
Abstract
Objective
Age screening and preventive medication for future myocardial infarction and stroke has been previously described. We aimed to ascertain whether different age cut-offs are needed for males and females.
Methods
We determined five parameters for each sex according to age cut-off: detection rate (sensitivity), false-positive rate, proportion of the population eligible for treatment with a polypill, proportion who benefit from taking a polypill (simvastatin 20 mg, losartan 25 mg, hydrochlorothiazide 12.5 mg, amlodipine 2.5 mg), and among these, years of life gained without a first myocardial infarction or stroke.
Results
Approximately one-third benefit, regardless of the age cut-off. For males and females combined, using ages 40 and 80, the detection rates are 98% and 52%, false-positive rates are 51% and 7%, population percentages eligible for treatment are 52% and 7%, and years of life gained without a first myocardial infarction or stroke are 8.4 and 3.6. Using age 50, detection rates are 93% (males) 98% (females), false-positive rates 37% (males) 40% (females), percentage of the population eligible for treatment 38% (males) 41% (females), percentage who benefit 35% (males) 33% (females), and years of life gained without an event 8.5 (males) 7.0 (females). At a given age cut-off, the sex differences are relatively small.
Conclusion
A single age cut-off can be used for both sexes.
Introduction
Age screening for future myocardial infarction (MI) and stroke is effective and simple.1,2 Adding risk factors other than age has little impact on screening performance. 3 The use of an appropriate polypill (statin and three blood pressure lowering drugs at half standard dose) reduces low density lipoprotein cholesterol and blood pressure, and does so to an extent predicted from the independent effects of each polypill component. 4 These reductions have been used to estimate the reduction in MIs and strokes from the results of cohort studies and randomized trials.1,5–7 Such a polypill, taken daily from age 50, would benefit one in three people who would each gain an average of eight years of life without an MI or stroke. 8
In this paper, we investigate the sex-specific screening performance and the sex-specific health benefits of taking a four-component polypill, according to age of starting to take polypill. We also discuss the consequent implementation issues.
Methods
Standard life table analysis was used as described in Wald and Morris, 8 based on the UK population in 2013, to determine five sex-specific parameters, according to age of starting polypill preventive treatment: (i) the detection rate (DR) for first MI or stroke (i.e. the proportion of people who have a first MI or stroke at or above an age cut-off), (ii) the false-positive rate (FPR) (i.e. the proportion of all people who never have an MI or stroke at or above an age cut-off), (iii) the proportion of the population eligible for preventive treatment, (iv) the proportion of people among those eligible who benefit from a taking a daily polypill consisting of simvastatin 20 mg, losartan 25 mg, hydrochlorothiazide 12.5 mg, and amlodipine 2.5 mg, and (v) the average years of life gained without a first MI or stroke among those who benefit.
The analysis created a lifespan cohort by applying age and sex-specific 2013 all-cause mortality rates to the cohort of people born in 2013, to obtain the age-specific number of people at risk of an MI or stroke. The analysis then applied age and sex-specific incidences of a first MI, first stroke, and death from causes other than MI and stroke, to pairs of sub-cohorts from age 40, 50, 60, 70, and 80; one sub-cohort in each pair takes the polypill from the specified age, and the other does not. The years without a first MI or stroke were accumulated for each cohort and the results compared between the two. The proportion of people who benefit was determined using the holistic model described by Wald and Morris 8 (i.e. all who would have had a MI or stroke benefit by delaying the time when they would have had an MI or stroke). To determine the DR (sensitivity) for a first MI or stroke, the FPR and the proportions of the population eligible for preventive treatment, a cohort not taking the polypill was followed from birth.
