
Abstract
Objectives
Risk stratification may improve the benefit/harm ratio of breast screening. Research on acceptability among potential invitees is necessary to guide implementation. We assessed women’s attitudes towards and willingness to undergo risk assessment and stratified screening.
Methods
Women in England aged 40–70 received summary information about the topic, and completed face-to-face computer-assisted interviews. Questions assessed willingness to undergo multifactorial breast cancer risk assessment, more frequent breast screening (if at very high risk), or less frequent or no screening (if at very low risk), and preferences for delivery of assessment results.
Results
Among 933 women, 85% considered breast cancer risk assessment a good idea, and 74% were willing to have it. Among 125 women unwilling to have risk assessment, reasons commonly related to ‘worry’ (14%) and ‘preferring not to know’ (14%). Among those willing to have risk assessment (n = 689), letters/emails were generally preferred (42%) for results about very low-risk status. Face-to-face communication was most commonly preferred for results of very high-risk status (78%). General practitioners were most commonly preferred sources of assessment results (≈40%). Breast cancer specialists were often preferred for results of very high-risk status (38%). Risk-stratified breast screening was considered a good idea by 70% and 89% were willing to have more frequent screening. Fewer would accept less (51%) or no screening (37%) if at very low risk.
Conclusions
Women were generally in favour of multifactorial breast cancer risk assessment and risk-stratified screening. Some were unwilling to accept less or no screening if at very low risk.
Introduction
The Breast Screening Programme in England currently invites all women aged 50–70 for mammography on a triennial basis. However, there is growing interest in whether the balance of harms and benefits of screening could be improved by estimating women’s personal risk status, and tailoring screening accordingly. For example, the Tyrer–Cuzick model estimates breast cancer risk based on a range of factors, including body mass index, family history and the results of genetic testing.1–4 This information could be used to vary screening intervals so that women at higher risk are screened more frequently than triennially (as in the PROCAS study; Predicting Risk of Breast Cancer at Screening),3 and women at lower risk are screened less frequently, or not at all. This would direct limited resources towards women more likely to benefit from screening (via early detection of cancers), while reducing the opportunity costs and harms (e.g. overdiagnosis) faced by women less likely to benefit. 5
To be successful, risk-stratified breast screening must be acceptable to the target population. The PROCAS study tested uptake of breast cancer risk assessment and screening behaviour following feedback of risk results to those at high risk, and found that although uptake of 18 monthly screening was high (99%), 6 uptake of the initial risk assessment itself was relatively low, at 37–47%. 3 Women’s perceptions of risk assessment and related interventions have been well researched, in general. Around 50 qualitative studies have been conducted, the majority of which have been in the context of primary prevention, such as lifestyle changes and risk-reducing medication. 7 However, relatively few have had a specific focus on issues relating to risk-stratified screening. Studies that have done so report that women’s attitudes towards breast cancer risk assessment are generally positive,8,9 and Meisel et al. 10 found that women generally consider risk-stratified breast screening to be a good idea, and would be willing to have more frequent screening if at high genetic risk. However, markedly fewer women would be willing to have less frequent screening if at lower risk. 10 Comparable findings are reported by Henneman et al., 9 who found that women endorsed the concept of risk-based breast screening, but had concerns about some women not being invited for any screening. However, the perceived acceptability of not being invited for any breast screening (if women were at very low risk) has not been quantified in the general population. Furthermore, previous studies have focused on risk-stratified screening based solely on genetic testing, not multifactorial algorithms, which are the more likely method of assessment.3,4 Women may have more negative overall attitudes towards this (as it requires the disclosure of additional personal information) or positive attitudes (as it may be perceived as offering greater accuracy). There is some support for both hypotheses from a recent qualitative focus group study. In a sample of 52 women in Australia, participants saw advantages of a multifactorial approach, but had reservations around data security and motivations behind transitioning to this method. 11
There is also varied evidence on women’s preferences for delivery of risk assessment results. Research from the United States suggests that women have mixed preferences for written (vs. face-to-face) information, and from primary care clinicians and genetic counsellors,12,13 whereas participants in a study in Sweden found a consultation with a cancer specialist was most preferable. 8 To our knowledge, this has not been assessed in England, which has a different healthcare system. Unlike the United States, the health service in England carries out a mass screening programme. Given that this programme has become well established over decades, women in England may expect it to be involved in risk-stratified screening. 9 Furthermore, preferences for a delivery method may differ depending on whether the results indicate high or low risk. This has not been tested previously.
