
Abstract
Objectives
To report the key outcomes of evaluation of the national cervical cancer screening program in Morocco, and describe its organization, status of implementation, performance, and major challenges.
Methods
An evaluation team conducted program manager interviews and screening provider focus group discussions, supervisory visits to primary health and diagnostic centers, and review of published documents. Aggregated performance data collected by the Ministry of Health from the screening and diagnostic centers were analyzed.
Results
Screening is conducted using visual inspection with acetic acid. The program is opportunistic, with no mechanism to identify and invite eligible women. Coverage of the target population was very low (6.6% in 2015 and 7.7% in 2016). Positivity rates were 5.3% and 8.9% in 2015 and 2016 respectively, and varied widely between regions. Detection rate of cervical intraepithelial neoplasia (CIN) 2 or worse in 2016 was very low (0.9/1,000), with more invasive cancers detected than CIN 2/3. Lack of histopathology and treatment facilities at the Cancer Early Detection Centers is a major short-coming, and there is a need for service-provider refresher training. Without a computerized health information system tracking screen positive women, ensuring high treatment compliance and performing regular quality assurance are challenging.
Conclusions
The screening program in Morocco requires better organization, a pragmatic system of inviting the target population, improved compliance to diagnosis, treatment, and follow-up, improved provider training, better quality assurance systems, and an effective health information system with appropriate linkages for monitoring and evaluation.
Keywords
Introduction
Cervical cancer is the second most common cancer in women in Morocco. Age-standardized incidence and mortality rates were estimated in 2012 at 14.3 and 7 per 100,000, respectively, much higher than neighboring Algeria (incidence 8.5, mortality 3.5). 1 It is reported that 65.7% of cervical cancers are diagnosed at advanced stages (II and III), due to limited access to early diagnosis, especially for the women living in hard-to-reach regions. 2
The National Plan for Prevention and Control of Cancer was launched in 2010, 3 and by 2017, the cervical cancer screening program was implemented in 8 of the 12 regions in Morocco. Women aged 30–49 were screened using visual inspection with acetic acid (VIA) by general practitioners, nurses, and midwives at primary health centers (PHCs). 