Results
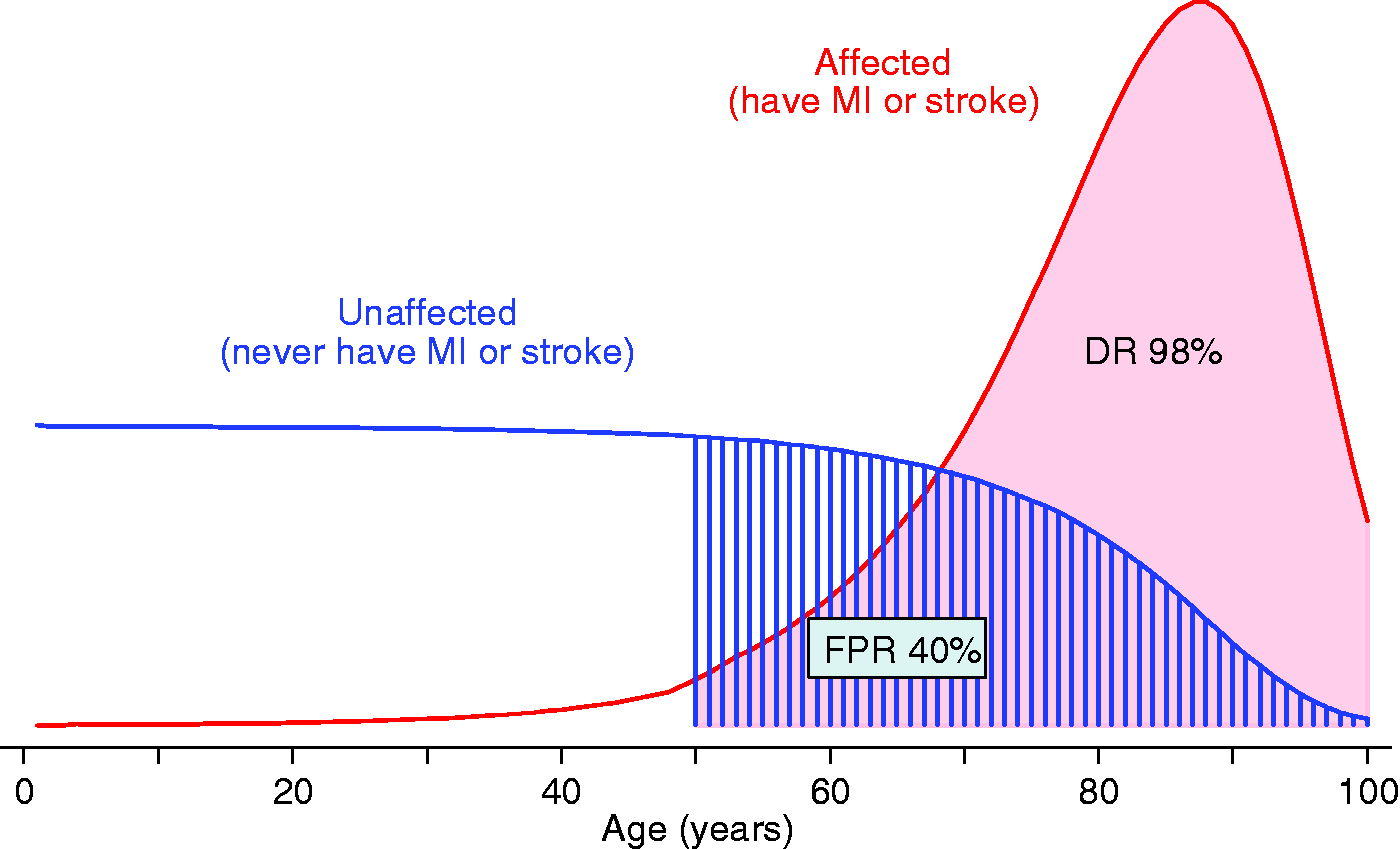
Figure 1 shows, in the absence of preventive treatment, the relative age distribution of a first MI or stroke among males who do (affected) or do not (unaffected) have an MI or stroke at some time in their life. The figure illustrates the use of an age cut-off of 50, showing a DR of 93% and a FPR of 37%. Figure 2 shows the corresponding distributions in females; at an age cut-off of 50, the DR is 98% and the FPR is 40%.
