
Abstract
Cardiovascular disease is the leading cause of death in women and more heart disease is present in elderly women than men. Risk factors for heart disease affect men and women differently, with a greater impact of diabetes, hyperlipidemia and smoking in women. Diagnosis of heart disease can be more challenging in women, especially when elderly, as symptoms may be vague. Understanding the appropriate use of diagnostic testing and appropriate treatment is essential, given the high burden of disease in elderly women. This article will discuss the current guidelines for diagnosis and therapy of heart disease in women and will discuss the appropriate role of prevention strategies.
Cardiovascular disease (CVD) remains the most common cause of death in women, accounting for more deaths yearly than all other causes combined [1]. CVD is more prevalent in men under the age of 40 years compared with women, but in those aged 40–60 years the prevalence is equal, and in elderly women (>60 years) the prevalence of CVD is even greater than in men [2]. More women than men die each year of CVD, a fact that is under-recognized by most physicians [3]. Over the past decade, mortality due to CVD has decreased for men. However, until recently, the mortality in women has actually increased [4]. Owing to a greater understanding of the importance of CVD and the recognition of the risk factors and cardiovascular symptoms, a small trend towards improvement in women can now be observed; although, a wide gender gap persists (Figure 1). Women remain under-represented in major clinical trials and there remains an under-recognition and underdiagnosis of the disease [5]. Both patients and their physicians contribute to this disparity in cardiovascular treatment by their lack of awareness of the significance of the disease in women [3]. Only 21% of women believe heart disease is their major health threat according to the American Heart Association (AHA) [6]. Recent studies demonstrate that physicians continue to under-recognize CVD and myocardial infarctions in women, perform less testing for CVD and less aggressively manage CVD in women when it is identified [7–10].

Sex-based cardiovascular mortality from 1979 through 2004.
Managing CVD in women requires an understanding of the sex-based differences in the epidemiology and presentation. A careful assessment of the risk factors and their implication in women is a mainstay in approaching CVD. Incorporating a detailed clinical history with complete risk assessment will allow the clinician to properly evaluate women who present with symptoms suggestive of CVD.
Coronary heart disease
Coronary heart disease (CHD) is the leading cause of the increased CVD deaths observed in women. Given the aging population and the epidemics of obesity, metabolic syndrome and diabetes, increases in CHD will continue. Clinical manifestations of CHD appear approximately 10 years later in women compared with men [11,12]. However, the prevalence increases rapidly after menopause [11]. The limited research in this area suggests that women have greater functional limitations from CHD, as well as a higher likelihood of abnormal, noninvasive findings that suggest CHD [13–16]. Despite this, women have a lower prevalence of obstructive coronary artery disease. The Women's Ischemic Syndrome Evaluation (WISE) study found that of the women who underwent angiography for the evaluation of chest pain or an abnormal stress-test result, only 43% had significant stenoses [16,17]. In the women without significant stenoses, if symptoms of chest pain persisted, they had more than three-times the 6-year risk of myocardial infarctions than those without persistent symptoms [18]. The abnormal stress tests, which were part of the inclusion criteria – that were suggestive of ischemia – may have been the result of microvascular disease, endothelial dysfunction or both [19]. Impaired endothelial vasomotor function of the coronary arteries and microvascular dysfunction are both associated with a long-term risk of cardiovascular events [19,20].
Once women progress to obstructive coronary disease, their outcomes are worse compared with men. Although women tend to present less often with acute coronary syndromes, the mortality in young women after a myocardial infarction approaches twice that of men [21–23]. However, in elderly women (>74 years) evaluated in the National Registry of Myocardial Infarction 2, sex was not demonstrated to be a risk factor for mortality (Figure 2) [22]. Women who undergo coronary artery bypass surgery also have twice the mortality risk as men, which is primarily a result of their older age and a higher rate of comorbidities [24,25]. Rates of revascularization are lower in women [26]. Given the benefit of revascularization in women, especially diabetics, aggressive medical management and revascularization should be strongly considered.

Impact of age and sex on in-hospital mortality from an acute myocardial infarction.