4 VIA-positive women, and those with non-visualization of the squamo-columnar junction (SCJ) at VIA, were referred to the nearest Cancer Early Detection Center (CEDC) for colposcopy. The CEDCs have gynaecologists trained to perform colposcopy, and are equipped to perform loop electrosurgical excision procedure (LEEP). The program guidelines recommend that all colposcopically suspected cervical intraepithelial neoplasias (CIN) should be treated by LEEP, without waiting for histopathological verification (Figure 1). VIA-negative women are advised to repeat screening after three years. The screening, diagnostic procedures, and treatment of cervical pre-cancers are provided free.
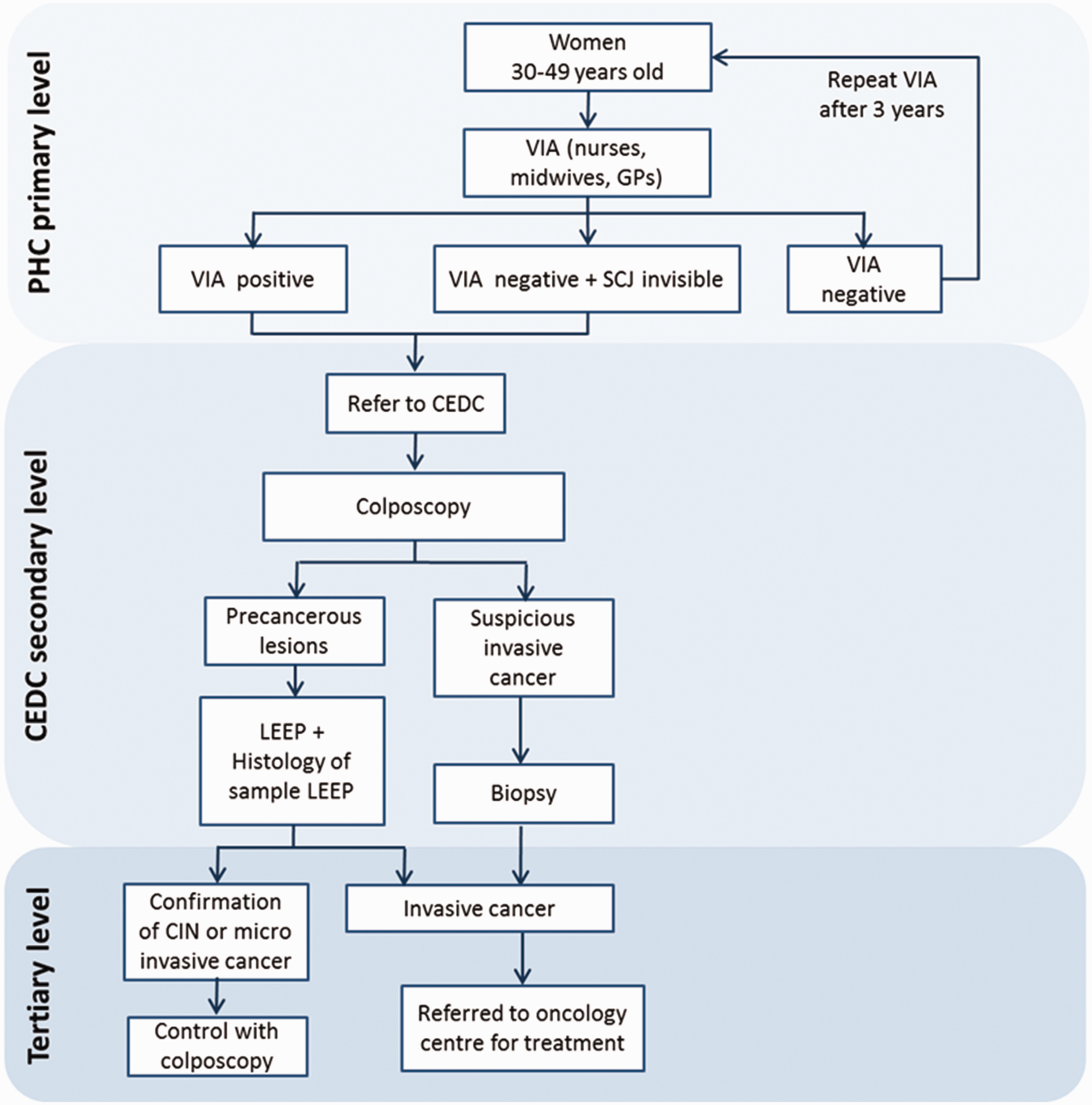
Cervical cancer screening algorithm in the National Cervical Cancer Early Detection Program of Morocco.
There is well-documented policy from the National Government to support the program on a continued basis, with budget allocation from 2010 to 2019. A technical committee is responsible for implementation and monitoring of the program at the national level. In each province, a program focal point reports to the regional focal points, who in turn are guided by the national focal point at the Ministry of Health.
Cervical screening is opportunistic, as there is no mechanism to identify and invite eligible women. Eligible women attending the PHCs for other health issues or accompanying other patients are counselled by the service providers to undergo screening. Sporadic public awareness campaigns to promote cervical cancer screening are conducted by the Ministry of Health in partnership with the local organizations at provincial and regional levels. The Ministry of Health conducts a highly visible campaign to promote breast cancer screening each October, and women attending for breast cancer screening are also counselled to undergo cervical cancer screening, if age-eligible.
The provincial focal point allocates each PHC a target number of women to be screened annually, usually calculated as 30% of estimated total number of eligible women registered with the PHC, with a full cover of the target population within the three-year interval of screening. However, annual targets may vary depending on manpower availability, year of initiation of service, and past performance of the PHC. All screening and diagnostic centers routinely send quarterly aggregated performance data to the national program coordinator at the Ministry of Health.
The Ministry of Health, the Lalla Salma Foundation for Cancer Prevention & Treatment, and the International Agency for Research on Cancer (IARC) jointly initiated a comprehensive evaluation of the screening program in 2017. This paper describes the methodology of evaluation and provides a summary of the program organization, status of implementation, and the evaluation of the outcomes.
