
Abstract
Objective
To assess the effectiveness of the current cervical cancer screening tools in Western Kazakhstan.
Methods
Smears taken through (i) conventional cytology using azur-eosin staining and (ii) liquid-based cytology (LBC) ‘Cell Scan’ in the general female population and in women first diagnosed with cervical cancer were collected throughout the region. ROC-analysis with curve construction and weighted Cohen's κ calculation were applied. A total of 494 cytological pairs were collected, including 94 sets with histology findings.
Results
The conventional (azur-eosin staining) technique contained 0.2% non-informative material and LBC ‘Cell Scan’ had 5.9%. Area under the curve was 0.95 for the conventional technique and 0.92 for ‘Cell Scan’ (p > 0.05). The conventional smears showed κ 0.62, sensitivity 90.4% at specificity 90.0% for CIN2+, while LBC ‘Cell Scan’ smears showed κ 0.47, sensitivity 83.3% at specificity 92.5%.
Conclusions
In this analysis it was not possible to prove that the LBC ‘Cell Scan’ technique was superior to its predecessor, azur-eosin staining. These findings highlight the need to modify the current screening programme according to updated international scientific evidence on effective screening design, such as the use of HPV DNA testing with Pap smear triage in women aged 30 or older. Further research, and a Health Technology Assessment, are necessary if we wish to establish a national standardized screening programme using the available technology appropriately.
Introduction
Diagnoses of cervical cancer are predicted to rise by at least 25% by 2030, mainly in low- and middle-income countries. 1 From 1999 to 2008 the annual incidence rate of cervical cancer in Kazakhstan was 14.5 ± 0.3, with 8.0±0.1 mortality per 100,000 women, 2 but by June 2019 the incidence rate had risen significantly, to 18.2 per 100,000 women. 3
The national screening programme, implemented from 2008, initially included conventional Pap-testing performed by trained midwives every 5 y in the target group of women aged 30–60. From December 2017 the screening interval was reduced to 4 y, and the target group was extended to age 70. In 2013, liquid-based cytology (LBC) using the ‘Cell Scan’ technology (IMSTAR Lab, France) was introduced. According to IMSTAR (www.imstar.fr), the test specificity is >85% and sensitivity >90%. This technique was introduced in Kazakhstan without a Health Technology Assessment, and we have been unable to find any peer reviewed publications on the effectiveness of this technology in the literature. ‘Opportunistic screening’ in Kazakhstan is usually performed through the conventional method with azur-eosin staining, mainly in private clinics, but the coverage rates are not available.
According to research from the Kazakh Institute of Oncology and Radiology, cervical cancer screening coverage decreased from 72.9% in 2008 to 45.9% in 2016. The proportion of pre-cancers detected was still insufficent, at 50.8%, in 2016, when the standardized mortality rate for cervical cancer reached 7.1 per 100,000. 4
The growth of cervical cancer incidence, despite the national programme, suggests that the screening strategy in Kazakhstan should be re-examined. Cervical screening through human papillomavirus (HPV) testing is now widespread throughout the world,5–7 with a majority of countries, including relatively new members of the European Union from Eastern Europe, changing or adapting their national programmes to primary HPV testing in women aged 30 and older.8–12 In Kazakhstan, this policy has not been adopted, regardless of the guidelines and health technology assessments confirming the advantages of HPV primary screening.13–15
We here aim to assess the diagnostic value of both techniques currently in use in Western Kazakhstan, with a view to informing a Health Technology Assessment plan to update the screening paradigm.
Methods
This analysis included the general female population aged 18–60, and women with newly diagnosed cervical cancer, who signed the Informed Consent form. Data were collected in outpatient clinics in cities and rural smaller towns across four western provinces of Kazakhstan: Aktobe, West Kazakhstan (Uralsk), Mangystau (Aktau), Atyrau. To reach a wider female population and avoid possible bias, we included a range of medical settings: state-sponsored, insurance, and private. In women with cervical cancer, smears were collected in Aktobe’s University Hospital and in regional Oncology Centres, and these participants were included regardless of age and the disease stage. Women with a history of HPV vaccination were excluded, and cancer patients with a history of any intervention (surgery, chemotherapy, radiotherapy) were also excluded. HIV status and first trimester pregnancy were not exclusion criteria. The data collection routine is presented in Figure 1.