Heart failure
Heart failure, a recognized complication of CHD, has become more prevalent over the last several years, particularly as people with CHD are living longer. According to the Framingham study, approximately 20% of both sexes have a lifetime risk of heart failure [27]. The risk of decreasing left ventricular systolic function increases with age [28]. Epidemiologic studies of patients with heart failure reveal higher rates of survival for women compared with men [29,30]. As with CHD, the majority of women with heart failure are older than their male counterparts with a higher rate of hypertension and diabetes [31,32]. However, women tend to have higher ejection fractions and more diastolic heart failure [33]. The greater prevalence of heart failure associated with preserved ejection fraction in women has been postulated as the factor contributing to lower mortality rates. Frazier et al. pooled five randomized, controlled trials in order to assess sex-based differences in etiologies and outcomes in chronic systolic heart failure [34]. Among the women in the study, approximately 60% had a nonischemic etiology (in men 43% were nonischemic). Regardless of the etiology, women had a better survival compared with men.
Stroke
Stroke is a major cause of death, regardless of sex. Goulene et al. evaluated patients admitted for an acute cerebrovascular event, assessing the neurological impairment and disability at discharge and at 1 year [35]. At 1 year, there was a greater degree of neurologic impairment in women. The older age of women at presentation appeared to only partially explain the difference. The clinical presentation and outcome of stroke appear to differ based on sex as well as clinical management [36]. The elderly are at a higher risk of stroke, but preventive strategies must be weighed against the higher risk of certain prevention strategies [37]. Atrial fibrillation as a cause of stroke occurs more commonly in women compared with men. The Anticoagulation and Risk Factors in Atrial Fibrillation (ATRIA) study of approximately 15,000 patients with atrial fibrillation found a higher rate of stroke in women, and it was even higher in women over 75 years of age [38]. Despite this, women with atrial fibrillation receive less oral anticoagulation therapy prior to their stroke compared with men, which is more remarkable because of the high-risk features associated with women [38,39]. Thus, strong consideration to anticoagulation in the elderly female patient with atrial fibrillation is appropriate, given the increased stroke risk.
Obstructive carotid disease is a significant risk for stroke and recurrent stroke in both men and women. Risk factor reduction by treatment of hyperlipidemia, hypertension, diabetes, weight control, exercise and smoking cessation are all important in both primary and secondary prevention. Data also support the use of aspirin as primary prevention, and antiplatelet therapy for the treatment of a noncardioembolic stroke. Carotid endarterectomy is also beneficial for both primary and secondary prevention, but may carry increased risk in the elderly [37]. However, there appears to be no sex-based differences on the safety or efficacy of revascularization [40]. After a stroke, the risk of a myocardial infarction, stroke or death within 5 years is 47.3%, with no difference observed between men and women [41]. The risk of subsequent events in those over 70 years of age was 67% higher. Thus, aggressive management of elderly women following a stroke is important for the prevention of recurrent strokes as well as myocardial infarctions and death.
Cardiovascular risk factors
Identifying the primary cardiovascular risk factors in women must be an important component of periodic health screening. Guidelines from the National Cholesterol Education Program (NCEP) and scientific statements from the AHA and the American College of Cardiology (ACC) [42] identify the following risk factors as part of a women's risk assessment: age over 55 years, dyslipidemia, family history of premature CHD, smoking and hypertension. The cardiovascular risk equivalents of peripheral arterial disease, personal history of CHD and diabetes mellitus, are even stronger prognostic factors in a woman's risk assessment and mandate aggressive prevention. In addition, elevated triglycerides, obesity, glucose intolerance, prehypertension and a sedentary lifestyle are highly associated with coronary risk, although they are not considered to be primary risk factors [42]. To practice an appropriate risk-modification strategy, the aggressiveness of risk modification is generally based on the overall risk. In men, the Framingham risk score has been widely used, but in women this scoring system does not ideally identify risk [43–45]. Therefore, the Reynold's risk score has been developed, which includes traditional risk factors and C-reactive protein [46].
