
Abstract
Over the last few years, there has been growing international concern about the risk of overdiagnosis in breast screening and about how to communicate this to women. There has also been an increasing policy drive to provide people with information to enable them to make an informed choice about screening. In response to this, a novel approach to developing the information about cancer screening has been adopted in England. This approach has integrated the perspectives of people eligible for screening, and experts in public engagement, informed choice, and communicating risk, as well as experts in screening. New information based on this approach has been provided to women invited for breast screening from September 2013. The new information explicitly sets out the choice to be made, and provides much more detail than previous information about overdiagnosis, the balance of benefits and harms, and the scientific uncertainties. The novel approach has also been adopted to develop new information for the bowel and cervical screening programmes in England, and could provide a model for communicating about cancer screening in other countries.
Background
Whether the benefits of cancer screening outweigh the harms has been the subject of vigorous debate over the last few years. 1 Central to the controversy has been the emerging recognition of overdiagnosis – the diagnosis of conditions that would never otherwise have become clinically apparent – as a key harm of screening. 2
The balance of benefits and harms of breast cancer screening, in particular, has been keenly disputed.3,4 The English Department of Health responded to this debate by commissioning an independent panel to review the effectiveness of breast screening. Published in October 2012, the Independent Breast Screening Review concluded that screening reduced the risk of breast cancer death by 20% (95% confidence interval 11% to 27%) and that the UK’s NHS breast screening programmes, which offer three-yearly mammograms from age 50 to 70, conferred overall benefit. 5 However, the panel also estimated that for every woman whose death from breast cancer was prevented, about three women would be overdiagnosed, although there was more statistical uncertainty around this figure than the estimates of benefit.
The Independent Breast Screening Review recommended that clear information about the benefits and harms should be given to women to enable them to make an informed choice. 5 Alongside the review, a novel approach to information for the public about cancer screening was established. While the NHS Cancer Screening Programmes had long aspired to offer the public informed choice, 6 the information used previously had been widely criticized for exaggerating the benefits and underplaying the harms and thereby encouraging attendance.4,7,8 Breast screening information in other countries also leans towards promoting high uptake, rather than setting out the benefits and harms clearly.9,10
Challenges to communicating the benefits and harms of cancer screening
The public overestimates the benefits of screening, believing that ‘more is better’ when it comes to medical tests. 11 Three-quarters of respondents to a US survey said they would rather have a total body computed tomography scan than $1000 in cash. 12 The benefits of breast screening, in particular, tend to be overestimated by the public.13,14 Nearly half of women overestimate the benefits of breast screening about ten-fold, according to a large European study. 14 Strongly affirmative messages about screening can also come from charities and politicians.15,16
Information for the public about cancer screening has to convey difficult concepts, and tackle widely-held misunderstandings. For example, 45% women in a UK study believed that breast screening can prevent cancer developing. 17 Overdiagnosis is challenging to explain, 18 because it is currently not possible to identify whether an individual patient has been overdiagnosed, and the problem can only be described at the population level.18,19 Ductal carcinoma in situ is also a difficult concept to explain. 20 The National Cancer Institute recently recommended that ductal carcinoma in situ be relabelled an ‘indolent lesion of epithelial origin’, so as to lose ‘cancer’ or ‘carcinoma’ from the name, and reduce the chance of people thinking that these lesions are always fatal. 21 Presenting estimates of benefits and harms 22 and statistical uncertainty 23 in a way that is meaningful to the public needs to take account of population levels of literacy and numeracy. Among UK adults, one in six has literacy levels and one in four numeracy levels below those expected of an 11 year old. 24
A new approach to communicating about cancer screening
One alternative to encouraging attendance when people are invited for screening is to provide data about benefits and harms, and to let people make their choice. This may appear to be a rational approach, however, for many people it may be burdensome to analyze the data. People may prefer to rely on others, including health professionals whom they trust, to process the complex data about benefits and harms on their behalf. It may also be disconcerting to be asked to ‘take or leave’ a screening programme that the government, on the advice of experts, has decided to fund. Equally, there are concerns that encouraging individuals to carry out a detailed analysis of their decision might not lead to good choices; indeed it might disrupt the usual way that people make decisions about their health that fits with their values and social context. 25
The novel approach in England to information for people invited for cancer screening involves each eligible person receiving a letter of invitation from the NHS. This system sanctions screening, and may be seen as a recommendation in itself. Alongside the letter, people receive a leaflet with balanced information about benefits and harms, with encouragement to assess the offer of screening. The leaflet makes it clear that that not taking up the offer may be a reasonable choice.
