, and all subjects interviewed gave signed informed consent. Our specific study was approved by the scientific committee of INE/FCT/DGEEC (process no. 593).
A sample of households was defined, using data from the 2011 Population and Housing Census, to be used as the sampling frame for household surveys conducted by Statistics Portugal. It included 1183 primary sampling units, selected systematically within larger geographical strata, with a probability proportional to the number of households in each unit. A random sample of the households was then selected, and everyone aged 15 or older living in these households at the date of the recruitment was eligible. In each household, the selected individual was the one whose previous birthday was closest to the date of the contact. The sample size was defined to ensure a homogeneous distribution of the participants by the nine NUTS II regions. Between September and December 2014, 22,538 households were contacted and 18,204 persons were evaluated. Information was collected using either computer-assisted personal interviewing, or computer-assisted web interviewing (50% in each regional stratum). The questionnaire covered four themes: health status, healthcare use, health determinants and income, and health expenses.
FOBT and colonoscopy testing was assessed in a section referring to ‘Preventive Care’. To evaluate the prevalence of FOBT use, two specific questions were asked: ‘Have you ever performed a FOBT?’ and, if yes, ‘When was the last time?’, followed by the options ‘in the last 12 months’, ‘between 1 year and less than 2 years’, ‘between 2 years and less than 3 years’, ‘3 years or more’. Similarly, to evaluate the prevalence of colonoscopy testing, the question ‘Have you ever undergone a colonoscopy?’ was asked and, if yes, ‘When was the last time?’, followed by the options ‘in the last 12 months’, ‘between 1 year and less than 5 years’, ‘between 5 years and less than 10 years’, ‘10 years or more’. For all questions, the options ‘prefers not to answer’ and ‘don’t know’ were also available.
Although 18,018 subjects provided information on FOBT and colonoscopy use, our analyses were restricted to those aged between 50 and 74 (n = 7359), the age range most commonly targeted by organised programmes conducted in Portugal.7,8 After excluding subjects with incomplete data on any of the variables analysed in this study (n = 151), the final sample size was 7208. Those who had never undergone FOBT or colonoscopy were classified as non-users. Those reporting previous FOBT or colonoscopy testing were classified as ever users, and were further grouped according to the time since the latest testing: up to 2 years or 2 or more years for FOBT, and up to 10 years or 10 or more years for colonoscopy. Those who had undergone the latest testing 2 or more years, or 10 or more years before the interview were defined as under-users of FOBT and colonoscopy, respectively.
We estimated the prevalence of FOBT and colonoscopy testing and used Poisson regression models to compute age- and education-adjusted prevalence ratios, with respective 95% confidence intervals (95% CI) to identify factors associated with the non- and under-use of FOBT and colonoscopy, separately for men and women. All analyses were conducted with STATA® version 11.2 (StataCorp LP, College Station, TX), using sampling weights computed based on the design weight, i.e. the inverse of the probability of selection of each primary sampling unit, and of each household within each primary sampling unit, further corrected for non-responses, and for the effective number of subjects evaluated, taking into account the age- and sex-structures.
Results
Table 1 summarises the main sociodemographic characteristics of the study population. The sample was mostly composed of married (75.7%) and retired (41.0%) subjects, with more than half having completed the second level of basic education (53.7%).
Characteristics of the study sample (n = 7208).