Relative distributions of age in a cohort of British males who (a) have a first myocardial infarction (MI) or stroke, and (b) never have an MI or stroke (unaffected). The detection rate (DR) and false-positive rate (FPR) are shown using an age cut-off of 50. Relative distributions of age in a cohort of British females who (a) have a first myocardial (MI) infarction or stroke, and (b) never have an MI or stroke (unaffected). The detection rate (DR) and false-positive rate (FPR) are shown using an age cut-off of 50.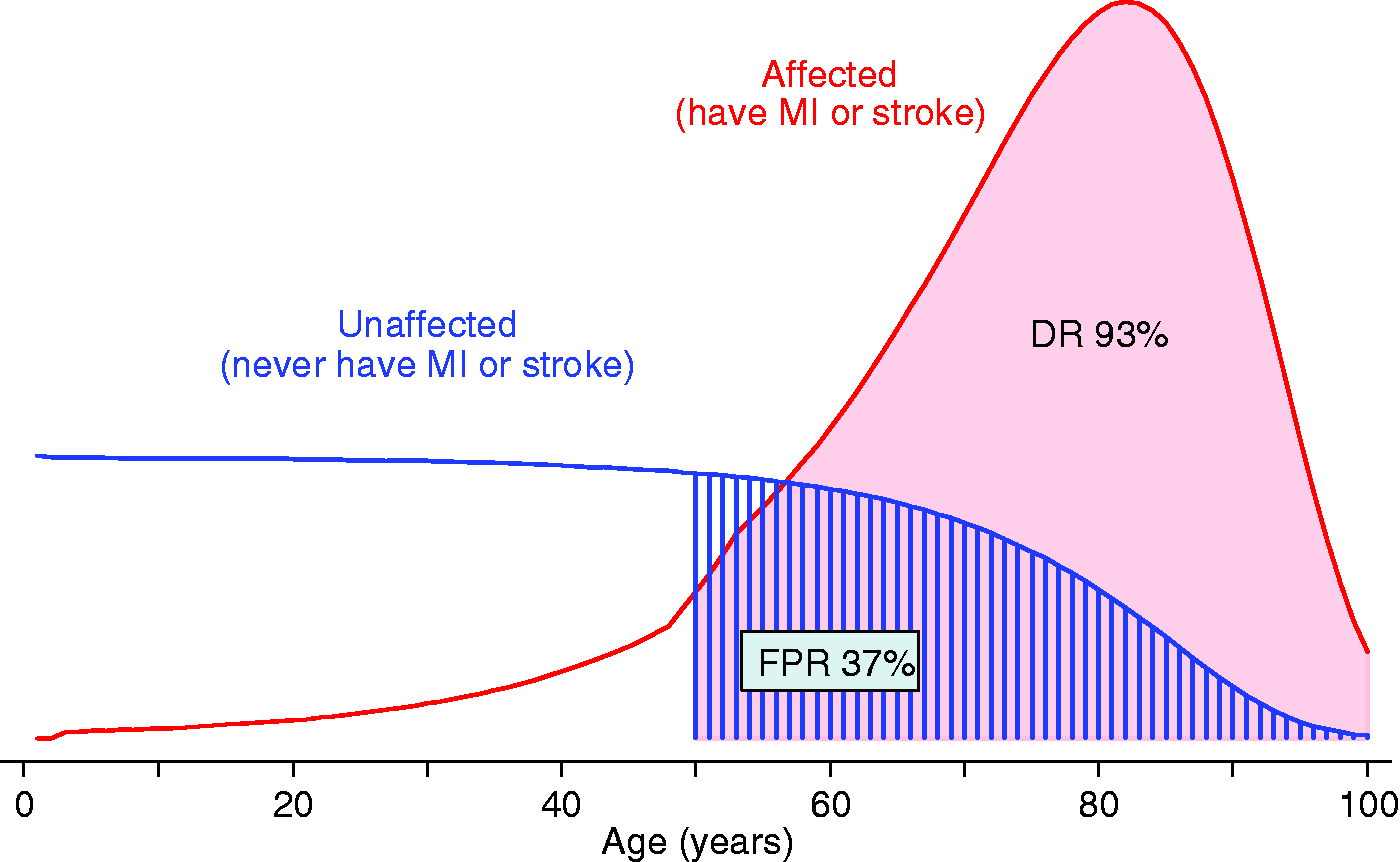
Screening performance, percentage of the population eligible for the polypill and the corresponding health benefits in males and females according to age cut-off.
