
Abstract
Objectives
Population-based colorectal (bowel) cancer screening using faecal occult blood tests leads to a reduction in cause-specific mortality. However, in people where the colon is defunctioned, the use of standard faecal occult blood test is not appropriate. The aim of this study was to examine the current trends of clinical practice for colorectal cancer screening in people with defunctioned colons.
Methods
An online survey was performed using SurveyMonkey. All members of the Association of Coloproctology of Great Britain and Ireland were invited by email to participate. Reminders were sent to non-responders and partial responders till six weeks. All responses were included in our analysis.
Results
Of the 206 (34.59%) questionnaires completed, all questions were answered in 110 (55.8%). Among responders, 94 (85.4%) were colorectal consultant surgeons, 72% had worked in their current capacity for more than five years, and 105 (50.9%) had encountered colorectal cancer in defunctioned colons during their career. Some 72.2% of responders stated that a screening test for colorectal cancer in patients with defunctioned colons was currently not offered, or that they did not know whether or not it was offered in their area.
Conclusions
Bowel screening in the United Kingdom is currently not offered to 72.2% of the age appropriate population with defunctioned colons. Among responding colorectal surgeons, 50% had encountered colorectal cancer in such patients. There is considerable variability in clinical practice regarding the optimal age for onset of screening, time interval, and the optimal modality to offer for screening in such cases.
Introduction
Colorectal cancer (CRC) is the fourth most common cause of cancer-related death worldwide,1–5 with around 41,000 new cases a year in the United Kingdom.4–5 It is well established that early CRC is associated with improved survival, and randomized trials have demonstrated that CRC screening can reduce disease specific mortality in the population offered screening.6–8 A range of screening modalities have been investigated with varying acceptability and cost-effectiveness. Currently, in the United Kingdom (UK), bowel cancer screening is performed with the guaiac Faecal Occult blood Test (gFOBT) and recently a change to Faecal Immunochemical Testing (FIT) for hemoglobin as the primary test has been agreed by the UK NHS Bowel Cancer Screening Programmes; however, both FIT- and gFOBT-based screening require faecal samples. In patients where a reasonable length of colon has been defunctioned (i.e. with a defunctioning ileostomy or colostomy), this screening test is not appropriate.
Non-specific inflammation of the colon is a well-described phenomenon following diversion of faecal stream in the segment of colon downstream. The histological changes of diversion colitis include diffuse inflammation, crypt architectural distortion, crypt abscesses or atrophy, and lymphoid follicular hyperplasia.9–11 The incidence of defunctioning colitis is reported to be approximately 70–100%. However, to date there is no evidence that faecal diversion without any coexisting predisposing factor for CRC increases the risk for development of CRC in the segment of colon downstream. The incidence of CRC in defunctioned colons is poorly reported in the literature.
Patients may be left with a defunctioned colon for several reasons, the most common of which is rectal cancer surgery. A, 2013 Dutch study reported that 70% of patients undergoing low anterior resection undergo temporary ileostomies. 12 A contemporary retrospective study reported that one in four temporary ileostomies performed during anterior resections were never closed due to reasons such as anastomotic leak, rectovaginal fistula, and disease progression. 13 Another important group of patients includes those with functional bowel disorders with long term ileostomy or colostomy. The prevalence of patients with defunctioned colons is not well-known, but it is likely that most health care professionals will encounter this clinical situation. The practice of offering screening for CRC in these people is variable and, to date, there are no guidelines which can help in decision making process.
The aim of this study was to examine the current trends of clinical practice for CRC screening in asymptomatic people with defunctioned colons.
Methods
A 10-question survey assessing the current awareness and practice of colorectal surgeons about screening for CRC in people with defunctioned colons was generated (Table 1). All questions were multiple choice, with an option for additional information. The questionnaire also examined the region of the clinical practice and duration of the surgeon’s experience in the relevant capacity. The questionnaire was distributed via SurveyMonkey (www.surveymonkey.com) to members of the Association of Coloproctology of Great Britain and Ireland (ACPGBI) whose email addresses were listed on the ACPGBI website. Reminders were emailed to partial- and non-responders until six weeks had elapsed. Respondent data were de-identified, and all responses were collected anonymously. Descriptive statistical analysis was performed using software within the SurveyMonkey analytics and using Microsoft Excel (Redmond, WA). Institutional review board approval was not obtained for this study, but the study was performed based on the guidelines in the Declaration of Helsinki. All responses were included in analysis.
