
Abstract
Background
The aim of the English Bowel Cancer Screening Programme (BCSP) is to diagnose early colorectal cancer and advanced adenomas. However, other findings are also reported at screening colonoscopy. Small studies demonstrate findings other than cancer or adenomas (non-neoplastic findings (NNF)) in 11–25%.
Objectives and setting
Describe the frequency and nature of NNF within the BSCP.
Methods
Data were obtained from the BCSP national database for all individuals undergoing colonoscopic investigation after positive faecal occult blood testing between August 2006 and November 2011. Data included demographics, smoking status, neoplastic findings and NNF.
Results
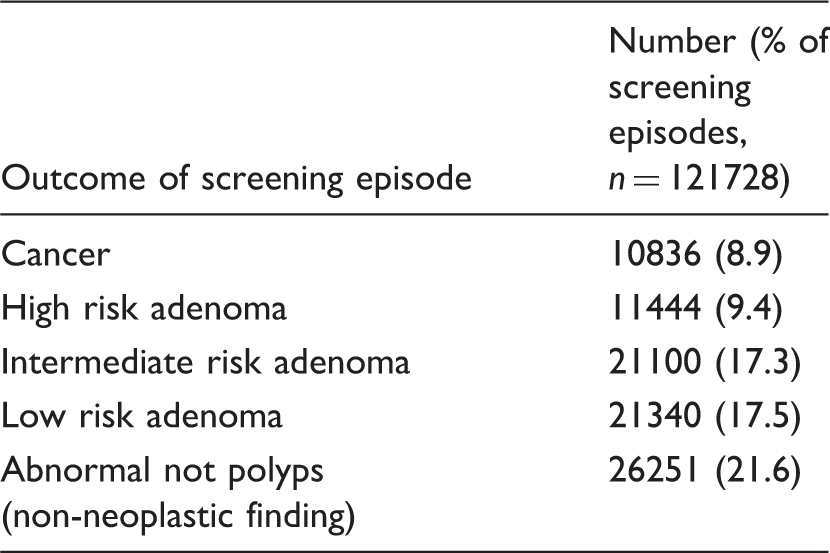
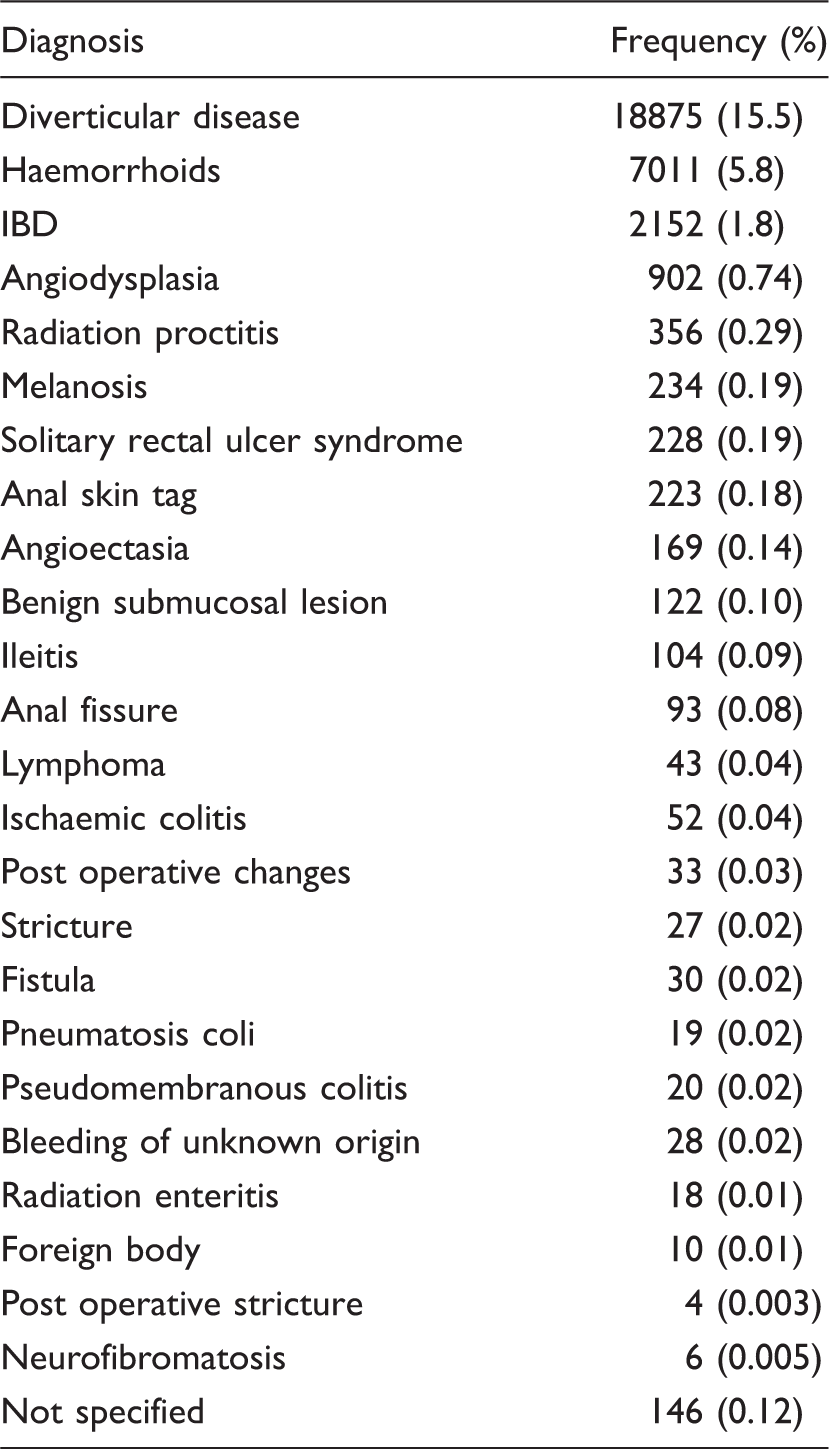
121728 colonoscopies were analysed. ≥1 NNF were found in 26251 cases (21.6%). Diverticular disease (18875 cases) and haemorrhoids (7011) were the most frequently reported. Inflammatory bowel disease (IBD) was reported in 2152 cases. Individuals with a neoplastic diagnosis were less likely to have an NNF than those without (19.8% v 24.4%, p < 0.001). After adjustment for confounding using multivariable analysis, older age was still associated with a small but statistically significant risk of NNF.
Conclusions
The BCSP generates a significant volume of NNF. A small proportion of individuals were found to have inflammatory bowel disease (IBD) - an important diagnosis with implications for long-term management. BCSP participants should be aware that findings other than neoplasia may be detected and the relevance of these findings to that individual is not known. Reporting of NNF varies between colonoscopists, and potential underreporting is a limitation of this study. Further study is required to establish the impact of NNF on primary and secondary care.
Introduction
Cancer screening programmes aim to detect localised cancers or pre-cancerous lesions in asymptomatic individuals, in order to increase the potential for curative treatment, improve survival, and reduce incidence. Findings other than cancer may be identified during the screening process. For breast and cervical cancer screening these are largely of low clinical significance. The English Bowel Cancer Screening Programme (BCSP) has the potential to make a wide range of diagnoses other than cancer or adenoma. Some of these findings may have long-term importance for the health of individuals; however the relevance of many of the findings other than cancer or adenomas is unknown.