The present study addresses these gaps in the literature, using a large-scale population-representative survey of women at or approaching the current age of eligibility for breast screening in England.
Full research aims are stated on Open Science Framework (OSF; https://osf.io/fg7qj/). We aimed to determine:
The extent to which women think it would be a good or bad idea to use a range of risk factors in order to estimate breast cancer risk. The extent to which women would be willing or unwilling to have their risk of breast cancer estimated using multifactorial algorithms, and women’s reasons for being willing or unwilling to have their risk estimated in this way. Women’s preferences for receiving their results if they were found to be (i) at very low risk or (ii) at very high risk of breast cancer. The extent to which women think it would be a good or bad idea to vary the frequency of breast screening based on this form of risk assessment using multifactorial algorithms. The extent to which women would be willing or unwilling to have (i) more frequent screening; (ii) less frequent screening; (iii) no screening based on their risk status.
We also carried out an exploratory analysis of participant characteristics (e.g. age and frequency of worry about breast cancer) potentially associated with (i) willingness to have breast cancer risk assessment, (ii) willingness to have less frequent breast screening (if at very low risk), and acceptability of the National Health Service (NHS) only inviting women at higher risk for screening (if at very low risk).
Methods
Data were collected by a survey company (Kantar TNS) between 25 January and 12 February 2019. Questions for this study were embedded within a larger weekly survey on unrelated topics, administered to participants face-to-face in their homes with the assistance of a computer. Households are approached within small geographic areas selected based on stratified random location sampling, using the Postcode Address File and 2011 Census. Within each area, population representativeness is increased using quotas based on age, gender, employment status and children living within a household. Consenting participants read summary information about breast cancer, screening, risk assessment and risk stratification (Figure 1) immediately prior to completing survey questions. Participants were debriefed on where to find further information on breast cancer and screening from the NHS. Institutional ethical approval was obtained (registration number: 2951/007). The study was pre‐registered on OSF.
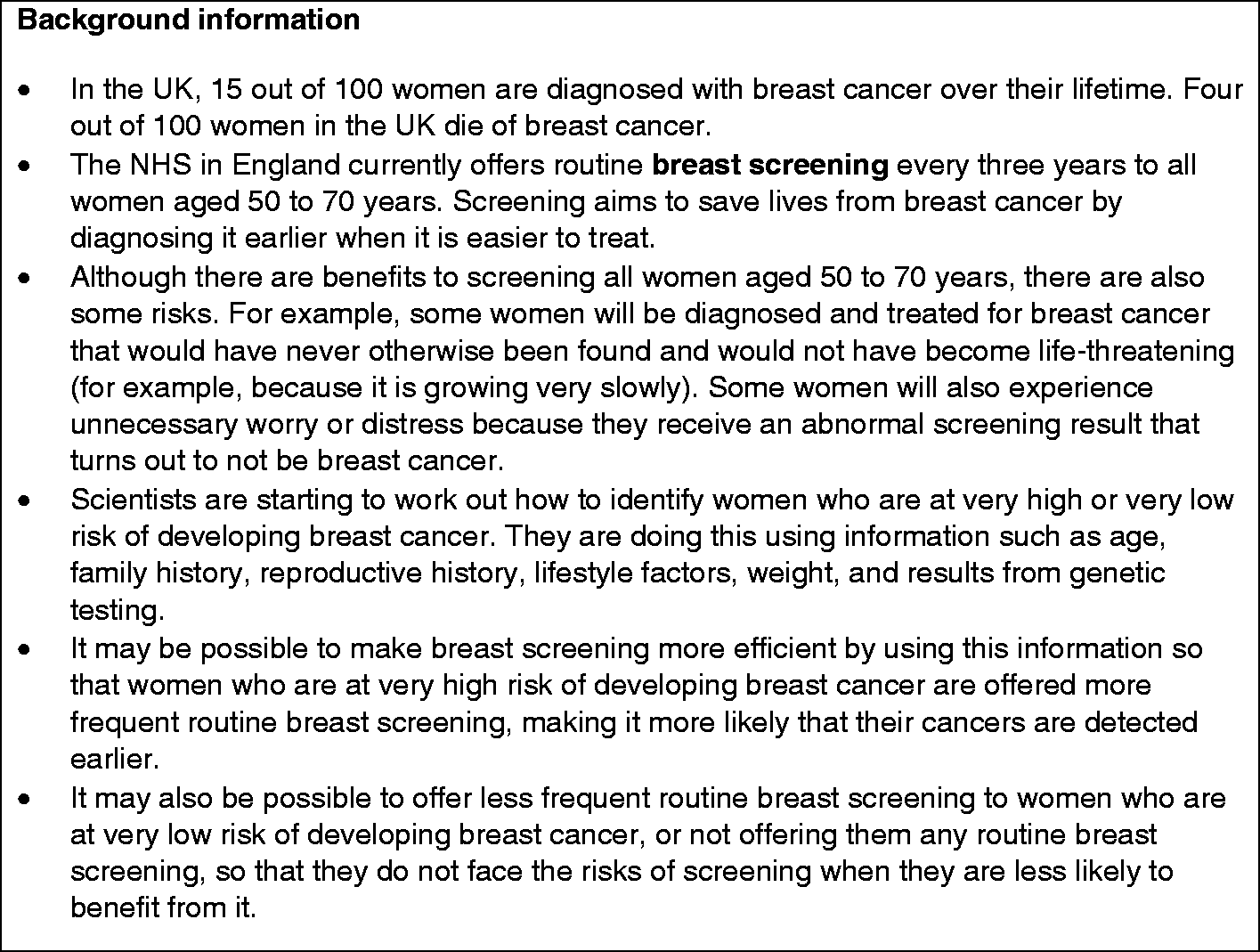
Summary information on breast cancer and screening.