The new information was developed at arm’s length from the NHS Cancer Screening Programme, and seeks neither to encourage screening nor to ask people to make decisions without guidance. This approach was based on a way of communicating about screening called ‘consider an offer’. 26 The approach was developed through a public consultation. 27 A draft of the approach was developed, drawing on existing evidence and guidance on communicating with the public about health issues.28–35 This draft set out a number of guiding principles, and a process involving synthesis of the evidence based on benefits and harms of the screening programme and the patient experience, and rigorous public and expert involvement. We circulated this widely to the public, charities, and relevant professionals, and about 1000 members of the public and more than 50 people with a professional interest in the subject gave input through face-to-face discussions and written comments.
Developing new information about the NHS Breast Screening Programme
The four-step process to develop the new information about the NHS Breast Screening Programme was overseen by the advisory committee on information about cancer screening. Experts in screening worked alongside experts in informed choice and communicating with the public, including risk communication, and with representatives of users of screening information.
36
The process included
gaining initial input from women through a Citizens’ Jury gaining input from professional experts in screening, in public engagement, informed choice and communicating risk gaining input from women on draft information, through cognitive testing integrating the input from women and professional experts with final checking informed by comments from the advisory committee.
Gaining the initial input from women: A Citizens’ Jury
Key recommendations of the Citizens’ Jury for information about breast screening.
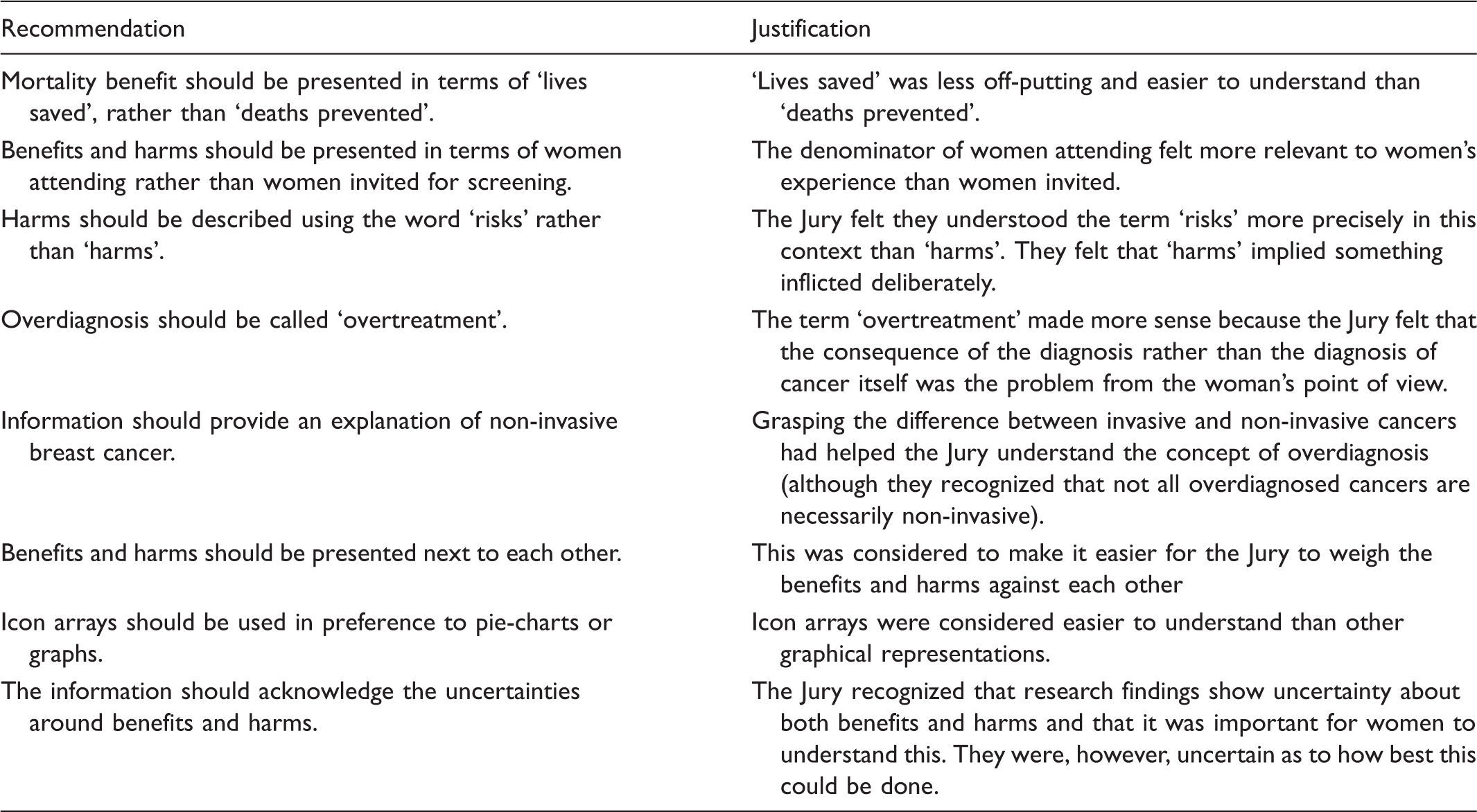
Gaining the input from professional experts
Throughout the process of developing the new information, input from experts in screening was sought to ensure accuracy and engagement from those delivering the service. There were several key areas of debate. The screening experts argued for more detail and scientific precision. Some criticized attempts to display the data using infographics, because they implied scientific certainty, although experts in risk communication supported their use. The most extreme view was that the leaflet should set out the full range of possibilities: that the reduction in risk of breast cancer death associated with breast screening could be as great as 27% and as small as 11%, and that the risk of overdiagnosis could be as great as 50% and as small as 0%. Some experts objected to the term ‘overtreatment’, on the grounds that it implied that it is possible to tell which women are overtreated and that health professionals are at fault for treating overdiagnosed cases.