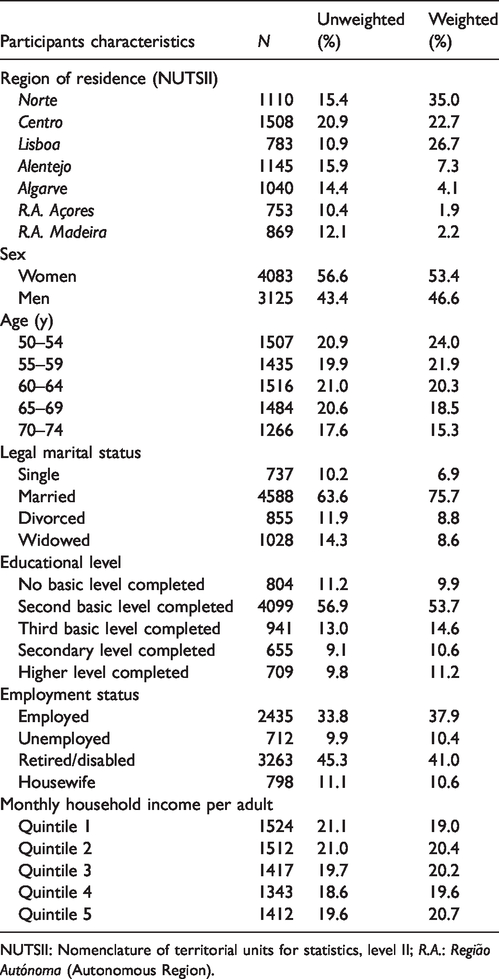
NUTSII: Nomenclature of territorial units for statistics, level II; R.A.: Região Autónoma (Autonomous Region).
The overall proportion of subjects who had never undergone FOBT or colonoscopy was 36.9% (95%CI: 35.2–38.5), with similar proportions in both sexes (women: 36.5%, 95%CI: 34.4–38.7 vs. men: 37.3%, 95%CI: 34.8–39.8, p = 0.654). The overall proportion of individuals who had never undergone FOBT was 50.7% (95%CI: 48.9–52.4), also with similar proportions in both sexes (women: 50.4%, 95%CI: 48.1–52.7 vs. men: 51.0%, 95%CI: 48.4–53.6, p = 0.687). The overall proportion of colonoscopy never-users was 62.2% (95%CI: 60.5–63.9), also with no differences according to sex (women: 64.0%, 95%CI: 61.8–66.2 vs. men: 60.2%, 95%CI: 57.6–62.7, p = 0.134). The highest values of non-use of any type of the tests was observed at age 50–54 in both women (44.4%, 95%CI: 39.4–49.4) and men (45.3%, 95%CI: 39.7–51.1), whereas the prevalence of non-use was lowest at age 60–64 among women (29.7%, 95%CI: 25.8–34.0) and at age 65–69 among men (29.1%, 95%CI: 24.4–34.4). The prevalence of FOBT non-use was highest at age 50–54 in women (56.2%, 95%CI: 51.1–61.4) and age 55–59 in men (56.7%, 95%CI: 51.1–62.4), and lowest at age 60–64 in women (45.5%, 95%CI: 40.8–50.2) and age 70–74 in men (43.7%, 95%CI: 37.5–49.8). For colonoscopy non-use, the highest values were observed at age 50–54 for both women (72.2%, 95%CI: 67.6–76.8) and men (68.9%, 95%CI: 63.4–74.4), and the lowest values were found at age 60–64 in both women (57.1%, 95%CI: 52.3–61.9) and men (55.4%, 95%CI: 49.9–61.0) (Figure 2).