Methods
The core evaluation team included the representatives from the Ministry of Health, the Lalla Salma Foundation, and IARC. The team reviewed the program protocols, operational guidelines, and past evaluation reports. In-depth interviews were conducted with the four program managers at national, regional, and provincial levels, and also with the key representatives of the major stakeholders (the Lalla Salma Foundation and the United Nations Populations Fund country office). Four focus group discussions were conducted with 32 service providers involved in screening, diagnostic evaluation, and treatment, to obtain feedback and experience. The Focus Group participants were selected in consultation with the Ministry from those regions implementing cervical cancer screening for more than one year. The team performed supportive supervisory visits to screening centers and CEDCs randomly selected from the regions implementing the program. One province was randomly selected from each region, following which one urban and one rural screening center were randomly selected in that province. The supervisory team used a checklist to collect information on the counselling and registration procedures, screening and referral process, documentation, and record keeping at each screening center. The monthly performance of the center (number of women screened, number testing positive on VIA, number referred) during 2016 was extracted from the registers, and the registration process, diagnosis, treatment, and follow-up procedures and performance during 2016 were documented from each CEDC. The data for the 2015 and 2016 were shared with us by the Ministry of Health. We analyzed the data to estimate selected processes and outcome indicators.
Results
The number of women undergoing VIA at the 13 PHCs included in the supervisory visits ranged from 8 to 871 in 2016, with only four of the 13 centers achieving more than the 90% annual target. The VIA positivity rate ranged from 0% to 34.5% across these PHCs. In the absence of an electronic database, records of the screened women are maintained in screening registers separate from the regular clinic registers. The screening registers were up to date, complete, and well maintained in the majority of the visited centers. From 2016 a unique identity number has been assigned to each screened woman. Without an electronic database, tracking the screen positive women is not efficient. The provincial focal points are responsible for manually cross-checking the monthly list of screen-positive women sent by the PHCs with the list of attendees sent by the CEDCs, to identify non-compliant women. The list of non-attendees is sent to each PHC. The nurses and the midwives at the PHCs are responsible for contacting women non-compliant to colposcopy by telephone, to remind them to attend the CEDCs.
During the supervisory visits to the six randomly selected CEDCs, it was observed that the number of VIA-positive women attending the centers in 2016 ranged from 18 to 444. At some of the CEDCs, the gynaecologists advise Pap smear cytology for all VIA-positive women, and perform colposcopy only if the cytology results are abnormal. The cytology was performed outside the CEDCs, mostly at private clinics, and was not quality assured. The CEDCs were not equipped for cryotherapy treatment. Moreover, the procedure is not included in the national guidelines. The majority of the gynaecologists were not confident in performing LEEP at the CEDCs, and referred the women to the nearest tertiary care hospitals. LEEP was performed in only two of the CEDCs visited, and in 2016 only 17 LEEPs were performed at the two CEDCs combined. The diagnostic centers do not have histopathology facilities. The women are instructed to carry their own biopsy specimens to the laboratory at the local or regional hospital, or to the private clinics.
The total number of women screened in 2015 was 177,011, which comprised 6.6% of the eligible population (N = 2,674,544), and 30.8% of the annual target population in the regions implementing the program (Table 1). Of the women screened, 9453 (5.3%) were VIA-positive. Positivity varied widely across the regions, from 3.0% to 13.8% (Table 2). Among the VIA-positive women, 5412 (57.2%) were known to have undergone colposcopy at the CEDCs. CIN 2 or worse (CIN 2+) lesions were suspected on colposcopy in 661 (12.2%) women, with only 155 women undergoing LEEP, and 71 women having the final diagnosis of invasive cancer (Table 2). No information was available on the number of CIN 2/3 detected on histopathology.
Cervical cancer screening in Morocco: screening coverage by total eligible population and by annual target population in different regions in 2015.