Lipids
The lipoprotein risk factors for CHD are somewhat different in women compared with men. Low high-density lipoprotein (HDL), rather than high low-density lipoprotein (LDL)-cholesterol, is more predictive of coronary risk in women [47]. Triglycerides influence risk in older women [47,48]. In the Women's Health Study, the total cholesterol:HDL ratio was the most predictive of cardiovascular events in a group of over 15,000 healthy women over 45 years of age [49]. In both primary and secondary prevention studies of CHD, women have greater risk reduction with statin therapy (Figures 3 & 4) [50–52]. In addition, secondary prevention trials of coronary atherosclerosis regression with statin therapy have greater efficacy with women [52–55]. Guidelines for the treatment of hypercholesterolemia are identical between men and women (Table 1) and there is currently no known age at which statin therapy does not improve survival when used for secondary prevention [52,53,56]. Despite the marked survival benefit of aggressive statin therapy for prevention in elderly women, there remains a large proportion of high-risk women who are not effectively treated and who do not meet goal LDL-cholesterol levels. Major benefit can be achieved by following the lipid-reduction guidelines in these women.
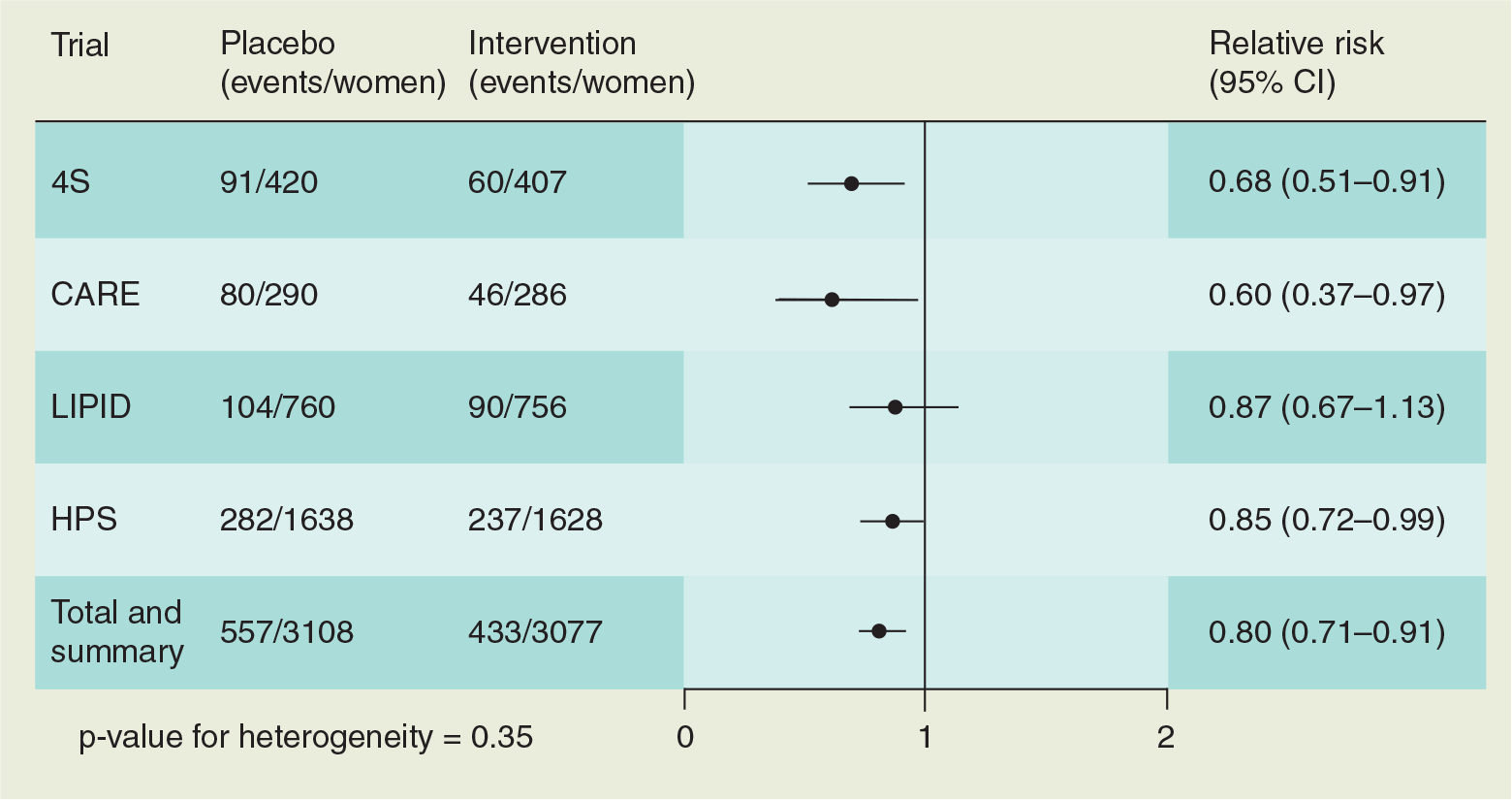
Secondary prevention of coronary heart disease events with statin therapy in women.