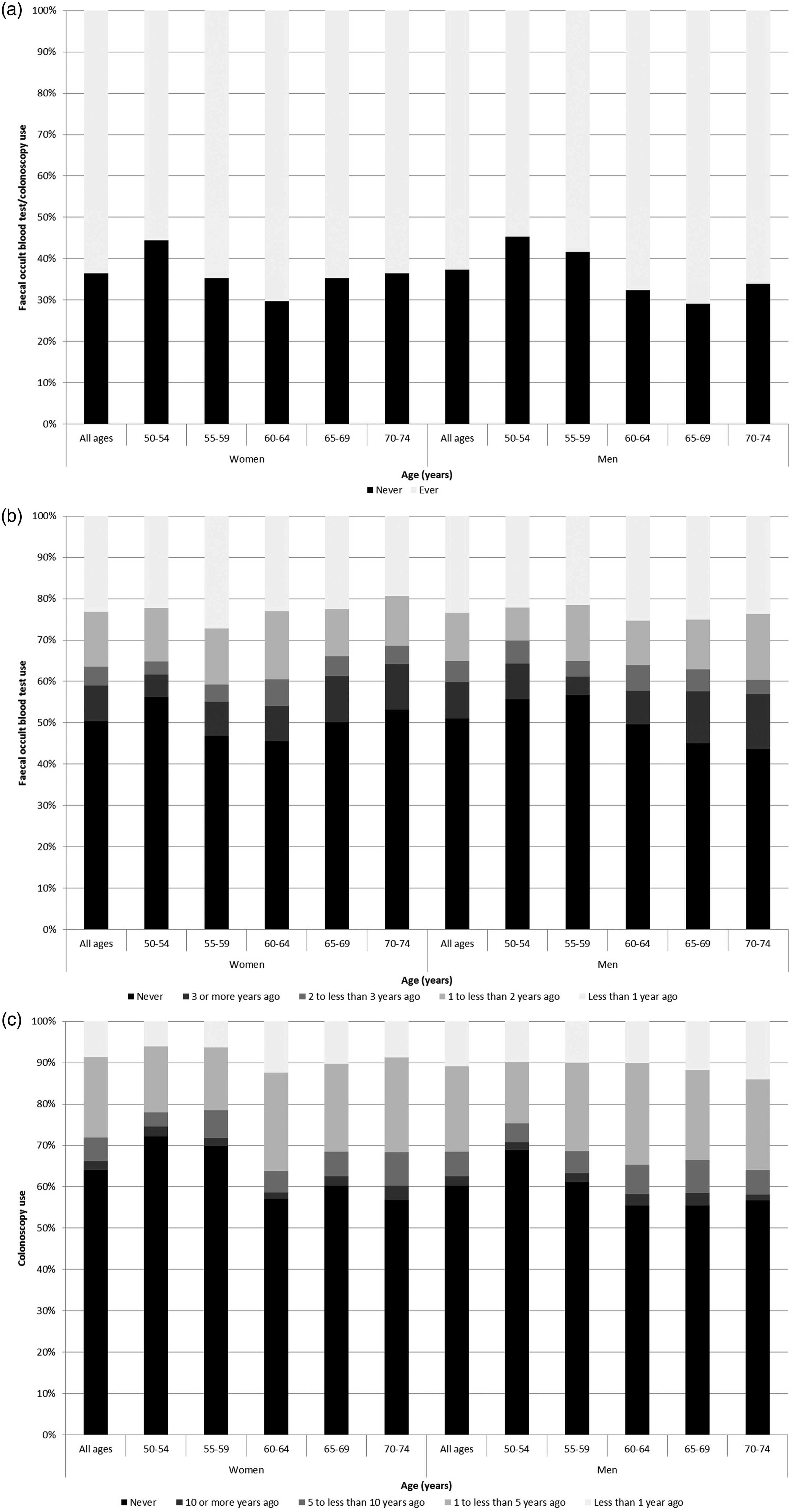
Prevalence of faecal occult blood test or colonoscopy use (a), faecal occult blood test use (b) and colonoscopy use (c) in Portugal among subjects aged 50–74, by sex and age group, according to the elapsed time since the latest testing (b and c).