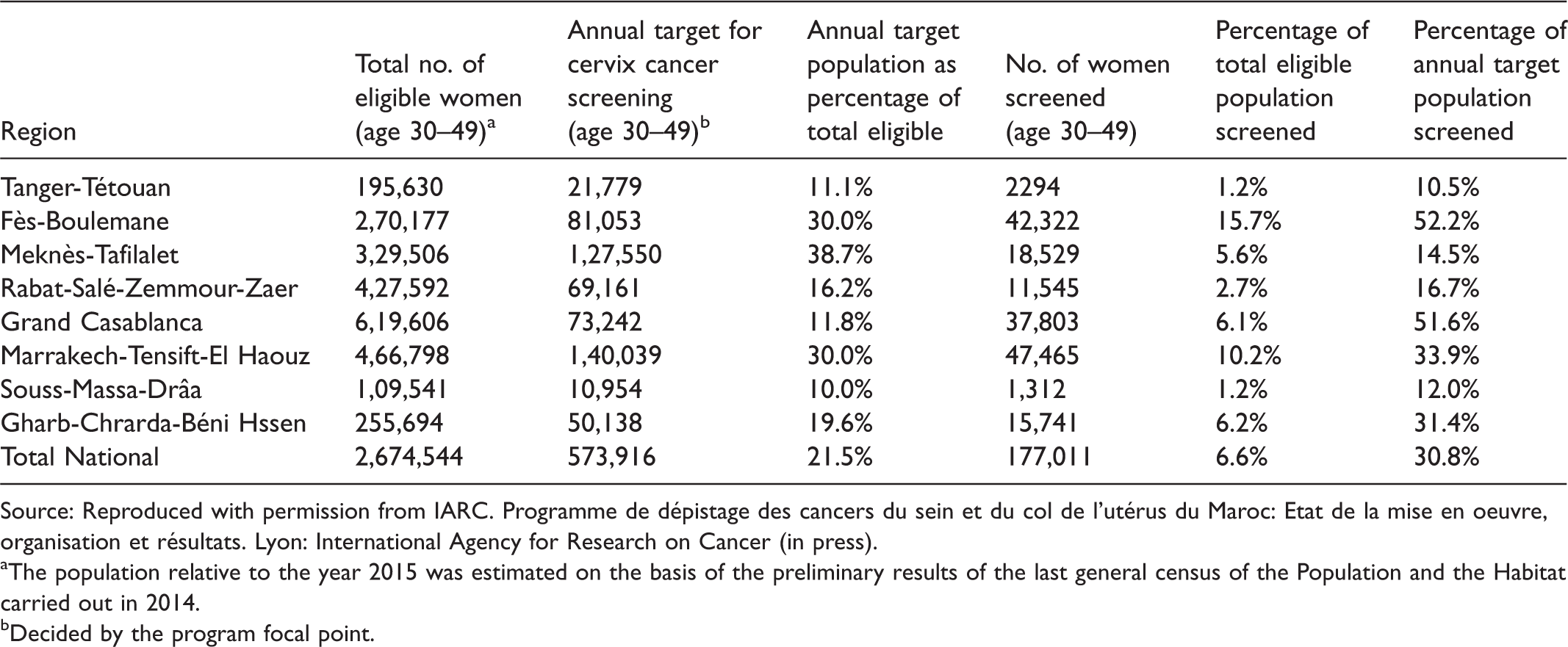
Source: Reproduced with permission from IARC. Programme de dépistage des cancers du sein et du col de l'utérus du Maroc: Etat de la mise en oeuvre, organisation et résultats. Lyon: International Agency for Research on Cancer (in press).
aThe population relative to the year 2015 was estimated on the basis of the preliminary results of the last general census of the Population and the Habitat carried out in 2014.
bDecided by the program focal point.
Cervical cancer screening in Morocco: information on further assessment of the VIA positive women in different regions in 2015.