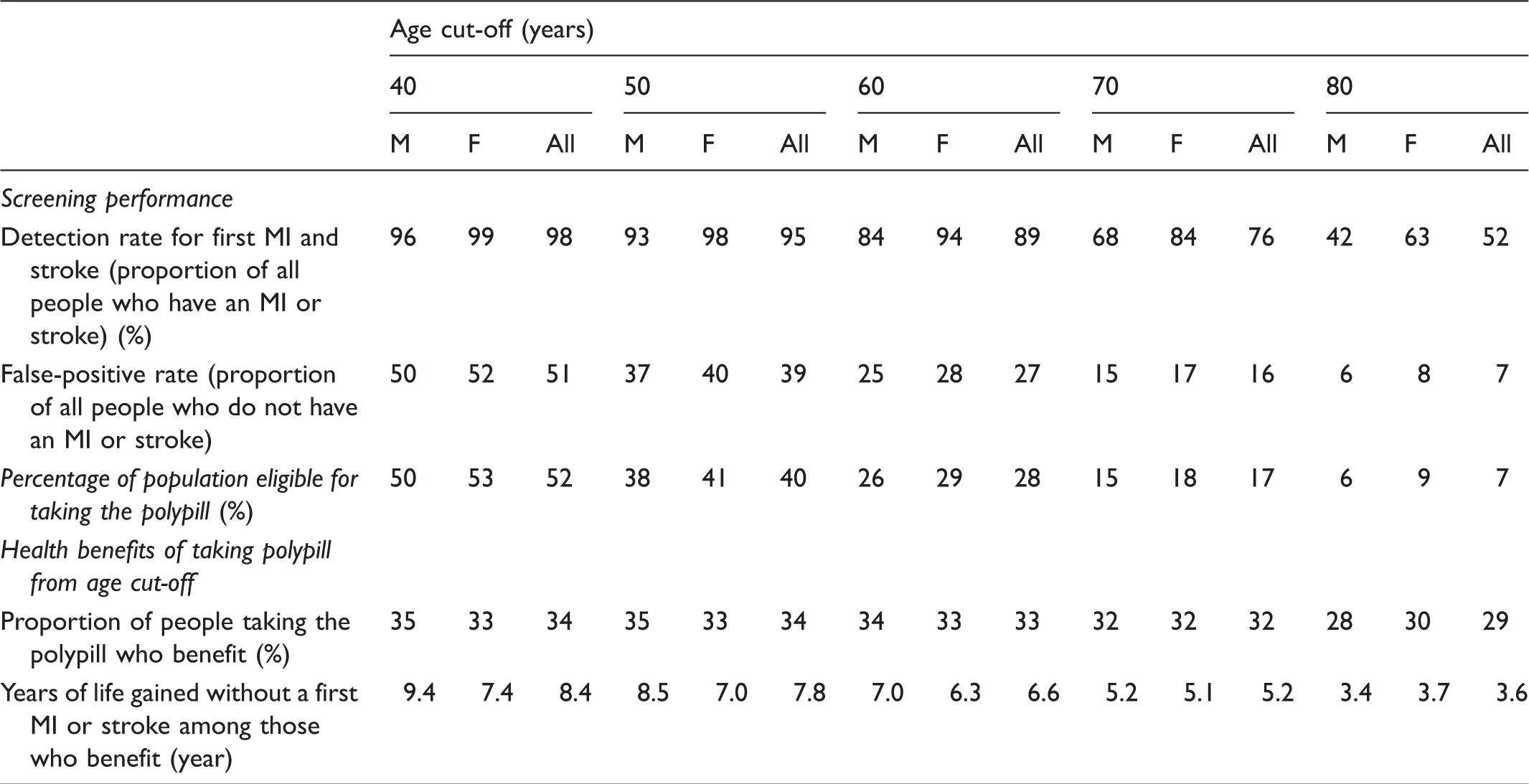
MI: myocardial infarction.