Questionnaire: colorectal cancer screening in people with defunctioned colons.
Results
Of 596 ACPGBI members invited to participate in the survey, 206 responded (34.5%). Complete responses to all parts of the questionnaire were received from 110 participants, who answered all the relevant questions from the questionnaire. Among the responders, 80.0% were working in England, 9.1% in Scotland, 4.5% in Wales, 3.6% in Ireland, and 2.7% in other parts of the world. Some 85.5% of respondents were consultants, 6.3% were specialty doctors and staff grades, and 72% had worked in their current capacity for more than five years. Experience of CRC in patients with defunctioned colon was reported by 105 participants (see Figure 1).
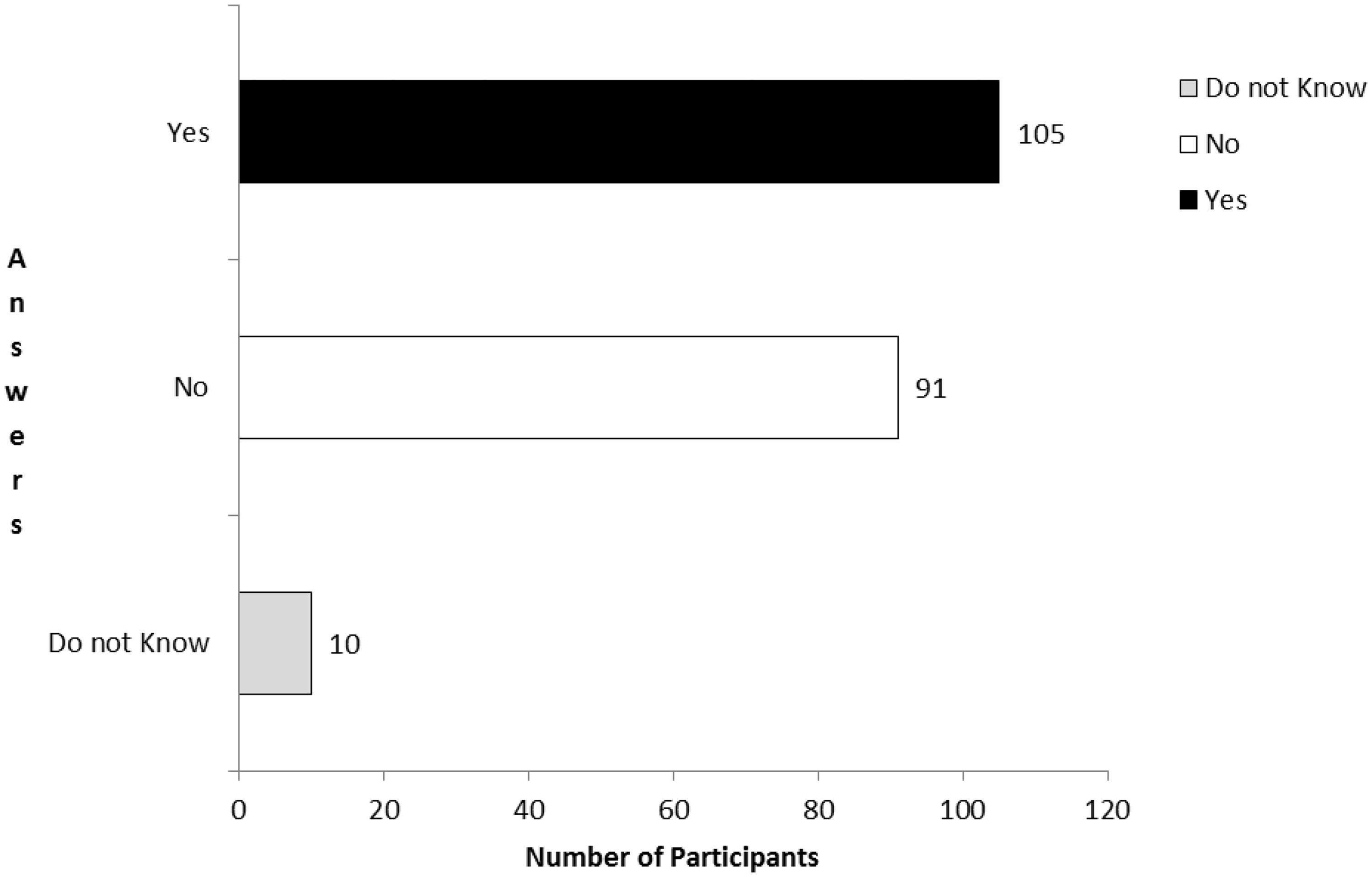
Have you encountered colorectal cancer in defunctioned colons?