Participants were women in England, aged 40–70 (i.e. approaching or at the age of eligibility for being invited to the existing Breast Screening Programme) 14 and excluded if they did not self-report that they had not been diagnosed with breast cancer.
In addition to questions on age and sex, participants were asked to report their ethnicity, marital status, education (graduate level or above, or other qualifications; the latter category included A Levels, apprenticeships and technical or vocational qualifications) and employment status (working or not working). The latter category included participants who were retired and were either looking or not looking for work, and employment type. Data on National Readership Survey occupational social grade were also collected (Grades A–E; Grades A and E denoted highest (managerial/professional) and lowest (semi-skilled/unskilled) grades, respectively. Grades were determined by the survey company based on factors relating to the occupation of the chief income earner in the household. Data on additional background characteristics were collected as part of the broader survey but are not reported here.
Participants were asked about their perceived susceptibility to breast cancer (relative to other women their age) and how often they worried about getting breast cancer, based on previously used measures.15,16 They were also asked whether any family members had been diagnosed with breast cancer, and whether they had ever had a mammogram (for any reason). If they reported having had a mammogram and were eligible for breast screening based on their age (i.e. were aged 47–70), they were asked if this had been part of screening.
Participants were asked what they thought ‘of the idea of using information like age, family history, reproductive history, lifestyle factors, weight, and results from genetic testing to identify women who are at very high or very low risk of developing breast cancer’ (‘very bad idea’, ‘bad idea’, ‘good idea’, ‘very good idea’, ‘not sure’, ‘prefer not to say’). Participants were also asked if they would ‘personally be willing to have your risk of breast cancer estimated using this kind of information, if the NHS were to offer it?’ (‘yes, definitely’, ‘yes, probably’, ‘no, probably not’, ‘no, definitely not’, ‘not sure’, ‘prefer not to say’). They were then given a free-text field to state their reasons for being (un-)willing to have breast cancer risk assessment, as applicable. Willing participants were asked (i) how (e.g. ‘face-to-face’, ‘by telephone’) and (ii) from whom (e.g. ‘my General Practitioner (GP)’, ‘a screening practitioner from a hospital’) they would prefer to receive risk assessment results if they were at (i) very low risk and (ii) very high risk.