The BCSP was introduced in England in 2006. The main aim of the screening programme is to detect colorectal cancer at an earlier stage, with a secondary aim of detecting and removing colorectal adenomas found at colonoscopy in faecal occult blood test (FOBt) positive individuals. Results from the pilot study and early rounds of screening have shown that there is a shift towards detection of earlier stage cancers compared with a symptomatic population.1–3
Individuals attending for screening are informed that conditions such as haemorrhoids may explain positivity of the FOBt, but not that other conditions may be found. 4
To date, two studies from the BCSP have reported a yield of findings other than cancer or adenomas (non-neoplastic findings (NNF)), ranging from 11–25%,2,5 but have not explored these findings in detail.
Studies from other bowel screening programmes have identified lesions other than cancer or adenomas in 24–38%.6,7 Studies reviewing causes for FOBt positivity outside of a formal screening programme have reported a wide variation in NNF of 5–45%.8,9 This variation may be due to methods of reporting. Diverticular disease and haemorrhoids are variably reported, with some studies suggesting that these findings would not cause FOBt positivity.8,9
The aim of this study was to describe NNF generated by the BCSP, in terms of frequency and nature of findings made.
Patients and methods
Study population
The BCSP invites all eligible adults aged 60 to 74 years (the upper age limit was extended from 69 to 74 years in 2010) to undergo screening with a postal FOBt. A description of this testing process is found elsewhere. 10 An invitation to an assessment centre appointment with a Specialist Screening Practitioner (SSP, a nurse trained specifically for the post, and who is present at each step of the screening process after a positive result) is issued to those with a positive result; in >97% of these cases a colonoscopy is offered as further investigation, 11 with less than 3% deemed to be unfit for colonoscopy and instead offered CT colonography, plain CT, or barium enema studies. At the assessment centre, data on smoking status are also collected, recording individuals as current, ex, or non-smokers. Past medical history is noted as reported by the participant. An assessment of symptoms is made, although this has not always been the case throughout the screening programme.