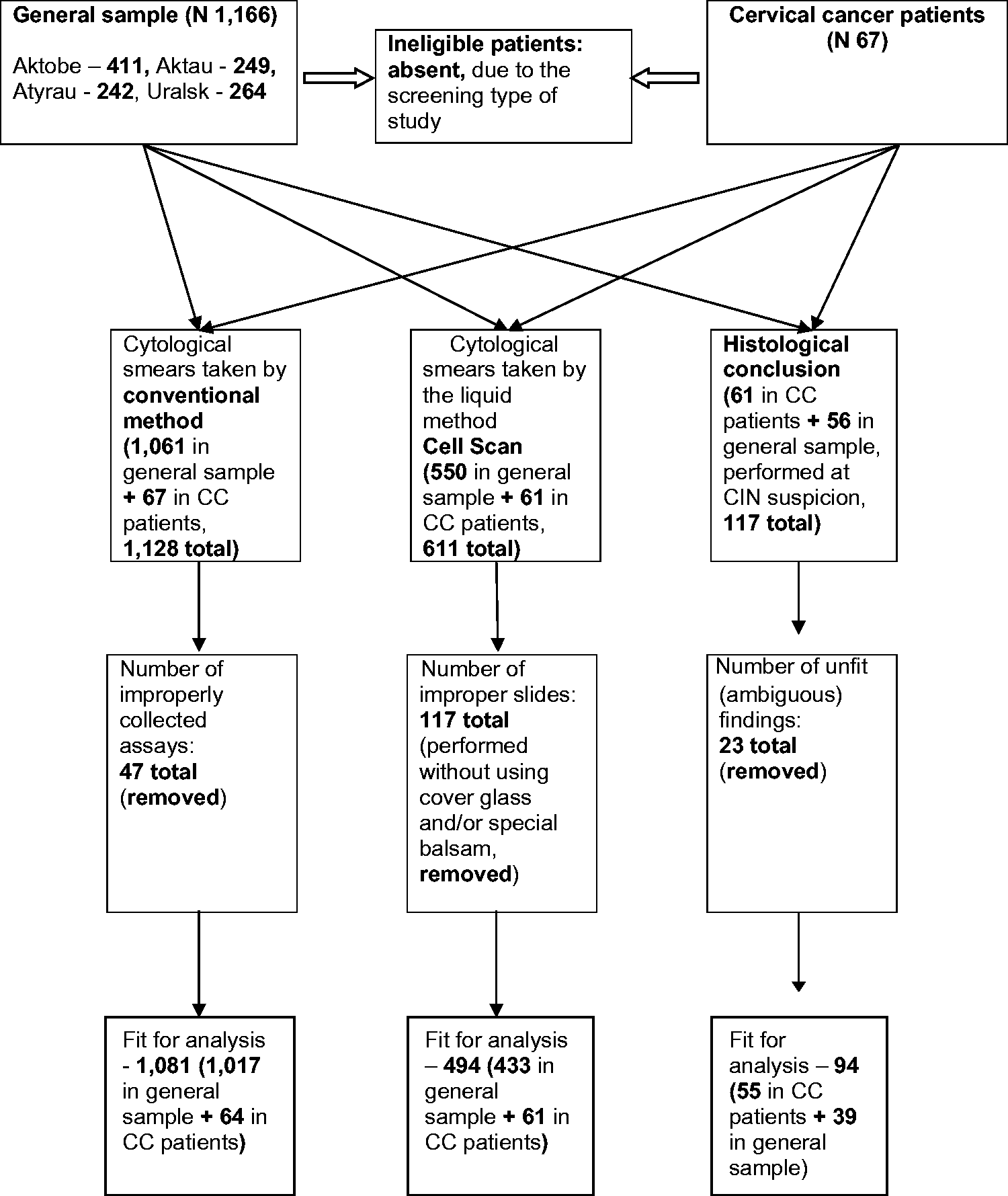
Flowchart of the study.