Participants were asked their thoughts on ‘the idea of varying how often women are invited for breast screening based on them being at very high or very low risk of developing breast cancer’ (responses as before) and whether they would ‘personally be willing to have [their] breast screening invitations …’ (i) more often than every three years if at very high risk and (ii) less often than every three years if at very low risk. Finally, participants were asked whether (if they were at very low risk) it would be acceptable for the NHS Breast Screening Programme to only invite women at higher risk than themselves for breast screening (response options were as above).
The survey was designed with input from two patient representatives. Questions are included on OSF.
Free-text data were coded using content analysis by the survey company once all data were collected, prior to transfer to the research team. Responses were assigned to a category when content was mentioned by at least three participants; category names were derived on the basis of responses rather than a pre-defined coding frame. A subsample of 50 responses was evaluated by a member of the research team (AG) to confirm that codes were appropriate. Descriptive statistics report proportions of participants giving each possible response to questions, and 95% confidence intervals. Exploratory binomial logistic regression models tested whether participant characteristics were associated with three dependent variables (willingness to have breast cancer risk assessment, willingness to have less frequent breast screening and acceptability of the NHS not inviting women for screening, if at low risk) dichotomized into ‘yes, definitely’/‘yes probably’ vs. ‘no, definitely not’/‘no, probably not’/‘not sure’. Independent variables were age (categorized into groups; 40–49, 50–59 vs. 60–70), ethnicity (White British vs. other ethnic groups), marital status (married/living as married, widowed/divorced/separated vs. single), highest level of education (graduate level/above vs. other qualifications/not sure), social grade (grade A or B, grade C1, grade C2 vs. grade D or E), perceived susceptibility to breast cancer (‘a little higher’/‘much higher’, ‘about the same’, ‘not sure’ vs. ‘much lower’/‘a little lower’), frequency of worry about breast cancer (‘often’/‘very often’/‘occasionally’/‘sometimes’, ‘not sure’ vs. ‘never’), family history of breast cancer (‘yes’ vs. ‘no’/‘not sure’) and personal experience of (any) mammography (‘yes’ vs. ‘no’/‘not sure’). Variables were dummy coded and tested for multicollinearity; all variance inflation factors < 10. Bonferroni corrections based on the number of variables in each model were applied to adjust for multiple comparisons. Sensitivity analyses repeated analyses with responses of ‘not sure’ excluded from dependent variables.
Analyses were conducted in SPSS version 25; raw data and syntax files are available on OSF.