The association between sociodemographic, healthcare and lifestyle factors, and FOBT or colonoscopy non-use among subjects aged 50–74 according to sex is presented in Table 2. In both sexes, subjects living in any other region showed a higher prevalence of non-use of any test compared with those living in the Norte, as well as individuals living in less populated areas in comparison with those living in densely populated areas. Women from other nationalities were significantly more likely to have never undergone FOBT or colonoscopy when compared with the Portuguese, while the opposite was observed for married men compared with single. A significant decline in the prevalence of non-use of any test was found with increasing education in men only. Among women, retired or disabled and inactive or housewives were less likely to never perform any type of test. A similar result was observed for men living in smaller households. No significant differences in the prevalence of non-use of both tests were observed according to monthly household income, public healthcare provider, or owning private health insurance, except for women in the highest income quintile, who were less likely to have never undergone either test. Men and women who better self-rated their health status were more likely to have never undergone any of the tests. Having been diagnosed with a chronic disease, or having had an appointment with the general practitioner or a specialist doctor in the last year were associated with a lower prevalence of non-use of both tests. The same trend was observed for women who had ever undergone a mammography or a cervical cytology. Overweight women and those having a daily dietary intake of five or more fruits and vegetables were also less likely to have never undergone either test. Current smokers in men were more likely to have never participated in FOBT or colonoscopy.
Determinants of faecal occult blood test and colonoscopy non-use among subjects aged 50–74, according to sex.

CI: confidence interval; PR: prevalence ratio; NUTSII: nomenclature of territorial units for statistics, level II; R.A.: Região Autónoma (Autonomous Region).
aAdjusted for age and education, except in education strata.
bBased on the share of local population living in urban clusters and in urban centres according to Commission Directorates-General for Regional and Urban Policy, Agriculture and Rural Development, Eurostat, Joint Research Centre and OECD.
cOnly asked to women.
dSelf-reported weight and height were used to compute BMI, which was divided into three categories according to the World Health Organization guidelines.
Factors associated with FOBT non- and under-use among subjects aged 50–74 according to sex are presented in Table 3. Compared with Norte dwellers, subjects living in other regions were significantly more likely to have never undergone FOBT. Similar results were observed for under-use, although non-statistically significant results were observed for Lisboa in men, and R.A. Açores and R.A. Madeira in women. While no differences were found for FOBT under-use according to the degree of urbanisation, subjects living in areas of intermediate density, or areas thinly populated, were more likely to never been tested by FOBT. Married men were less likely to have never undergone FOBT, while divorced and widowed women presented a higher prevalence of FOBT under-use. No consistent trend was observed across educational levels. An increase in the prevalence of FOBT under-use was observed for unemployed women and retired/disabled and inactive men, in comparison with employed participants. No consistent differences in the prevalence of FOBT non- and under-use were found according to size of household, or monthly household income, except for men living in households with more than four subjects, who presented a lower prevalence of FOBT non-use. Men who were covered by subsystems other than the national health system were more likely to have never used or to under-use FOBT. A similar prevalence of FOBT non- and under-use was found regardless of whether or not the subjects held private health insurance. Individuals perceiving their health status as good or very good were more likely to have never used FOBT, whereas men with a very good health perception were less likely to under use FOBT. Having been diagnosed with a chronic disease and having had the last appointment with the general practitioner or a specialist doctor in the last year were associated with a lower prevalence of FOBT non-use. A similar result was observed for FOBT under-use only for those who had the last appointment with the general practitioner in the previous year, but an opposite result was found for women being diagnosed with a chronic disease. Women who had ever performed mammography or cervical cytology were less likely to have never undergone FOBT. Small differences in the prevalence of FOBT non-use were observed according to lifestyles, except among men for former drinkers and obese subjects, who were more and less likely to under use FOBT, respectively.
Determinants of faecal occult blood test non- and under-use (more recent test performed ≥2 y ago in those reporting having undergone faecal occult blood test before) among subjects aged 50–74, according to sex.

CI: confidence interval; PR: prevalence ratio; NUTSII: nomenclature of territorial units for statistics, level II; R.A.: Região Autónoma (Autonomous Region).
aAdjusted for age and education, except in education strata.
bBased on the share of local population living in urban clusters and in urban centres according to Commission Directorates-General for Regional and Urban Policy, Agriculture and Rural Development, Eurostat, Joint Research Centre and OECD.
cOnly asked to women.
dSelf-reported weight and height were used to compute BMI, which was divided in three categories according to the World Health Organization guidelines.