We collected the two smears from the women at the same time: using special cytobrushes for LBC ‘Cell Scan’, which were then placed into vials with the preservative fluid, and also for conventional cytology (azur-eosin staining). Slides preparation was performed using the Cell Scan-100 (semi-automatic) and Cell Scan-200 (automatic) devices with haematoxylin-eosin staining. Interpretation of the material obtained was based on The Bethesda System (TBS) terminology reporting (we used TBS 2011, as the research started before the 2016 edition). 16
To assess the two screening tests, we compared a set of performance indicators. To calculate indexes where an independent evaluative parameter is needed, we used 94 available sets of histological (biopsy samples)/LBC ‘Cell Scan’ azur-eosin cytological findings collected simultaneously from the same patient. To identify the concordance of smears obtained by the two methods, all 494 pairs were analysed by matching. We adapted the classification of cervical smears by Papanicolaou to allocate our findings according to epithelial damages. The C category 1 included normal cytological findings, with no signs of atypia. The concept of ‘normal cytology’ has been extended to the NILM (negative for intraepithelial lesions or malignancy) in recent years, and therefore TBS categories C, D, E and G1 corresponded to NILM. 17 In category 2 we allocated AS-CUS (questionable with respect to atypia results) and also AGC-NOC (dubious changes in the glandular epithelium). In category 3 we included LSIL (CIN1). Accordingly, we placed high-grade squamous intraepithelial lesions (HSIL) (CIN2+) in category 4, and AGC and invasive cancer in category 5.
Calculations were performed in Statistica.10 (Dell Technologies, TX, USA). For all tests a two-tailed type I error of p<0.05 at 95% confidence interval (CI) was assumed statistically significant. Non-parametric operational tests were used due to data not being normally distributed. Common practice to measure the strength of agreement between the diagnostic tests was applied: ROC-analysis (using Stata 15.1, StataCorp, 2017, College Station, TX) with curve construction and Kappa statistics (weighted Cohen's κ, calculated in MedCalc, www.medcalc.be).
Ethical approval for the study was provided by the West Kazakhstan Marat Ospanov Medical University’s Institutional Review Board (Minutes No. 3, October 09, 2014). The Informed Consent Form was designed according to the World Health Organization guidelines, and all participants who signed the form were comprehensively informed concerning purposes of this research and provided their clear consent to participate. The study is retrospectively registered in ISRCTN registry, No. ISRCTN71514910 (2 January 2018).
Results
A total of 494 LBC ‘Cell Scan’ and conventional azur-eosin smears were collected (see Figure 1). Results obtained through the two methods in the general female population (cervical cancer negative) are presented in Table 1. We found 5.9% of inadequate smears for LBC ‘Cell Scan’ vs. 0.2% for azur-eosin staining in the 433 paired samples (61 were cervical cancer).
Cytological findings obtained by conventional and LBC techniques in general sample, cervical cancers excluded (N = 433).
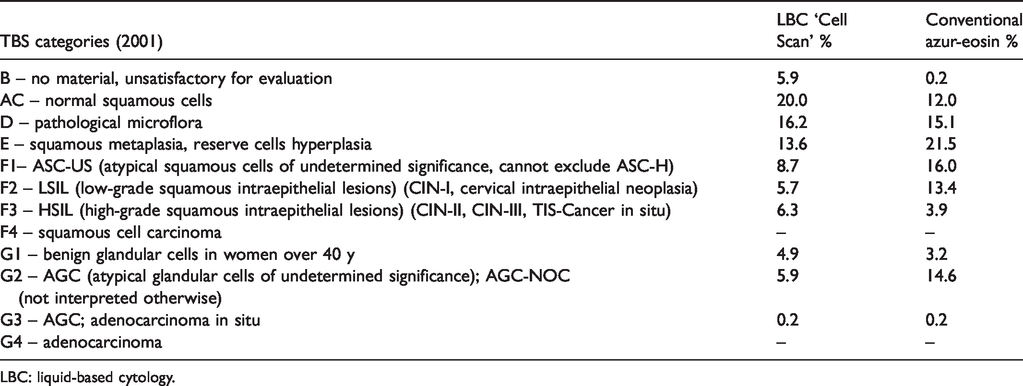
LBC: liquid-based cytology.