Results
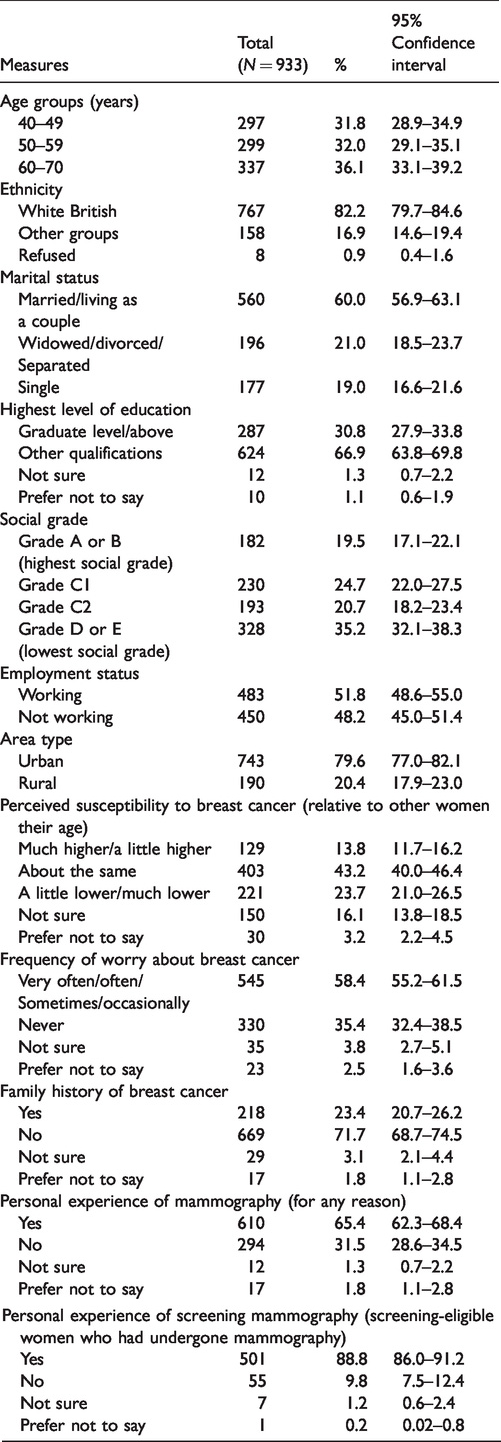
Of the 1135 participants who began the survey, 936 met the inclusion criteria and 3 were excluded for responding ‘prefer not to say’ for all questions. Mean age was 54.9 years (standard deviation: 9.3). Demographic characteristics and responses to questions on breast cancer and screening experience are shown in Table 1. Kantar TNS do not collect information on numbers of people approached for the omnibus survey so we are unable to report a true response rate.
Sample characteristics.
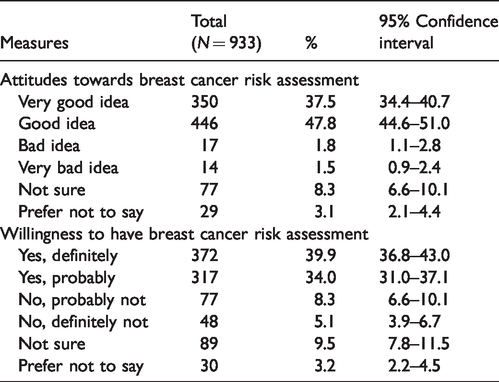
Proportions of participants in each response category for questions on breast cancer risk assessment are shown in Table 2. A large majority considered it a good idea (85%), and stated they would definitely/probably take up an offer (74%). The most common reasons for being willing were labelled ‘(early) detection/(early) treatment’ (11%), ‘family history’ (9%) and ‘so you know/would want to know’ (8%). The three most common reasons for being unwilling were ‘too much of a worry/I wouldn’t want to worry’ (14%), ‘I would rather not know’ (14%) and ‘I have already been tested/I already know my risk’ (7%). All categories of reasons for being (un-)willing are presented in the online Appendix.
Attitudes towards and willingness to have breast cancer risk assessment.
Preferences for methods of delivering risk assessment results are given in Table 3. Face-to-face communication was preferred for delivering assessment results on very high-risk status by most participants (78%), followed by letters/emails (12%). The most commonly preferred people to deliver these results were GPs (45%) or breast cancer specialists (38%). Where assessment results indicated very low risk, letters/emails were the most commonly preferred method of delivery (42%), followed by face-to-face communication (37%). GPs (40%) and nurses at GP surgeries (19%) were the most commonly preferred people to deliver this result.
Preferred methods of receiving risk assessment results by risk status.