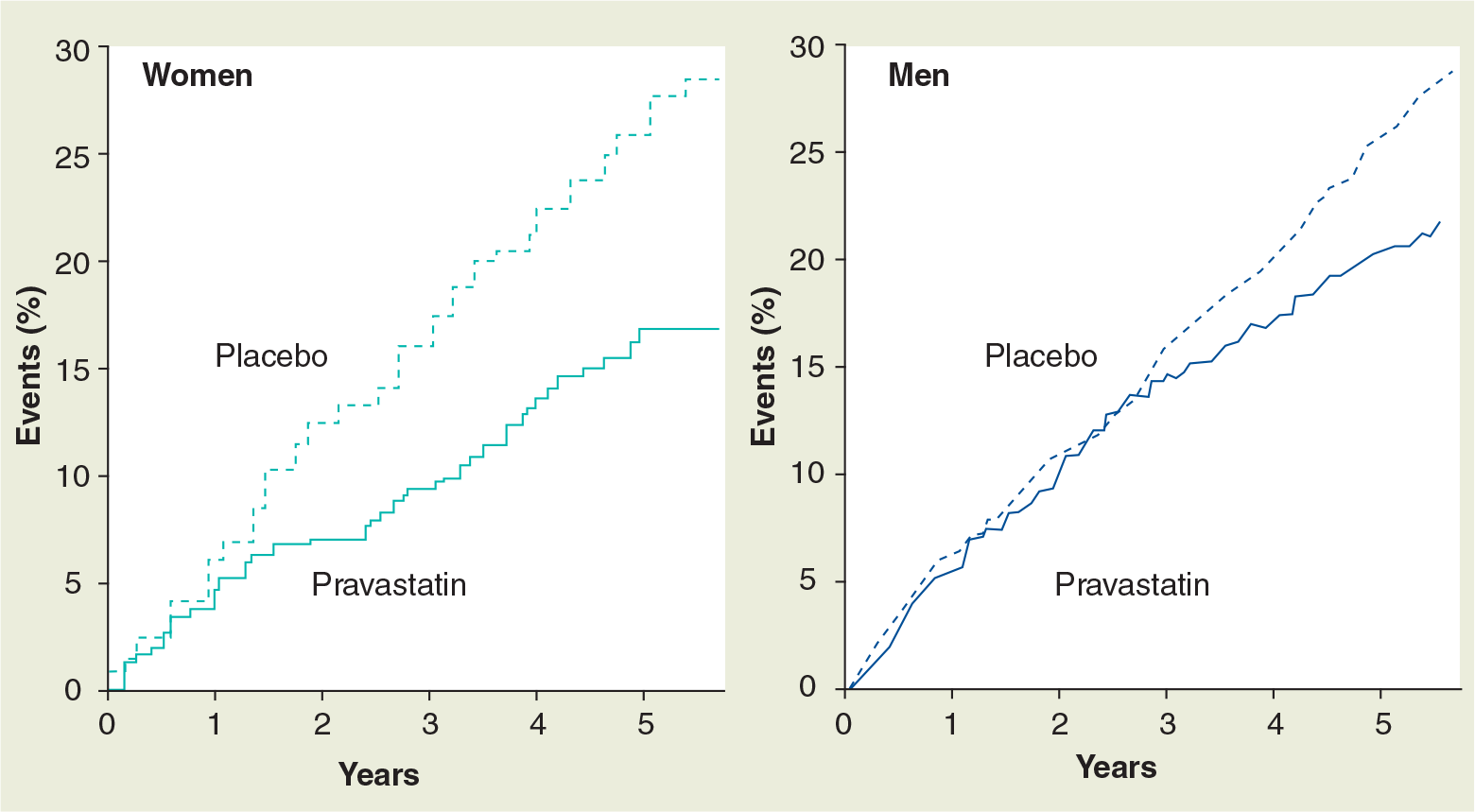
Impact of gender on secondary prevention of cardiovascular events with pravastatin therapy in the Cholesterol and Recurrent Events (CARE) trial.