Table 4 presents the factors associated with colonoscopy non- and under-use among subjects aged 50–74, according to sex. Overall, most regions presented higher prevalences of non-use when compared with those living in the Norte, especially among women. Although not statistically significant, similar results were found for under-use. Non-Portuguese women were more likely to have never undergone colonoscopy, while married and divorced men presented a higher prevalence of colonoscopy non-use. Overall, more educated men were less likely to have never undergone colonoscopy. While retired and disabled women, as well as inactive men, were less likely to have never undergone colonoscopy, or to under use it, unemployed women were more likely to under use colonoscopy. Size of the household was only significantly associated with colonoscopy non-use among men. A trend towards a lower prevalence of colonoscopy non-use with increasing monthly household income was observed, particularly in women. No differences in the prevalence of colonoscopy non- and under-use were observed according to healthcare provider, but those with private health insurance were less likely to have never undergone colonoscopy. Individuals who rated their health status as good or very good were more likely to have never undergone colonoscopy, whereas men with poor health were less likely to under use it. Reporting a previous diagnosis of chronic disease or having had an appointment with a general practitioner or a specialist doctor in the last year were associated with a lower prevalence of colonoscopy non-use, especially in women. Women who had used mammography or cervical cytology were also less likely to have never used colonoscopy, as well as those with higher fruit and vegetable intakes. An opposite result was observed for current smokers in both sexes.
Determinants of colonoscopy non- and under-use (more recent test performed ≥10 y ago in those reporting having undergone a colonoscopy before) among subjects aged 50–74, according to sex.

CI: confidence interval; PR: prevalence ratio; NUTSII: nomenclature of territorial units for statistics, level II; R.A.: Região Autónoma (Autonomous Region).
aAdjusted for age and education, except in education strata.
bBased on the share of local population living in urban clusters and in urban centres according to Commission Directorates-General for Regional and Urban Policy, Agriculture and Rural Development, Eurostat, Joint Research Centre and OECD.
cOnly asked to women.
dSelf-reported weight and height were used to compute BMI, which was divided in three categories according to the World Health Organization guidelines.
Discussion
Our results show that half of the population in Portugal had never performed FOBT and almost two-thirds had never undergone colonoscopy, despite being in the age range eligible for colorectal cancer screening. Moreover, a segment of the screened Portuguese population does not follow the recommendations regarding the time intervals between tests. In addition to regional variations, patterns of use also differ according to sociodemographic characteristics, and access and use of healthcare services.
Portugal shows more favourable results on colonoscopy use than those observed in 11 other European countries, 12 although the latter evaluation occurred 10 years ago, and for France, Italy, and Spain, increases in colorectal screening uptake have been described in the last decade.13–15
Our results show regional differences in the prevalence of FOBT and/or colonoscopy use, which are not in agreement with the differences observed in organised screening across Portuguese regions.7,8 The Centro region, where the programme has been running for longer, has a low prevalence of FOBT non- and under-use, but the Norte region presents the lowest values in our study, despite having an organised programme that was only initiated after the survey. These differences may be explained by the fact that territorial units used for statistics defined by NUTS II do not entirely correspond to regions covered by each regional health administration responsible for implementing colorectal cancer screening programmes. Conversely, Lisboa, Algarve and Madeira have no organised programme yet, and show similar results to regions with organised programmes.