The leaflet was carefully designed for the target audience and content. The colour palette was chosen to be calm and feminine. The typography and imagery were appropriate for people aged 50–70, and the leaflet was laid out to make it as readable as possible.
Gaining further input from women: Cognitive testing of the draft information
Drafts of the new breast screening invitation letter and leaflet were tested among women of the age group offered breast screening to check how well these were understood. This involved two rounds of one-to-one, face-to-face cognitive interviews, 39 lasting 30–60 minutes each, with 20 women, half who had accepted the offer of screening and half who had not.
A key finding was that women wanted the information to be as simply expressed as possible, and, almost unanimously, with the minimum of numbers. The women preferred a simple graphic showing the main benefit and the main harm against each other to any graphics setting out the quantitative data. They found all attempts to illustrate the size of the benefits and harms confusing; detailed explanation of the numbers either in the text or graphically was considered to hinder rather than help decision-making. Many struggled to understand the concept of overdiagnosis, whether it was described as such, or as ‘overtreatment’. A spaciously laid-out format for the leaflet, without too much text on each page, was considered useful in helping them understand the information. The difference between the letter (the ‘offer’ of screening) and the leaflet (an account of the benefits and harms) was well understood. They felt the information was balanced, would be helpful in making a choice, and conveyed the idea that not having screening might be a reasonable choice.
Integrating the input from the professional experts and women
Tensions between experts and women
Cognitive testing showed that women found numbers overwhelming, contrary to best practice in developing health information, which is to express frequencies using numbers rather than adverbs such as ‘sometimes’ or ‘rarely’. 29 The women also considered the infographics unhelpful. A central challenge was to keep the information simple, and to resist the call from experts for detail and caveats to convey scientific precision. Women found this kind of detail distracting, hindering their understanding. This is consistent with evidence suggesting that people receiving more information do not always make better decisions. 40
Communicating about overdiagnosis
The new information avoids the terms ‘overdiagnosis’ and ‘overtreatment’, instead spelling these concepts out: ‘cancers that would otherwise never have been found or caused harm’ or ‘never become life-threatening’. The leaflet also explains that it is not always possible to tell which breast cancers will become life-threatening, and that research is under way to understand this.