National Cholesterol Education Program guidelines for lipid goals.

CHD: Coronary heart disease.
Data obtained from [56].
Diabetes mellitus
Diabetes is an important risk factor for CHD with a greater risk presented in women than men [57,58]. Patients with Type 2 diabetes without a prior myocardial infarction have the same risk and coronary mortality as a nondiabetic patient with a prior infarction (Figure 5) [59]. Thus, diabetes has become a cardiovascular risk equivalent for both men and women. Cardiovascular mortality rates in diabetic women are close to three-times higher than those seen in men [60]. Good diabetic control reduces cardiovascular events in both men and women with a goal for hemoglobin A1C less than 7 [61,62]. Recent studies conflict as to how tight diabetic control should be, and there may be a point, especially in patients with established CHD, that too tight a control is associated with increased mortality. Early evidence suggests medications, such as pioglitazone, may slow atherosclerosis progression, but further studies are required to confirm these results [63].

Risk of a myocardial infarction based on coronary heart disease and diabetes.
Tobacco
Tobacco use is an important risk factor in both sexes. The prevalence of smoking is higher in men; however, the decline in smoking rates is less evident in women [64]. Half of all coronary events in women are associated with smoking [65]. Coronary risk appears elevated even in women with minimal use (relative risk [RR]: 2.1 for 14 cigarettes/day) [65,66]. Smoking cessation results in a rapid reduction in the risk of myocardial infarction, approaching the risk in nonsmokers within 2–3 years of cessation [67]. Owing to the greater difficulty in smoking cessation in women, the astute clinician must use all resources, including medications and psychosocial support mechanisms, to help improve the odds for success in women.
Hypertension
In elderly women (>70 years), the prevalence of hypertension approaches 70–80% [68]. Isolated systolic hypertension is the more common form of hypertension in the elderly women [69]. The overall incidence of hypertensive complications is lower in women compared with men. However, in elderly women, hypertension is a stronger predictor of coronary risk compared with men, and increased risk is observed even with borderline blood pressures [66]. Optimal blood pressure is defined as less than 120/80 mmHg. Therapy in hypertensive women is similar to men and follows the recommendations set forth by the Joint National Committee (JNC)-7. Control of hypertension decreases the risk of CHD and stroke in both genders as observed in several large clinical trials [70].
Metabolic syndrome
The clinical identification of the metabolic syndrome using the AHA/National Heart, Lung and Blood Institute (NHLBI) definition is based upon the presence of any three of the following characteristics [71]:
Central obesity as measured by waist circumference (women >35 inches)
Fasting triglycerides greater than or equal to 150 mg/dl
Low HDL-cholesterol (women <50 mg/dl)
Blood pressure greater than or equal to 130 mmHg systolic or greater than or equal 85 mmHg diastolic
Fasting glucose greater than or equal to 100 mg/dl
The metabolic syndrome is associated with a significant increase in the risk of cardiovascular events in both men and women. In the WISE study, metabolic syndrome was identified in 25% of the women referred for coronary angiography [72]. These women had a higher mortality rate at 4 years, as well as a higher rate of major cardiovascular events. This increased mortality rate was independent of BMI. This relationship appears to indicate that visceral fat and not total body obesity (as measured by BMI) is a more valuable risk predictor [73]. Abnormal metabolism rather than obesity alone may require more attention when assessing overall cardiovascular risk in a women.