For the analysis of attributive agreements, 94 sets of histological, liquid and conventional assays were available, of which there were 55 with CIN2+, and 39 with CIN1 and lower results. Concordance between cytological and histological findings when combined into categories is presented in Table 2.
Cross-checking categorization of cases by histology and cytology, for LBC ‘Cell Scan’ and conventional azur-eosin (N = 94).
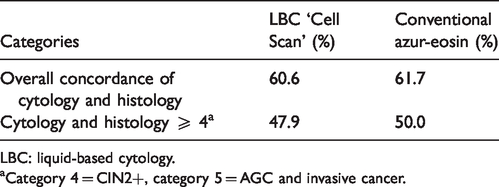
LBC: liquid-based cytology.
aCategory 4 = CIN2+, category 5 = AGC and invasive cancer.
Concordance of the cytology results with histology was 60.6% in the LBC ‘Cell Scan’ group, compared with 61.7% in the azur-eosin conventional group. When looking only at categories ≥4, this concordance decreased to 47.9% in the LBC ‘Cell Scan’ group and 50.0% in the azur-eosin group. Kappa statistics resulted in weighed κ for LBC ‘Cell Scan’ 0.47±0.08 (95% CI 0.31;0.63) vs. 0.62±0.08 (95% CI 0.46;0.78) for conventional technique, in MedCalc. The ROC curve (Figure 2) outlines no statistically significant difference (p>0.05) due to the mentioned shortness in observations (94 available sets).
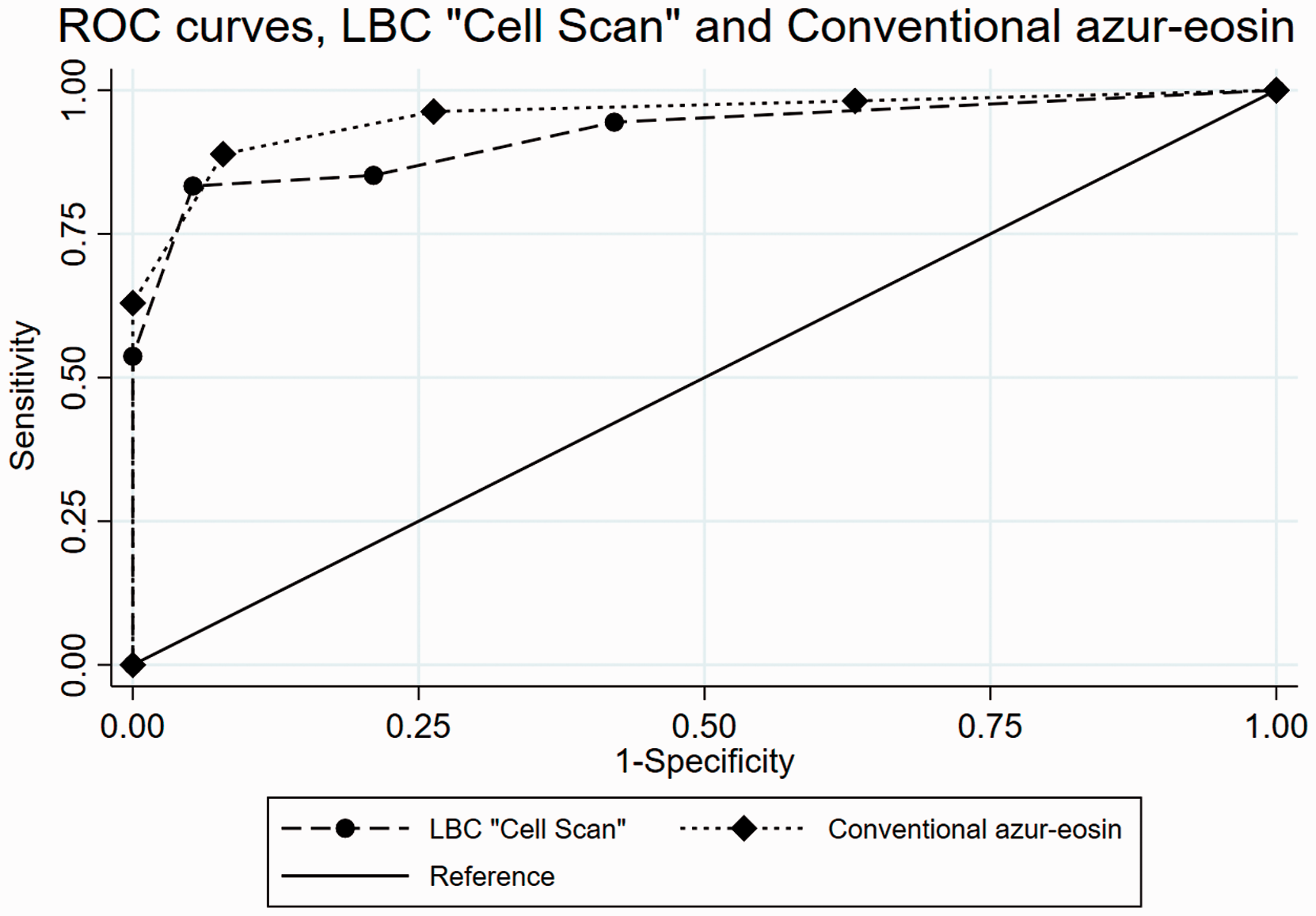
ROC-curve for the two cytological tests. LBC: liquid-based cytology.
The area under the curve was: 0.92±0.002 (95% CI 0.86;0.97) for LBC ‘Cell Scan’ and 0.95±0.003 (95% CI 0.91;0.99) for azur-eosin staining, (p>0.05). Table 3 shows the coordinates of the obtained ROC curve.
Coordinates of the obtained ROC curves and proportion correctly classified.

LBC: liquid-based cytology.
The LBC ‘Cell Scan’ and conventional azur-eosin methods had, respectively, sensitivity 83.3% and 90.4%, and specificity 92.5% and 90.0% at cutpoint ≥4 (CIN2+), without statistically significant differences. Placing the cutpoint at category 5 (AGC and cancer) resulted in substantially decreased sensitivity of both tests.
Discussion