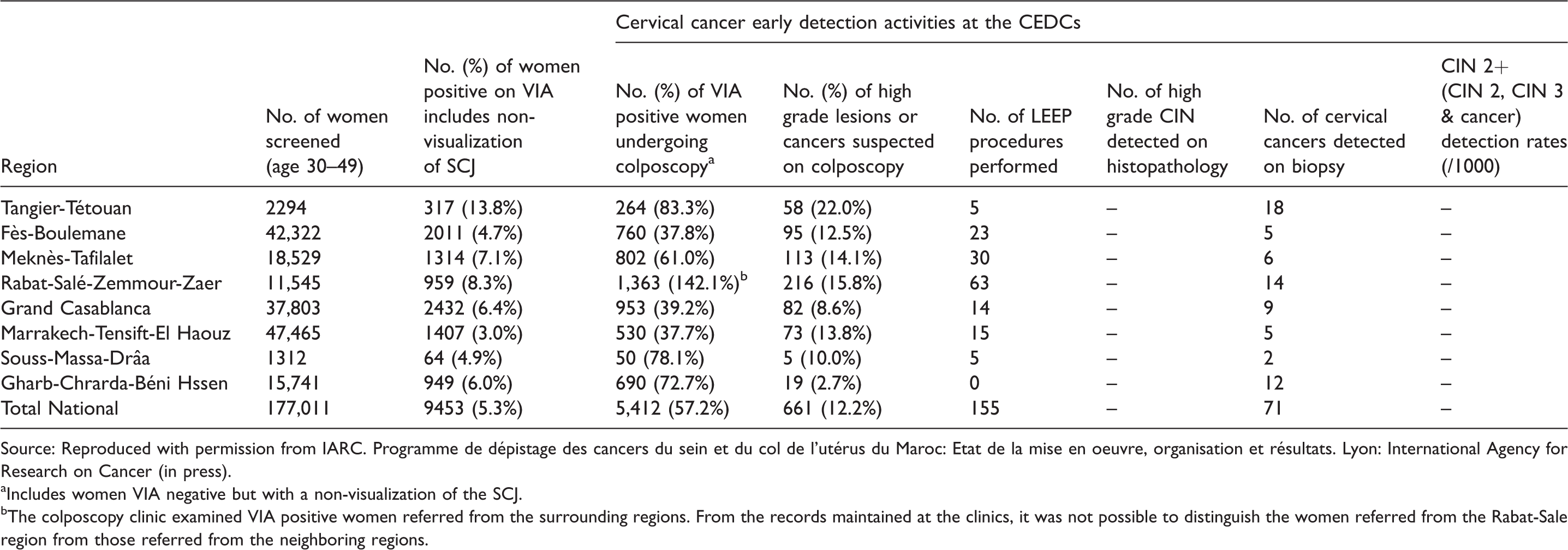
Source: Reproduced with permission from IARC. Programme de dépistage des cancers du sein et du col de l'utérus du Maroc: Etat de la mise en oeuvre, organisation et résultats. Lyon: International Agency for Research on Cancer (in press).
aIncludes women VIA negative but with a non-visualization of the SCJ.
bThe colposcopy clinic examined VIA positive women referred from the surrounding regions. From the records maintained at the clinics, it was not possible to distinguish the women referred from the Rabat-Sale region from those referred from the neighboring regions.
In 2016, 216,137 women were screened by VIA, with target population coverage of 7.7% (N = 2,791,854) (Table 3). The VIA-positivity rate was 8.9%, ranging from 4.5% to 20.2% across the regions (Table 3). Colposcopy was performed on 5399 (28.1%) VIA-positive women at the CEDCs. High grade lesions or cancers were suspected on colposcopy in 10.1% (N = 547), and 110 women underwent LEEP. In 67 cases the histopathology showed CIN 2/3, and 122 cases of invasive cancer were detected at the CEDCs. The detection rate of CIN 2+ in 2016 was 0.9/1000 women screened (Table 4).
Cervical Cancer Screening in Morocco: Screening coverage by total eligible population and by annual target population in different regions in 2016.