The proportion of the population eligible for the polypill (i.e. the positive rate, not the FPR) also declines with age (52%, 40%, 28%, 17%, and 7% for people starting at ages 40, 50, 60, 70, and 80, respectively). The differences between the sexes are small at all age cut-offs (Table 1).
The proportion of people taking the polypill who benefit from it is approximately one-third at all starting ages (ranging from 34% to 29%, which is the lifetime risk of a first MI or stroke in the absence of preventive treatment). Again, the differences between the sexes are small. The years of life gained without an MI or stroke among those who benefit declines with increasing age of starting (8.4 years at age 40 to 3.6 years at age 80). The sex differences are modest; for example, from age 50, the estimates are 8.5 years in males and 7.0 years in females; the differences decrease with increasing age of starting and reverse between ages 70 and 80.
Discussion
Age has a large effect on the DR, the FPR, the proportion of the population eligible for the polypill, and the years of life gained without an MI or stroke, among people who benefit. At a given age cut-off, the sex differences are relatively small. Consequently, a single cut-off can be used in males and females.
MI and stroke occur at younger ages in males than females, so it might be intuitive to consider that preventive polypill treatment should start at a younger age in males than in females, on the grounds of “equity.” However, Table 1 shows that the notion of equity depends on what parameter is used. The proportion of people who benefit from the polypill is similar in males and females, so from this perspective one sex is not favoured over the other. The DR is higher in females at any age (so favouring females), but the years of life gained without an MI or stroke among people who benefit is higher in males up to age 70 (so favouring males). There are trade-offs inherent in screening, and unless the effect of any given factor is very large, the differences should not be used to modify or complicate the screening process.
The health benefits shown in the table have not been discounted. In a mature Polypill Prevention Programme, the number of years of life gained without an MI or stroke is constant from year to year so the prima facie reason for discounting does not apply. In addition, discounting health benefit secured in the distant future being worth less than benefits secured earlier is, we believe, flawed. 9
Using a single age cut-off for both sexes means that the cost per year of life gained without an MI or stroke is higher for females than for males. The difference (about £1000 per year of life gained) if the daily cost of delivering a Polypill Prevention Programme were about £1 a person 10 is, in our view, not enough to set different age cut-offs for the two sexes, given the advantages of simplicity, uniformity, and a public perception of fairness in implementing public health services. Also, if the age cut-off for women were 10 years later than for men, when the sex-specific costs would be similar, females who benefit from taking the polypill would lose an average of eight months of extra life without an MI or stroke.
The importance of the age cut-off in screening for a first MI or stroke is not surprising. In both sexes, the incidence of MI and stroke increases rapidly with age (approximately doubling every seven to eight years). Our results take into account these quantitative effects showing that overall, in terms of screening and prevention, the practical issue is selecting the single age cut-off, not selecting different cut-offs in males and females. What perhaps is surprising is that, given differences in the age specific incidence rates of MI and stroke in males and females, sex plays a relatively minor role from a screening perspective. The use of a single age cut-off fits in with public policy in general, which has tended to move away from sex discrimination, for example in adopting a common retirement age.
We conclude, therefore, that selecting people for medication in the primary prevention of cardiovascular disease on the basis of a single age cut-off in males and females has the advantage of simplicity, and similar efficacy.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Nicholas Wald jointly holds European and Canadian patents (EU1272220 priority date 10 April 2000) and a US patent (8470868, 25 June 2013) for a combination pill for the prevention of cardiovascular disease and has an interest in its development. He is a founder and director of Polypill Ltd, which owns the website Polypill.com.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.