Data collection
All data are entered prospectively onto the BCSP database by the SSP. For this study we identified all individuals with a positive FOBt who went on to have a screening colonoscopy between August 2006 and November 2011, and any subsequent surveillance colonoscopies that were performed within the BCSP on these individuals.
Data were collected on individual demographics (gender, age), smoking status, screening round, clinical outcome, lesion of highest risk (recorded in the BCSP database as cancer detected, high risk polyps, intermediate risk polyps, low risk polyps, abnormal result not polyps, or normal), and details of other findings. Data is recorded either “live” by the SSP during the procedure (when a finding is commented on verbally by the endoscopist), or added at a later date using the finding recorded on the endoscopy report which is produced by the screening colonoscopist. Colonoscopists produce a report on the endoscopy reporting package used in their centre, and are not required to complete a standardized reporting proforma.
The BCSP dataset uses the term “abnormal not polyps” for those colonoscopies where the final outcome is not normal, but not due to a neoplastic lesion. For the purposes of this study we have used the alternative term ‘non-neoplastic finding’ (NNF). For polyps, outcomes are categorized according to the British Society of Gastroenterology surveillance guidelines as low risk (1 or 2 small (<1 cm) adenomas), intermediate risk (3 or 4 small adenomas, or at least one >1 cm), or high risk (either ≥5 adenomas, or ≥3 adenomas, one of which is >1 cm). 12 For diagnoses where histological samples are taken, the BCSP database entry is finalized once the histology results are available.
Data analysis
Normally distributed continuous data are presented as mean (standard deviation, SD). Non-parametric data are presented as median (interquartile range). Univariable analysis was performed using chi-squared test for categorical data and the t-test for parametric continuous data. Multivariable analyses were performed using binary logistic regression, with presence or absence of an NNF as the dependent variable. Potential variables were included in the model if the p value for their association with the outcome was <0.01 in univariable analysis. Statistical analysis was performed with SPSS version 19 (Chicago, USA). P values were considered significant if <0.05. All tests were 2 sided.
Results
Major outcomes at colonoscopy amongst individuals with a positive FOB test.
Frequency of non-neoplastic findings.
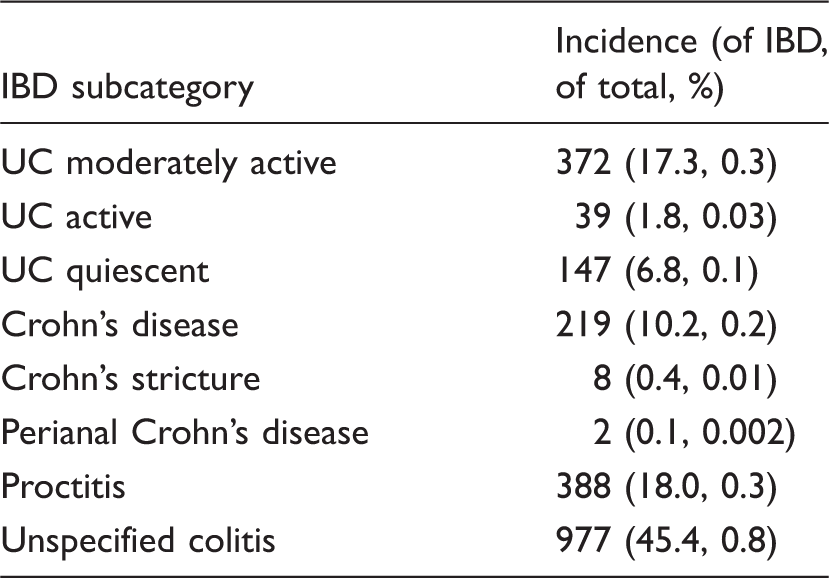
IBD diagnoses.