Despite excluding all inadequate smears and slides, for the LBC ‘Cell Scan’ technique, the amount of unsatisfactory smears was almost three times beyond the international standards, compared with adequate values for the conventional azur-eosin method. By comparison, research from India revealed opposite findings, of 1.61% for LBC vs. 7.1% for conventional smears. 18 It is worth mentioning that in 2015–2016 large numbers of unfit ‘Cell Scan’ membrane filters were discovered throughout Western Kazakhstan, and reported to the Health Authorities. Exact data on the quantities of defective supplies are not available, but this situation forced state-sponsored screening settings to duplicate the ‘Cell Scan’ smears with conventional ones, in order to check the true state of the cervix. By 2017 the situation had improved, presumably because the manufacturer streamlined the quality control of membrane filters.
Beyond the problematic smears adequacy, our study results did not demonstrate superiority of the LBC ‘Cell Scan’ system over the conventional method in any of the examined indicators relating to cancer detection. According to the Delphi study results on a system to evaluate the quality of any organized cancer screening, cancer detection rate is one of the decisive indicators. 19
Azur-eosin staining by hand is far from being a standard in cytology, as its diagnostic sensitivity is inferior to that of LBC preservative fluids approved by the United States Food and Drug Administration. In addition, the haematoxylin staining used in the Pap-test provides a better picture of the atypia of the cellular nucleus than the azur. 20 The conventional method is also operator dependent, as the thickness of the smear varies significantly. Despite these shortcomings, in the context of Western Kazakhstan, the implementation of the LBC ‘Cell Scan’ smear did not prove to be advantageous over the conventional azur-eosin. It follows that an assessment of the impact of the ‘Cell Scan’ preservative fluid within a standardized screening programme (aiming for the highest possible coverage) needs to be performed in this setting, ideally through a health technology assessment.