Among participants, 31 (28.2%) stated that a screening test for CRC was offered to people within the screening age range with defunctioned colons, 42 (38.8%) offered no screening, and 37 (33.6%) did not know whether it was offered in their area of clinical practice (see Figure 2). There were 54 (49.1%) responders who did not know at what age to offer a screening test, 15 (13%) stated that they would recommend a test in participants aged 50–54, and 14 (12.7%) would offer screening at age 60–64. Among responders 64 (58.2%) stated that they would offer colonoscopy, 24 (22%) would consider flexible sigmoidoscopy, and 21 (19.1%) considered computerized axial tomography (CT) colonography as the test of choice.
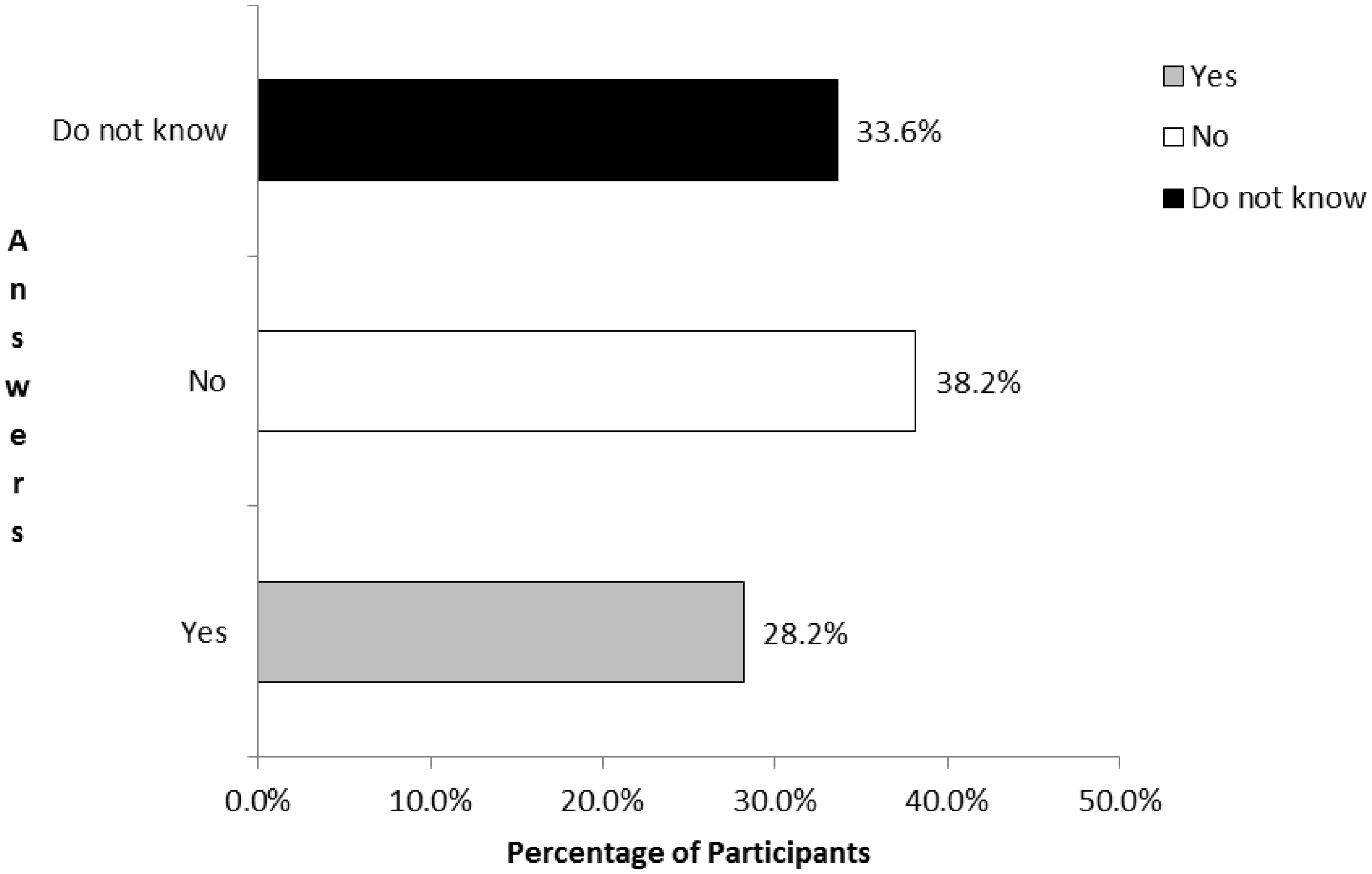
Do you think that a screening test for colorectal cancer in patients/people with defunctioned colons at appropriate age for screening is done in your area or in your clinical practice?