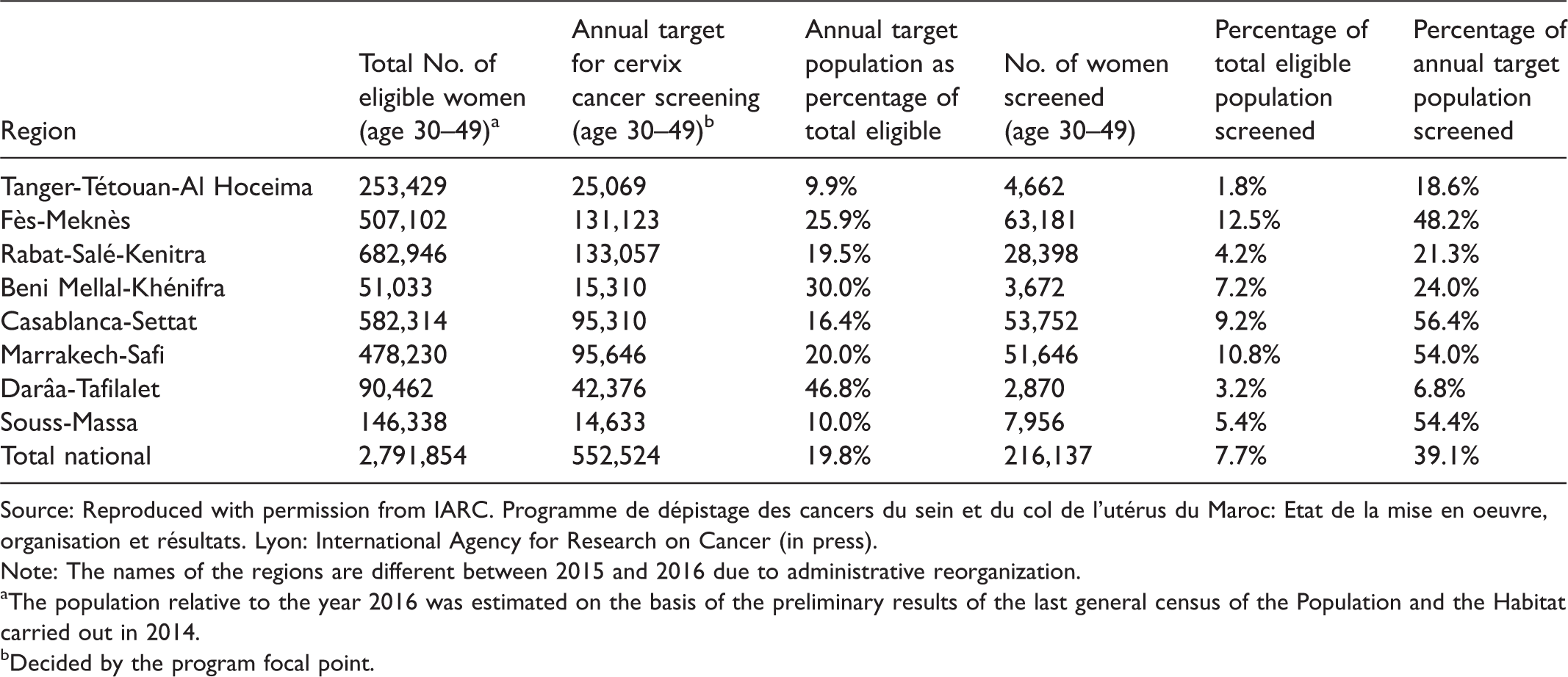
Source: Reproduced with permission from IARC. Programme de dépistage des cancers du sein et du col de l'utérus du Maroc: Etat de la mise en oeuvre, organisation et résultats. Lyon: International Agency for Research on Cancer (in press).
Note: The names of the regions are different between 2015 and 2016 due to administrative reorganization.
aThe population relative to the year 2016 was estimated on the basis of the preliminary results of the last general census of the Population and the Habitat carried out in 2014.
bDecided by the program focal point.
Cervical cancer screening in Morocco: VIA positivity and information on further assessment of the VIA positive women in different regions in 2016.