Age, gender and smoking
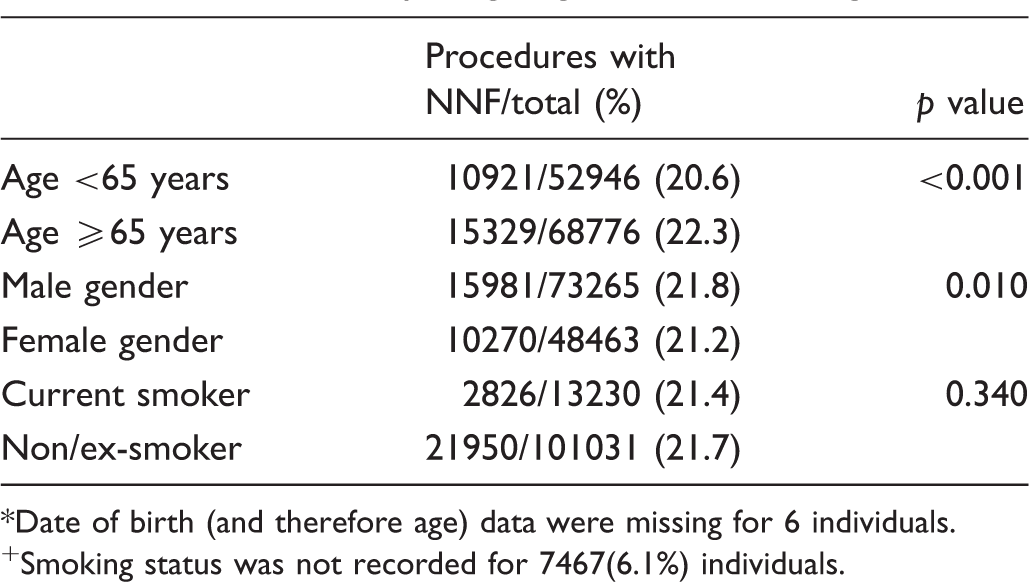
Date of birth (and therefore age) data were missing for 6 individuals.
Smoking status was not recorded for 7467(6.1%) individuals.
Presence of neoplasia
Presence of NNF according to grade of polyp

Discussion
This paper demonstrates that a diagnosis other than cancer or polyps is recorded in over one fifth of procedures within a national bowel cancer screening programme. The aim of the screening programme is to diagnose and prevent colorectal cancer, and it is important that other findings are considered in terms of their clinical relevance.
A weakness of this study is the subjective nature of reporting of NNF, which is dependent on the opinion of the endoscopist and may be influenced by other findings at colonoscopy. Individuals with a neoplastic diagnosis were less likely to have an NNF. It may be that, where a neoplastic diagnosis is made, the endoscopist attaches less significance to an NNF. If the endoscopist does not feel that the NNF has contributed to the FOB positivity, they may be less likely to report it. Alternatively, where an NNF is observed, the absence of a neoplastic lesion likely to be capable of generating a positive FOBt may lead the endoscopist to suggest that the positive FOBt was due to the non-neoplastic diagnosis. That is, the endoscopist may report the NNF as an explanation for the positive FOBt. As clinicians are not required to complete a standardised reporting proforma, and instead use the endoscopy reporting system at their screening centre, variation in reporting styles will have influenced the results of this study.
We cannot take the rates of NNF as an indication of prevalence of conditions, due to the mixture of incident and prevalent screening rounds, and index and surveillance colonoscopies in the dataset. We instead give an indication at the per colonoscopy level of the NNF that may be identified.
All screening programmes have the potential to generate non-cancer diagnoses. The lung cancer screening arm of the USA Prostate, Colorectal, Lung and Ovarian (PCLO) screening programme trial (a large population based randomized trial by the National Cancer Institute) reported 34.5% of chest X-rays (CXRs) as “abnormal but not suspicious for cancer”. 13 This is in comparison with CXRs suspicious for cancer, constituting 8% of the X-rays performed. The authors conclude that some of these abnormalities (which include granuloma, pulmonary fibrosis, bone and soft tissue lesions, cardiac abnormalities and COPD and emphysema) are associated with increased risk of developing lung cancer, and/or increased overall mortality. This is similar to the findings in the BCSP – some potentially increasing the future risk of bowel cancer, and some, such as IBD, diverticulitis and lymphoma, carrying potential mortality risks. The ovarian screening arm of the PCLO trial also reported benign neoplastic and non-neoplastic findings as common. 14 A study of screening for colorectal cancer using CT colonography detected colorectal cancer in 0.21% and an extracolonic cancer in 0.35% of subjects. 15 These extracolonic cancers were most frequently renal cell carcinomas and lymphoma, clearly carrying great clinical relevance for the individual. That study focused on extracolonic cancer findings; little was made of bowel diagnoses other than cancers and polyps.
It is important that the relevance of non-neoplastic findings and the potential impact of these findings for individuals and for health service resources are considered. Careful consideration must also be given to how these potential findings are communicated to the individual. For some NNF, treatment is likely to be required, but for other findings it is less clear what the significance is, particularly if individuals are asymptomatic.