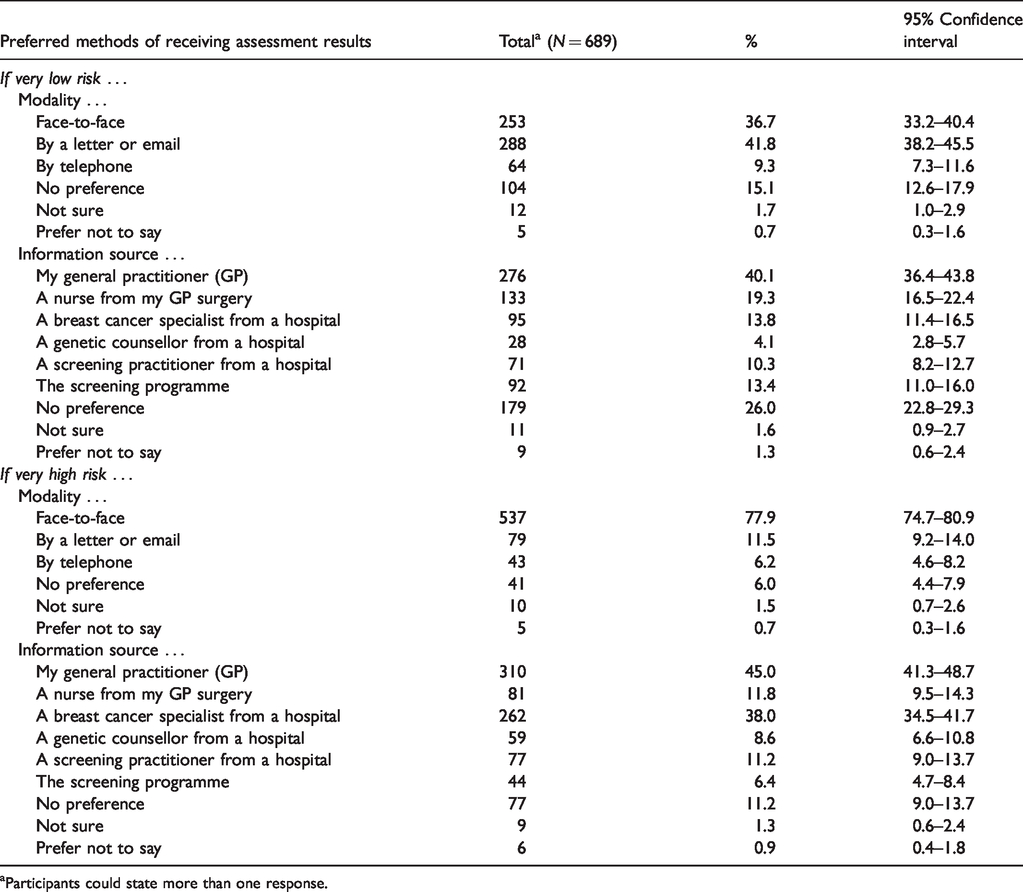
aParticipants could state more than one response.
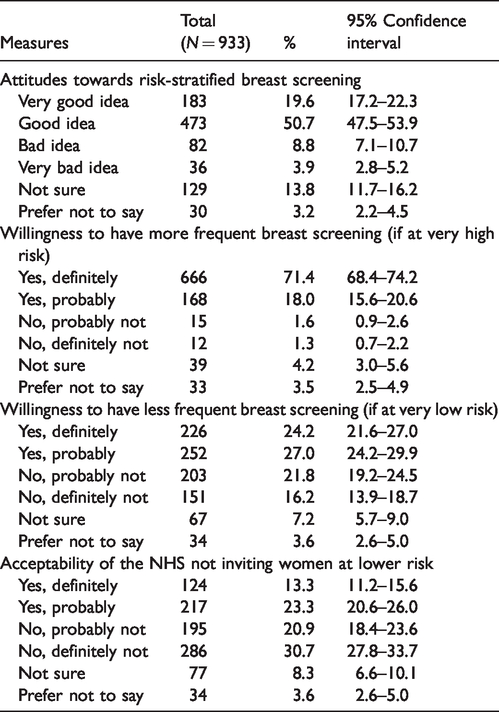
Table 4 shows proportions of participants giving each response to questions about risk-stratified breast screening. Most participants thought it was a good idea (70%). A large majority stated that they would be willing to have more frequent screening if at very high risk (89%), 51% stated that they were willing to have less frequent screening if at very low risk and 37% would find it acceptable if the NHS did not invite women at very low risk.