Menopause
The postmenopausal woman has the same risk of heart disease as a man. After menopause, lipid levels worsen with an increase in LDL-cholesterol and a decrease in HDL. In addition, hypertension and the metabolic syndrome increases, and hypertriglyceridemia, diabetes mellitus and abdominal obesity are more common. It is unclear whether menopause itself is a risk factor for CHD or a surrogate for other risk factors. Marked changes in the recommendations for estrogen therapy have occurred in the past decade. Estrogen therapy used to be a mainstay of therapy for heart disease and treatment of abnormal lipids in women [74], even when the onset of menopause was remote. Potential beneficial effects of estrogen include an improvement in lipid profile, enhanced endothelial function and improved insulin sensitivity. Adverse effects of estrogen include an elevation in triglyceride levels with oral estrogens, prothrombotic effects from a reduction in fibrinogen, factor VII and antithrombin III, and an increase in vascular inflammatory markers (C-reactive protein) [75]. Progestins may negate some of the potential beneficial effects with the estrogens. Multiple prospective studies of primary prevention with hormone therapy (HT), including the Women's Health Initiative (WHI) [76] and the Heart and Estrogen/Progestin Replacement Study (HERS)-I and -II trials [77,78], failed to demonstrate a benefit from therapy. In fact, the WHI demonstrated increased cardiovascular events with therapy (Table 2). In the placebo-controlled estrogen and progesterone study investigating over 16,000 women, the risk of breast cancer, stroke, CHD and venous thromboembolism increased, requiring an early termination of the study. The placebo-controlled unopposed estrogen study of nearly 11,000 women was also stopped early owing to an increased risk of stroke and venous thromboembolism. The benefit of HT was seen in regard to fracture risk and the risk of colorectal cancer. Thus, at present, HT is not recommended for postmenopausal women on the basis of cardioprotection, and may be potentially harmful, especially in the elderly woman who is not perimenopausal. Current hormonal studies are focused on different estrogen and progesterone regimens as well as being focused on the perimenopausal woman, where the benefits of therapy may be greatest [79]. In the postmenopausal woman, the US FDA recommends the shortest duration of estrogen therapy at the lowest dose in order to alleviate menopausal symptoms; current studies do not support a role for estrogen in CVD prevention or treatment.
Clinical outcomes in the estrogen and progesterone study of the Women's Health Initiative.

Data obtained from [76].
Dietary fat
Dietary fat intake may play a role in the risk of CHD. In the Nurses' Health Study, over 80,000 women between 34 and 59 years of age who were free from CVD and hypercholesterolemia were prospectively evaluated [80,81]. The risk of CHD was found to be increased based on the amount of consumption of saturated or transunsaturated fat. The risk was reduced in women who consumed higher amounts of monounsaturated or polyunsaturated fat. It was estimated that if saturated and trans fat were replaced by unsaturated fats, the risk of CHD would be reduced by 40–50%.
Exercise & cardiac rehabilitation
In the elderly, regular exercise is associated with a lower incidence of new CHD diagnoses after 2 years [82] and is also associated with improvements in the cardiovascular risk profile [83]. In CHD patients, exercise is effective in reducing mortality in both women (adjusted RR: 0.47) and in those aged 65–76 years and those over 76 years (adjusted RR: 0.67 and 0.45, respectively) [84]. Despite the benefits of exercise, both women and the elderly are referred less frequently for cardiovascular rehabilitation and when they are referred, they attend less often [85,86]. In the elderly, cardiac rehabilitation is associated with decreased weight, increased HDL-cholesterol and decreased fasting glucose, with a marked benefit of a 34% increase in exercise capacity [87]. In addition, scores for anxiety, depression, somatization and quality of life improved by 40, 40, 33 and 17%, respectively, with cardiac rehabilitation.
Renal disease
Renal disease is now a well-established risk factor for CVD and mortality, with a graded risk with decreased renal function [88]. Renal disease is very prevalent in the elderly population. Current recommendations are to aggressively treat other cardiovascular risk factors, such as hyperlipidemia, as if the patient has CVD, with a goal of LDL-cholesterol less than or equal to 100 mg/dl. In addition, in the elderly woman, careful calculation of renal function is needed using either the Cockroft–Gault equation or the modification of diet in renal disease equation because in these patients, renal function can be significantly impaired with minimal changes in the serum creatinine [89].
Inflammation
Markers of inflammation have been recently implicated as a risk for CVD. C-reactive protein was found to be a strong independent risk factor for CVD within the Women's Health Study and may be a more important risk factor in women compared with men [49,90]. It is additive to the more traditional risk factor of total cholesterol, and treatment with statins decreases inflammation and improves outcomes. Other inflammatory markers, including an elevated baseline white blood cell count, serum amyloid A and IL-6, are also predictors of cardiovascular events, but are more difficult to measure than C-reactive protein and, therefore, are less useful. Measurement of inflammatory markers may be helpful in the risk assessment of women, as 50% of all cardiovascular events occur in women without hyperlipidemia.