A relatively large number of individuals were found to have the potentially significant diagnosis of IBD. These include individuals with both quiescent and active disease. There are no evidence-based guidelines for the management of asymptomatic individuals found to have IBD, or studies on the natural history of IBD before symptoms develop. A large European study of incidence of IBD actively excluded asymptomatic cases and those identified during a screening activity. 16 An early UK colorectal screening programme 17 identified 8 cases of previously undiagnosed IBD in a cohort of 481 individuals with positive FOBt who underwent investigation of the colon, as well as 2 previously known cases. Further data from this centre later demonstrated 53 cases of previously undiagnosed IBD from approximately 2000 people with positive FOBt. This equates to 2–2.5% of those undergoing investigation for positive FOBt, similar to the proportion in this study.
People known to have IBD can participate in the BCSP. Many are in surveillance programmes already, and therefore may elect not to undergo investigation of their positive FOBt within BCSP. They are given the option of going ahead with BCSP colonoscopy if they wish, and as a result, some cases of IBD detected within the programme are known cases. However, we assume a percentage of the IBD detected in the programme to be a new diagnosis. We consider it relevant to report all IBD detected, as this is a descriptive study of the findings at screening colonoscopy. The current BSG guidelines 18 state that therapy “may not be required” in those with active ileal, ileo-colonic or colonic Crohn’s disease detected at bowel cancer screening. However, there may be benefit in treating individuals to prevent disease progression and long-term complications. 19 Subjecting individuals to long-term treatment where the benefit of treatment is unknown merits careful consideration of the risks and benefits.
The largest group of NNF are those in individuals identified with diverticular disease. Diverticular disease is common within the general population, 20 and in many cases may be a finding with no relevance to the individual. The natural history of diverticular disease in the population studied is not known. It is important, before giving an individual this diagnosis, that the clinical relevance and the opportunity to improve the natural history of the condition is considered. Individuals who are given a diagnosis that may not require any further medical input should be given the information in a manner that explains the findings and the implications of the findings. They should also be advised on the potential future relevance of the findings, for example, if symptoms develop. Due consideration should also be given to establishing how much information the individual wishes to receive about findings other than those that the screening programme aims to identify.
Prior to their procedure, individuals are given information leaflets including discussion about the possibility of a cancer or a neoplastic diagnosis; they are informed that conditions such as haemorrhoids may be found to explain FOB positivity, but not that other non-neoplastic conditions may be diagnosed. 4 A more detailed discussion at the assessment centre after a positive FOBt may be needed, in order to make individuals fully aware of what a colonoscopy may identify, along with a full explanation of findings after the procedure. There is currently no guidance for colonoscopists regarding reporting of other findings, and reporting may be subjective.
The presence of symptoms may be important. In a study from the authors’ centre, 21 the highest reporting of symptoms was in the group with a final diagnosis that was non-neoplastic (75% compared with 70% in those with a cancer diagnosis and 62% with a normal colonoscopy). Of the individuals with symptoms and an NNF, 60% had not attended their GP on account of their symptoms. A study of the factors that affect attitude to colorectal cancer screening 22 found that the presence of symptoms was associated with a positive attitude towards screening. It has also been demonstrated that the presence of multiple symptoms causes a perception of higher bowel cancer risk, 23 and this has an effect on screening uptake. The reviews of the first two rounds of the screening pilot alluded to the generation of work for primary care,24,25 but the potential for this to include continuing management of NNF was not considered at the time. This highlights an area for future research.
Conclusions
The BCSP generates a significant volume of non-neoplastic findings. It is important that findings are correctly interpreted so that incidental findings do not become diagnoses, and so that individuals attending for screening are not wrongly turned into patients.
IBD is an important and common diagnosis, and identifying it may have important implications. The significance of other findings, such as haemorrhoids or diverticular disease, is not known, and screening programmes must carefully consider the way in which these findings are communicated. Individuals should be informed prior to colonoscopy that there may be “other findings”, with some explanation about the likely relevance to the participant of such a finding. Correlation with the presence of symptoms may be important in deciding ongoing management of an NNF.
The burden of NNF generated by the BCSP nationally has not been investigated previously, and the relevance of NNF, relation to symptoms, and impact on individuals and on primary and secondary care requires further study.
Footnotes
Acknowledgments
We wish to acknowledge the contributions made by South of Tyne Bowel Cancer Screening Centre, Gateshead, UK, Bowel Cancer Screening Programme National Office, Sheffield, UK, and Dr Praveen Rajasekhar, South Tyneside General Hospital, UK.
Some content in this manuscript has been presented as a poster presentation (BSG 2012, abstract: Gut 2012; 61(Suppl 2):A376) and oral presentation (UEGW 2012, abstract: Endoscopy 2012; 44(Suppl 1):A84).
There are no conflicts of interest and this research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.