Attitudes towards and willingness to have risk-stratified breast screening.
In the models testing factors potentially associated with dependent variables of interest, there was only weak evidence against the null hypothesis for all but one included variable after adjusting for multiple comparisons. For worry about breast cancer, those who ever worried were more likely (odds ratio (OR): 1.89; p = 0.031) and those who were not sure were less likely (OR: 0.27; p = 0.019) to be willing to have risk assessment compared with participants who never worried about breast cancer (overall p = 0.002; adjusted α = 0.0056; next smallest p value = 0.013). This possible association was not observed in the sensitivity analysis (excluding ‘not sure’ responses from dependent variables; p = 0.022), reducing confidence in this finding. Sensitivity analysis results were not otherwise appreciably different from the main results. Full results of all models are reported in the online Appendix.
Discussion
This study found that the vast majority of participants (85%) had positive attitudes towards breast cancer risk assessment based on multiple risk factors including genetic factors, a finding consistent with previous studies in which similarly large majorities endorsed other forms of risk assessment for ovarian and breast cancer17,18 and a range of female cancers that also included cervical and endometrial cancer. 19 Similar findings to those of Wegwarth et al. 19 were also observed for the most common reasons for favouring risk assessment, which often centred on early detection/treatment, family history and wanting to know personal risk. This provides some evidence that breast cancer risk assessment would be received favourably if offered to the general population. However, it is notable that uptake in the PROCAS study was 37–47%, based on a real offer of one form of breast cancer risk assessment, suggesting that caution may be needed when drawing implications from our study about likely uptake rates. 3 Our study found that among the 15% who were unwilling to have risk assessment themselves, reasons given most frequently related to worry and preferring not to know. These may represent the predominant barriers that require mitigating in order to maximize uptake among those disinclined to undergo risk assessment. In addition, there may be other important barriers among those with positive attitudes that prevent them from participating when faced with a real offer.
This large-scale quantitative study adds to previous research, comprised mainly of qualitative studies with relatively small sample sizes, or population-based surveys carried out in other countries where healthcare systems and public attitudes may differ. This study also distinguished between levels of risk when assessing preferences for how assessment results would be relayed to participants. Previous results from Sweden showed that a consultation was the most popular method of receiving risk assessment results. 8 However, this study found that letters and emails were the most commonly preferred method for results of very low-risk status, but face-to-face communication was preferred for results of very high risk, indicating that more personal follow-up would be preferred if results have more significant health implications. In addition, GPs and practice nurses were the most commonly preferred healthcare professionals for providing results, although hospital-based breast cancer specialists were preferred almost as often as GPs for delivering results of very high-risk status. The Breast Screening Programme itself was preferred only rarely. In England, primary care only has limited involvement with breast screening, and there would be significant challenges in developing an organizational model for a large-scale breast cancer risk assessment and feedback programme in which primary care took a more prominent role, given its finite capacity, especially if tailored around women’s preferences for face-to-face feedback. However, these findings suggest that this would be perceived positively by participants. Alternatives to primary care include family history clinics, which are run by specialists in hereditary disease who can offer risk assessment, counselling and referral for further investigation. However, participants were not asked to state their preferences for these as they were less likely to be familiar to them.
As found by Meisel et al., 10 most women (70%) stated that risk-stratified screening was a good idea. This was somewhat lower than the equivalent percentage for risk assessment. In addition, participants’ reasons for being willing to have a risk assessment indicated that assessment was perceived as having a wide range of advantages unrelated to risk-stratified screening. An overwhelming majority of participants (89%) were willing to have more frequent screening if they were at very high risk, which was consistent with both hypothetical intentions and actual behaviour in previous studies.3,10 Only around a third of women (37%) stated that not being invited for any screening would be acceptable if at very low risk. Although somewhat lower than the 51% of women who were willing to accept less frequent screening, it might be considered encouraging that as many as one in three women would be willing to forego any screening at all (if at very low risk). However, it is notable that 31% of participants stated they would ‘definitely not’ accept no screening, providing an indication that any resistance would be likely to be intense (as well as widespread) if it were adopted as screening policy.