Communicating the balance of benefits and harms
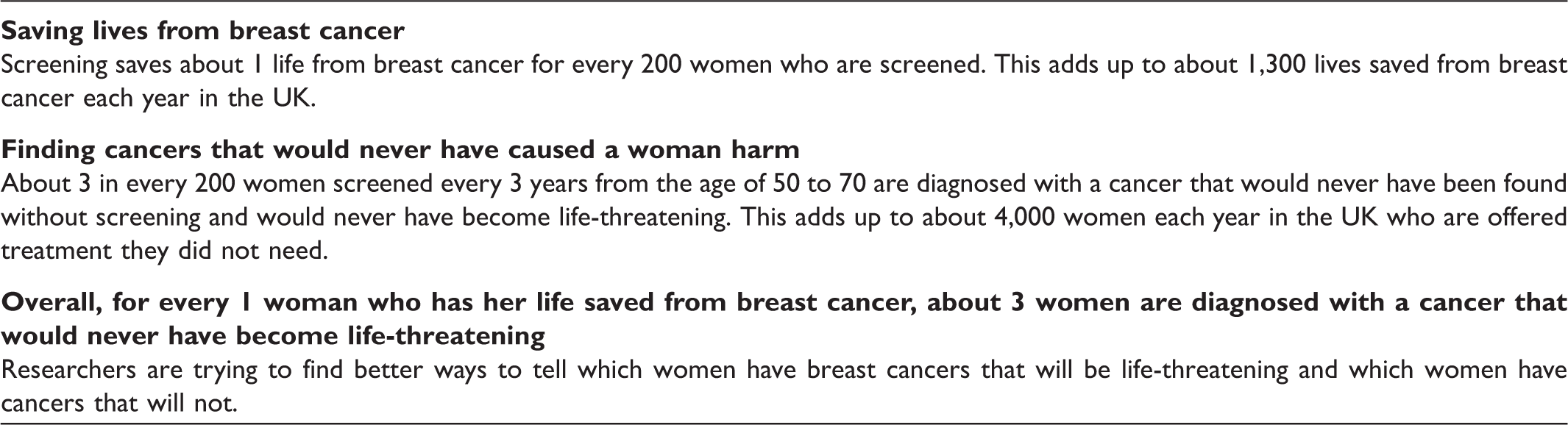
The leaflet provides some quantitative data: the absolute risk reduction of dying of breast cancer and the absolute risk increase of overdiagnosis associated with breast screening, and estimates of number of lives saved and overdiagnoses considered to be due to breast screening in the UK each year (see Box 2 for text). The leaflet provides an image of a woman ‘weighing up’ the main reasons for and against screening (Figure 1), but no graphical representations of the size of the benefits and harms (although these are available online).
Graphic used in the leaflet about breast screening to show the balance of lives saved against risk of overdiagnosis. How the breast screening leaflet sets out the size of the benefits and harms of breast screening.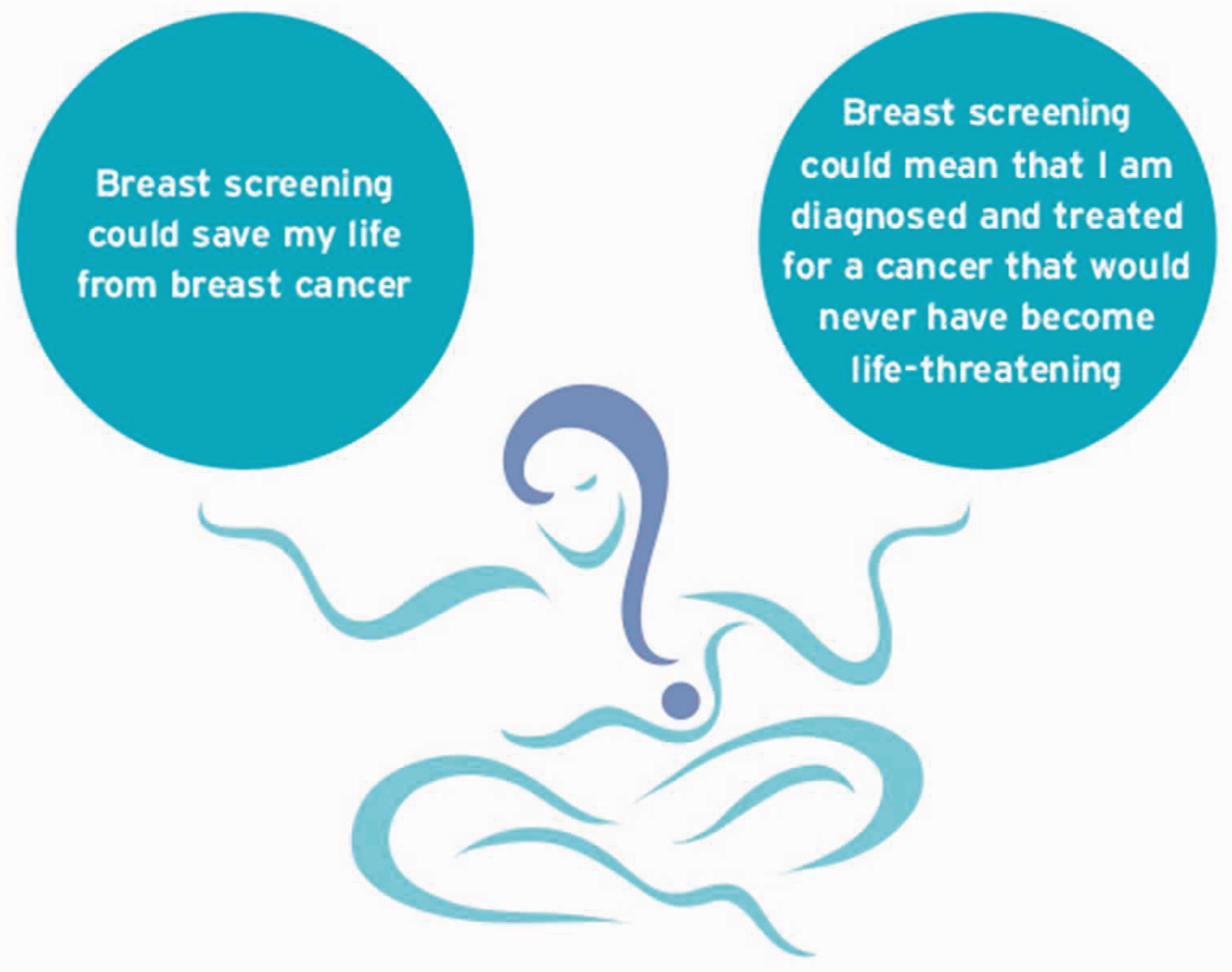
The views of women who took part in cognitive testing about providing illustrations of the size of the benefits and harms overrode the views of the Citizens’ Jury. We felt that cognitive testing represented a scenario closer to that of the experience of a woman receiving the information than the Citizens’ Jury, in which the jurors became very familiar with the concepts and data.