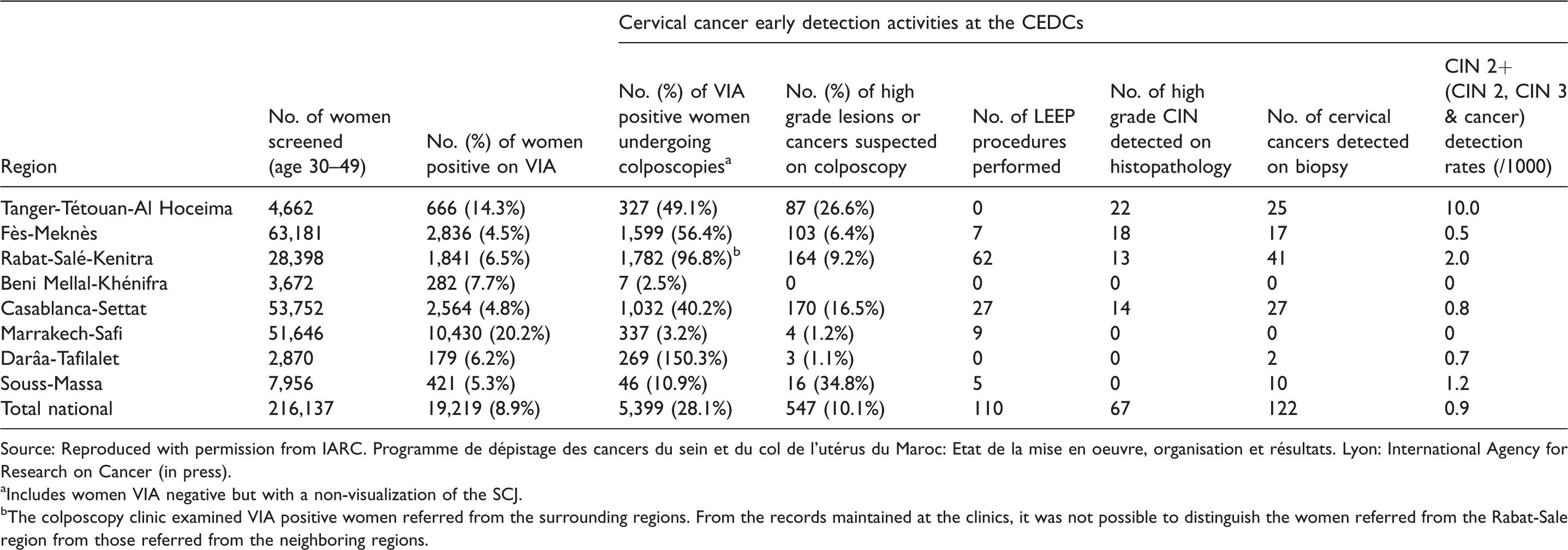
Source: Reproduced with permission from IARC. Programme de dépistage des cancers du sein et du col de l'utérus du Maroc: Etat de la mise en oeuvre, organisation et résultats. Lyon: International Agency for Research on Cancer (in press).
aIncludes women VIA negative but with a non-visualization of the SCJ.
bThe colposcopy clinic examined VIA positive women referred from the surrounding regions. From the records maintained at the clinics, it was not possible to distinguish the women referred from the Rabat-Sale region from those referred from the neighboring regions.
During the focus groups discussions, the knowledge of the health providers about the screening protocols, their acceptance of the screening and treatment recommendations, and their suggestions to improve the quality of services were assessed. The nurses were trained to perform VIA and had good knowledge of the procedure, follow-up advice, and the documentation of results. VIA screening was well accepted by the nurses, and they believed that the services were benefitting the women. Some nurses indicated that they would benefit from orientation training. The gynaecologists had a good understanding of the screening protocol; however, some indicated that they would prefer to advise a Pap smear for VIA negative women in whom SCJ was not visible. In many regions, cryotherapy was not feasible due to the difficulties in procuring refrigerant gas at the CEDCs. The gynaecologists preferred to perform LEEP in the hospitals, rather than the out-patient setting of the CEDCs, and felt that further training in LEEP would improve the quality of the services. They also indicated that not having histopathology facilities at the CEDCs was a problem for the patients, and that many women were lost to follow-up as they did not return with the histopathology reports.
Discussion
The coverage rate of the target population was very low, at 6.6% of the total eligible population in 2015 and 7.7% in 2016. The national screening protocol recommends VIA positivity as a performance indicator to be monitored, and suggests a standard value of 10–13%, based on the results of a pilot study. The observed VIA-positivity rates were significantly lower than the national standard, and varied widely between regions. The detection rate of CIN 2 or worse lesions was very low (0.9/1000), with higher number of invasive cancers detected than CIN 2/3 lesions.