When asked about the screening interval, 41 (37%) responders did not know how often they should offer screening, and 34 (30%) stated that they would offer a screening every five years.
Discussion
This study demonstrates that CRC screening in people with a defunctioned colon is not performed in the majority of cases in the UK. Defunctioning stomas (i.e. defunctioning ileostomy or transverse loop colostomy) are used for a variety of purposes in the management of benign and neoplastic colorectal diseases. Colorectal surgeons and, to a lesser extent, general practitioners, will not infrequently encounter patients with a long term defunctioning stoma with an appreciable length of colon which is not in functional continuity with the gastrointestinal tract. There is; however, no evidence on which to base a decision on whether or not to offer screening, and which test to advise.
To our knowledge, this is the first study to describe the attitudes and clinical practice of colorectal surgeons to bowel cancer screening in a population with defunctioned colons. Most participants in the survey responded that CRC screening in people with defunctioned colon was either not offered, or they did not know if it was offered in their area of clinical practice.
The incidence of CRC in defunctioned colons is poorly reported. In this study 105 respondents reported that they had seen a total of 115 cases of CRC in the defunctioned segment of colon, but on literature review we were unable to find a single case report. To date, there is no evidence to dispute that there is a need for CRC screening in these patients. If it is assumed that the risk of CRC is the same in these subjects as in a normal healthy population, participants with defunctioned colons should be offered CRC screening. As conventional FOBT or FIT testing is clearly inappropriate in these people, colonoscopy, flexible sigmoidoscopy, or CT colonography are the only currently available options. Our data suggest that in the UK the majority of ACPGBI members recommend colonoscopy, with equal numbers suggesting flexible sigmoidoscopy and CT colonography. Modelling studies have suggested that, where the resources are available, colonoscopy is the most effective screening strategy, with the highest life-years gained and CRCs prevented, and the lowest total costs.14,15 As the number of people with defunctioned colons is not very large, it may be reasonable to suggest that colonoscopy is the most appropriate screening test in such cases.
About half of the respondents were unsure about the correct age at which screening should commence in this group. There is variation in the screening age range among the bowel screening programmes in the four countries of UK, which may account for some of difference of opinion about the age of onset of screening. The majority of practitioners were similarly unsure about the correct time interval between screening tests. A biennial time interval was used for gFOBT-based CRC screening in the randomized trials that demonstrated efficacy,6–8 but in the UK Flexible Sigmoidoscopy trial, a single flexible sigmoidoscopy offered between ages 55 and 64 resulted in a decrease in CRC mortality of 31%. 16 Moreover, the latest long term results of UK Flexible Sigmoidoscopy Screening Trial confirm that a single flexible sigmoidoscopy continues to provide substantial protection from CRC diagnosis and death, with protection lasting at least 17 years. 17 However, 30.9% respondents of our study felt that a five yearly interval is reasonable in this group of people with defunctioned colons.
Limitations of this study were that a response could not be obtained from the majority of ACPGBI members, and it was not possible to compare the detailed characteristics of responders with non-responders or partial responders. However, the geographical distribution of responders had the same regional distribution as the total number of ACPGBI members, with 80% from England, 18 and similarly, 85% of responders were working as consultant surgeons, a percentage very close to that among total ACPGBI members. We have therefore inferred that the responders were a representative sample of ACPGBI members.
Conclusion
This study demonstrates that screening for CRC is currently not offered to the majority of people with defunctioned colons, despite 50% of responders having encountered CRC in such patients. There is a considerable variability in opinion regarding the optimal age at which to commence screening, the time interval between screening episodes, and the optimal modality to offer for screening in such cases. There is an urgent need to clearly define the extent of this important clinical problem, and to provide guidance for how these patients should be managed.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.