This study has limitations. We aimed to make information on the multifactorial nature of risk assessment clear and prominent (e.g. by restating it within survey questions), but we did not test participants’ knowledge of this element directly, meaning that we cannot confirm that participants factored it into their responses. Similarly, practical constraints on the amount of information that participants could be expected to absorb meant that the risk labels of ‘very low’ and ‘very high’ were left open to interpretation, and few details were provided on some complicated concepts (e.g. overdiagnosis). Participants may have responded differently if they had received and understood more information on this or other topics.20,21 Responses were also elicited in a hypothetical context, and may have differed following a real invitation. As previously noted, uptake was lower in the PROCAS study. 3 Finally, it is possible that associations with acceptability were missed in the exploratory analyses due to small numbers. For example, we found some evidence of a plausible association in which women who worried about breast cancer were more likely to be willing to have risk assessment than women who did not worry, but this was not supported in other models or sensitivity analyses. In addition, older women (aged 60–70) may have been less likely to be willing to have risk assessment than women aged 40–50. However, confidence intervals were often wide, and most p values provided only weak evidence against the null hypothesis after adjusting for multiple comparisons.
This study indicates several areas for further research. We elicited attitudes relating to risk assessment and screening for breast cancer only; these may differ for other types of cancer. A previous online survey found that 72% of women wanted to know their 10-year risk of breast cancer vs. only 65% for endometrial cancer, 19 and qualitative findings suggest that some women may be more accepting of longer intervals for cervical than breast screening. 11 This could be tested in future studies. We also assessed perceptions of one type of risk assessment (multifactorial). Future studies could test for differences in perceptions based on the type of risk assessment described. For example, participants could be allocated at random to receive information on either multifactorial or genetics-only risk assessment, and compared on outcomes such as willingness to take up a hypothetical invitation.
Conclusion
This study reports a number of findings relevant to the development of risk-stratified breast screening. Encouragingly, women were generally in favour of risk assessment and (more frequent) risk-stratified screening. However, it may be necessary to address the most common barriers to risk assessment among unwilling participants in order to increase uptake. These include worry and preferring not to know risk status. Several findings may be relevant guides to implementing large-scale risk assessment and risk-stratified screening: Letters/emails were most commonly preferred methods for receiving results of very low-risk status, whereas face-to-face communication was preferred for results of very high-risk status. GPs were the preferred sources of information relating to risk status. However, participants were relatively unwilling to accept less frequent and especially no breast screening following assessment results of very low-risk status. Future research can be used to better understand and mitigate this resistance.
Supplemental Material
MSC883662 Supplemetal Material - Supplemental material for Attitudes towards risk-stratified breast cancer screening among women in England: A cross-sectional survey
Supplemental material, MSC883662 Supplemetal Material for Attitudes towards risk-stratified breast cancer screening among women in England: A cross-sectional survey by Alex Ghanouni, Saskia C Sanderson, Nora Pashayan, Cristina Renzi, Christian von Wagner and Jo Waller in Journal of Medical Screening
Footnotes
Authors’ note
Cancer Research UK was not involved in the design of this study; the collection, analysis or interpretation of the results; in the writing of the manuscript or in the decision to submit for publication.
Jo Waller is now affiliated with School of Cancer & Pharmaceutical Sciences, King's College London, London, UK.
Acknowledgement
We are grateful to Beverley Chipp and Mary Kaye for their contributions towards the design of the survey.
Contributors
AG, SCS, NP, CR and JW conceived and designed the study. AG analysed the data. AG, SCS, NP, CR and JW participated in the interpretation of results. AG, SCS, NP, CR and JW drafted the manuscript, participated in critical revision and approved the final version.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a programme grant from Cancer Research UK awarded to Prof Jane Wardle [C1418/A14134]. Dr Jo Waller is supported by a Career Development Fellowship from Cancer Research UK [C7492/A17219].
Patient consent
Obtained.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.