According to data based on about one million women screened, ‘most of the reassurance of safety provided by a co-test (a Pap smear together with an HPV test) derives from the HPV test’, 21 but a negative HPV test is more reassuring than a negative cytological test, as the latter has a greater chance of being falsely negative. 22 In a joint document dated 2016, the Pan American Health Organization, World Health Organization, and American Centers for Disease Control summarize the evidence on the integration of HPV testing in screening programmes. They include the HPV test with triage cytology for positive women among the valid options for updating current screening programmes. 23 Aside from the triage, the use of cytology in a co-test has been recently limited only to the follow-up of patients who had been treated for cervical lesions. If they reach the end of a follow-up period without a recurrence, they go back to the periodic HPV testing. 24 The range of cervical screening models allows each country to design its own algorithm, accounting for socio-demographic factors and economic implications of introducing HPV testing, in particular in the context of HPV vaccination.10,25 Low-income countries are also able to change or adjust their approaches to face the most significant challenges caused by cervical cancer. 26
This study is the first to present the diagnostic value of the tests utilized in Western Kazakhstan, providing evidence for advocating the update of the national screening programme. The study has a number of limitations, including the relatively small number of observations and the low translatability of our findings. Only a few countries utilize the azur-eosin staining by hand and the LBC ‘Cell Scan’, but we could not find relevant comparative reports. HPV genotyping would have improved the comparability with similar studies, but this is currently not available in Kazakhstan, and so could not be performed in this study. 27
Conclusions
In the context of Western Kazakhstan, and using the available data, we were not able to find improvements in the detection of cervical abnormalities with the ‘Cell-Scan’ LBC technology compared with the conventional azur-eosin staining, despite the shortcomings of the latter. As programmes worldwide progressively shift to HPV testing in women from age 30, priority should be given to identifying the most appropriate screening design, including in this assessment the tests of choice, screening intervals, target age group, and interaction with the vaccination services. A Health Technology Assessment is advisable, in order to establish a universal and standardized cervical screening programme in Kazakhstan.
Supplemental Material
MSC885409 Supplemetal Material - Supplemental material for Cervical screening in Western Kazakhstan: Liquid-based cytology ‘Cell Scan’ versus azur-eosin staining
Supplemental material, MSC885409 Supplemetal Material for Cervical screening in Western Kazakhstan: Liquid-based cytology ‘Cell Scan’ versus azur-eosin staining by Saule Balmagambetova, Giovanni Gabutti, Arip Koyshybaev, Cecilia Acuti Martellucci, Olzhas Urazayev, Kanshaiym Sakiyeva and Karlygash Bekova in Journal of Medical Screening
Footnotes
Availability of data and materials
All data generated or analysed during this study are included in this published article (dataset on 94 histology/cytology findings is presented in supplementary file 1). The other datasets used and/or analysed during the current study are available from the corresponding author on request.
Authors’ contribution
S Balmagambetova: article search, data extraction, assessment of methodological quality, data analysis, drafting the manuscript. G Gabutti: conception and design, commented critically; editing and approving the manuscript. A Koyshybaev: assessment of methodological quality, data analysis, drafting the review. C Acuti Martellucci: data analysis, drafting the manuscript. O Urazayev: data extraction, data analysis. K Sakiyeva: article search, commented critically. K Bekova: data extraction, data analysis.
Acknowledgements
We thank Dr. Klara Sarkulova, Head of the Aktobe cytological lab at the Regional Pathomorphological Bureau, and Dr. Laura Yakupova, Head of the Uralsk cytological laboratory for processing cytological and histological findings in frames of this research.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research has been performed in the framework of the scientific Project ‘Epidemiological analysis of Human Papillomavirus in Western Kazakhstan in relation to HPV-attributable cervical pathology – social, clinical and genetic aspects’, funded by the Committee of Science of the Ministry of Education and Science of the Republic of Kazakhstan (grant no. 2230/GF4, State registration no. 0115РК01224). Giovanni Gabutti declares that he received grants from Sanofi Pasteur MSD, GSK Biologicals SA, Novartis, Pfizer, Sanofi Pasteur, MSD Italy, PaxVax and Seqirus for taking part in advisory boards and expert meetings, acting as speaker and/or organizer of meetings/congresses, and as principal investigator and chief of O.U. in RCTs.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.