Communicating uncertainty
The leaflet expresses the scientific uncertainties around benefits and harms by saying: ‘There is debate about how many lives are saved by breast screening and how many women are diagnosed with cancer that would never have become life-threatening. The numbers [set out in the leaflet] are the best estimates from a group of experts who have reviewed the evidence’. Recognizing that some women will want more detailed information about the uncertainties, the leaflet provides the address of an online source of information. 41
The future
The new approach in England to communicating about breast cancer screening is an unprecedented move towards offering informed choice in a national cancer screening programme, and could provide a model for communicating about screening for other conditions and in other countries.
The new approach is justified by a number of ethical considerations, but the question of how it affects the quality of women’s decisions and uptake of breast screening now needs to be evaluated. The current policy of judging the performance of cancer screening only on measures of uptake is, arguably, inconsistent with the policy of supporting informed choice. Some features of the ‘consider an offer’ type approach to communication are evident in the stated policies and information materials of other screening programmes, including some prenatal screening programmes and the UK neonatal blood testing programme26,42, but this has not eliminated the problem of some people believing screening tests are so routine (and implicitly good) that they require no thought, or cannot be declined. 42
The messages people pick up from health professionals will not always be congruent with new information, and there is currently no clear mechanism for supporting people to make decisions about cancer screening. Many primary care professionals have neither the capacity nor the training to make a major contribution to supporting informed choice about cancer screening for their patients. Facilitating shared decision-making in the context of cancer screening will need coordinated efforts, training, and structural and cultural change. 33 However, there is scope to build on the work so far. Although currently the same ‘one size fits all’ leaflet is sent to all women eligible for screening across England, digital channels offer potential to tailor it according to specific information needs, for example, according to risk of cancer or level of numeracy or knowledge, and perhaps prior beliefs, or inclinations for or against screening. This could further enable people to consider and make informed choices about offers of screening.
Footnotes
Declaration of conflicting interests
The authors have no conflicts of interest to declare.
Funding
The development of the approach to information about cancer screening and the development of the new breast screening information were funded by NHS Cancer Screening Programmes. However, these were carried out at arm’s length from the NHS Cancer Screening Programmes. The Director of NHS Cancer Screening Programmes reviewed and commented on the manuscript and approved the final version.
Authors’ contributions
LJL Forbes and AJ Ramirez led the drafting of the manuscript and led the development of the novel approach to cancer screening information and the new information about breast screening. A Coulter, J Dewar, R Felton, A Jones, M Michell, M Reed, J Rule, D Spiegelhalter and P Whelehan made a major contribution to the Citizens’ Jury. M Archer, J Cooke, A Coulter, V Entwistle, R Felton, J Kirby, M Reed, J Rule, D Spiegelhalter, D Spika, and R Wilson made a major contribution to the development of the breast screening information. All authors reviewed and commented on the manuscript and approved the final version.
Acknowledgments
The authors thank the women who took part in the Citizens’ Jury and the cognitive testing, members of the Advisory Committee on Information about Cancer Screening and the Advisory Committee on Breast Cancer Screening, for providing expert input into the development of the breast screening invitation letter and leaflet, the Office of Public Management, in particular Deborah Rozansky, Zoe Khor and Sanah Sheikh, for setting up and facilitating the Citizens’ Jury, BMG Research for conducting the cognitive testing of the invitation letter and leaflet, everyone who participated in the consultation, and Elliann Fairbairn and Louise Smith for managing the project.