Recognizing the challenges of implementing cytology-based mass screening programs, and based on the evidence for VIA documented by the IARC studies and the World Health Organization recommendation advocating VIA screening for low and middle income countries, Morocco introduced the national cervical cancer screening program based on VIA.5,6 The formal evaluation of the Moroccan program highlighted the inherent deficiencies of VIA in a scaled-up program, and the challenges that a resource limited setting might encounter in implementing cervical cancer screening.
As VIA is a subjective test, it requires adequate training, regular supervision, and periodic reorientation of the providers, to ensure quality. 7 The VIA positivity rate was compared with the national standard of 10–13%. A wide range of VIA-positivity observed across the screening centers, or reported from the different regions, underscores the variability in the test performance, and the need for refresher training of the providers. The detection rate of CIN 2+ lesions (defined as the total number of CIN 2/3 or invasive cancers detected among the total number of eligible women screened in the year) reported for 2016 was very low (0.9/1000), which may be explained by the low sensitivity of VIA, low compliance of the referred VIA-positive women to further assessment, sub-optimal quality of the diagnostic tests, and incomplete data collection. The number of cancers detected was much higher than the number of CIN 2/3, indicating deficiencies in screening and diagnostic evaluations. The national protocol recommended colposcopy for all women in whom the SCJ was not visualized on VIA. Such an approach has questionable benefits, and leads to unnecessary referrals. The inability to detect endocervical lesions is a well-accepted limitation of VIA, and the same limitation applies to colposcopy.
Due to purely opportunistic nature of the program, the screening coverage of the target population in Morocco was very low. Other reasons identified to explain the low coverage include lack of VIA facilities in some of the provinces, low acceptance of screening among the women, non-availability of VIA services on all working days at the PHC, and absence of a communication/awareness creation strategy promoting cervical cancer screening. An effective and robust linkage between screening and treatment is of paramount importance for the program to have the desired impact. 8 The program in Morocco was deficient in this aspect, due to the absence of an efficient mechanism to track the positive women, the lack of cryotherapy facilities at the colposcopy centers, and the limited capacity among the gynaecologists to perform LEEP on an outpatient basis. The colposcopists should treat at least the high-grade lesions suspected on colposcopy, to reduce treatment non-compliance. Due to the difficulties in introducing cryotherapy, thermal ablation, which is safe and as effective as cryotherapy,9,10 should be considered as an alternative ablative treatment. The need for additional visits to CEDCs for diagnosis and treatment is a limiting step, leading to poor compliance of VIA-positive women for further investigations and management. The treatment policy for management of precancerous lesions revolves around LEEP only. Such an approach requires considerable resources, particularly skilled human resources and a more sophisticated equipment infrastructure. It is important to consider the introduction of simple ablative techniques, such as thermal ablation, for the treatment of ectocervical precancerous lesions, while reserving LEEP for larger lesions and lesions involving the endocervix. Such a mixed policy, of using both ablative and excisional methods for the management of CIN, would be more pragmatic and sustainable.
A computerized health information system capturing screening, diagnostic, and treatment activities is an essential component of a well-organized program. 11 Linkage of this system with some form of population database (e.g. population register, electoral roll, unique national identification number, etc.) allows the establishment of a call-recall system, and the linkage between the different levels of service delivery allows tracking of the screen positive women, and those requiring treatment. Introduction of the computerized records system at the CEDCs, and linking that database with the already existing computerized databases of all the oncology centers, will allow estimation of some of the key program indicators, and also allow tracking of the women requiring treatment.
Conclusion
The VIA-based screening program in Morocco needs to be reorganized, with improved provider training, an effective health information system with appropriate linkages, mass media campaign to generate awareness in the community, a pragmatic system of inviting the population, implementation of a single visit approach for the management of precancerous lesions, increasing use of ablative treatments for ectocervical CIN lesions, and a better system of quality assurance, to ensure that the program is effective in reducing the cervical cancer burden, with efficient utilization of the limited resources.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We gratefully acknowledge the support from the Ministry of Health, Government of Morocco, and the Lalla Salma Foundation for Cancer Prevention & Treatment, Morocco.