This study identified other determinants for the non- and under-use of FOBT and colonoscopy. The prevalence of FOBT non-use was higher in people living in less populated areas, probably due to less access to healthcare services in these regions. 16 However, no differences were found for colonoscopy use, in agreement with what has been reported in other European countries.12,17,18 Lower prevalence of non-use of FOBT and/or colonoscopy was observed for married men. In other European countries, some studies have reported no differences according to marital status,13,17,19 while others showed similar results to ours.12,14 However, in our study, only information on legal marital status was available. The prevalence of FOBT and/or colonoscopy non-use was most associated with education level, particularly among men, as in other studies at European level, which found a positive association between higher education and use of screening.12,17,19,20 The prevalence of FOBT and/or colonoscopy non-use decreased with increasing household income, meaning that members of families with better socioeconomic background undergo more screening, in agreement with other studies.12–14,20
FOBT and colonoscopy non-use was lower among subjects reporting a more recent use of healthcare services, as well as in those with a previous diagnosis of chronic disease. This result conforms with other European studies that related more recent visits to the physician and having a chronic disease with higher adherence to screening.13,19 In women, performing cervical cytology and mammography was also associated with a higher prevalence of FOBT and colonoscopy use, and similar results have been previously reported in the French 13 and Italian 15 populations. Another study has shown that the use also increases if potential screeners are more informed about cancer. 17
In contrast, individuals who had a better self-perception of their health status were less likely to have undergone colorectal cancer screening. This result points to the possible need for additional primary prevention efforts targeting this specific group, especially because this finding has also been reported in other studies.12,17,19 Higher testing was also associated with healthier behaviours, in agreement with what has been reported by others.12–15 The association between higher body mass index and lower adherence to colorectal cancer screening12,14 could only be confirmed by our study when analysing the use of both tests.
To our knowledge, this is the first study reporting data on the use of FOBT and colonoscopy from a large representative sample of people living in Portugal, providing information to identify its determinants, but the study has some limitations. First, we did not collect information on personal and family history of colorectal cancer, which could have influenced cancer screening initiation, frequency and choice for test, as it depends on the risk category where family members of a colorectal cancer case may be fitted. 21 The main shortcoming of this study was that it was based on self-reported information. On one hand, social desirability bias may have led to an overestimation of FOBT and colonoscopy use, but on the other, underestimation of the prevalence of use may have occurred because of recall bias, particularly with colonoscopy testing, due to a much wider time interval between tests. We were unable to ascertain detailed data on the type of stool testing for occult blood, immunochemical or other. We cannot verify whether the participants who reported having undergone any of the tests (and particularly colonoscopy) had the test for the purpose of screening, and not as a diagnostic test, nor whether the tests were carried out in an opportunistic or organised setting. Having such information would allow for direct comparison with the annual reports from the organised screening programmes in Portugal,7,8 and with other studies that have evaluated screening programmes at the European level.15,20,22,23 Nevertheless, even when time trends are computed, the original data are based on consecutive cross-sectional surveys,13,14,18,20 which limits the establishment of a causal relation between the use of colorectal cancer screening and independent factors due to the lack of the time sequence.
Conclusions
A considerable portion of the eligible Portuguese population has never undertaken colorectal cancer screening or does not follow the recommendations regarding the time intervals between tests. This study identifies patterns of colorectal cancer screening use, which differ according to sociodemographic characteristics and lifestyles, with low socioeconomic status and unhealthy behaviours significantly associated with low testing, as well as access and use of healthcare services, with greater use being observed for those having more recent contact with healthcare services. This study also points to regional disparities that have not yet been reduced by the implementation of organised screening programmes.
Footnotes
Acknowledgements
The authors thank the Instituto Nacional de Estatística (INE) for providing the data. The Inquérito Nacional de Saúde 2014 was conducted under the supervision of the Departamento de Estatísticas Demográficas e Sociais/Serviço de Estatísticas das Condições de Vida from INE, with the collaboration of the Instituto Nacional de Saúde Doutor Ricardo Jorge and Unit F5 ‘Education, health and social protection’ of Eurostat.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed the following financial support for the research, authorship, and/or publication of this article: The work of BP was co-funded by ‘Fundação para a Ciência e a Tecnologia’ and the ‘Programa Operacional Potencial Humano’ (POPH/FSE) (grant number SFRH/BPD/108751/2015), and the ‘Unidade de Investigação em Epidemiologia - Instituto de Saúde Pública da Universidade do Porto’ (EPIUnit) (POCI-01–0145-FEDER-006862; Ref. UID/DTP/04750/2013).