Psychosocial & behavioral factors
Psychosocial and behavioral factors alter the risk and prognosis in women with CHD [91]. Lower socioeconomic status, particularly in women, is associated with a higher cardiovascular mortality. Depression not only confers a higher risk of adverse outcomes after a cardiovascular event, it also prevents adherence to a healthy lifestyle. The treatment of depression is indicated to reduce adverse outcomes in both men and women with heart disease, especially after a myocardial infarction [92]. Particularly in the elderly, depression can be overlooked, so careful assessment is needed for optimal patient care.
Diagnosis of coronary heart disease
Women are less likely to have typical anginal chest pain compared with men, especially in the elderly. Symptoms of dyspnea, nausea, fatigue and a vague uneasiness are not uncommon [93]. Owing to the atypical nature of the symptomatology, elderly women who present to the emergency room with an acute coronary syndrome or outpatients with angina or anginal equivalents may be diagnosed less aggressively than men [94].
Assessing the risk profile for CHD requires the synthesis of multiple risk factors. The 2004 guidelines for CVD prevention in women underscore the importance of the spectrum of CVD [95]. In these guidelines, women were classified into optimal-, low-, intermediate- and high-risk categories, based primarily on clinical criteria and the Framingham global risk score. However, the 2007 update [42] recommended a scheme for a more general approach to women based on the classification of ‘at high risk’, ‘at risk’ or ‘at optimal risk’ (Table 3). The rationale for this change was the need to understand that the average lifetime risk for CVD in women was quite high and, thus, all risk factors need to be identified and treated as appropriate [96]. The limitations on risk stratification using the Framingham global risk score, especially in light of the short-term (10 years) assessment, have been brought to attention. Lifetime risk assessment is a more appropriate approach in women with greater emphasis on lifetime prevention.
Classification of cardiovascular risk from the American College of Cardiology and American Heart Association guidelines on heart disease in women.

Data obtained from [42].
After the assessment of a woman's risk for CVD, the decision needs to be made as to the optimal diagnostic algorithm. Noninvasive testing, aimed at diagnosis and prognosis, has the potential to identify women at increased CHD risk and provide the basis for preventative and therapeutic interventions. In the evaluation of symptomatic women with chest pain, the questions that need to be addressed include: what is the patient's pretest probability of disease? How does the accuracy of the alternative tests compare? What are the costs and effects on outcomes on each test? Are there special considerations that make one test more suitable over another in a specific patient? The ACC/AHA have issued guidelines for the role of exercise testing in patients with chest pain [97]. The patient's ability to exercise and the ability to detect electrocardiographic changes induced by ischemia are taken into account. However, in women, these general guidelines are not always applicable. Women have been notoriously under-represented in studies involved in noninvasive testing. The accuracy and limitations of stress testing in women have remained a confusing dilemma. Stress testing is not advocated for the low-risk asymptomatic women, or for the asymptomatic women at high risk, who should be aggressively treated for secondary prevention. Treadmill exercise testing carries with it a lower sensitivity (61%) and specificity (70%) in women compared with men [98]. A positive or negative exercise stress test has a relatively low predictive value in a woman. Utilizing the Duke treadmill score improves the ability to exclude disease, particularly in women [99]. The ACC/AHA guidelines recommend exercise testing in women with an intermediate pretest probability of CHD (based on symptoms and risk factors), normal resting electrocardiograms and who are capable to exercise. Incorporating functional capacity data, such as the ability to achieve five metabolic equivalents on the treadmill and heart-rate recovery, may be additive factors in the interpretation of exercise testing [100,101].
Imaging, either with nuclear myocardial perfusion or with echocardiography, increases the diagnostic accuracy of stress testing in both men and women. The guidelines from the ACC/AHA recommend the use of imaging in patients with an intermediate probability of CHD, when there are resting electrocardiographic abnormalities, or in patients with prior coronary revascularization. Dobutamine echocardiography or adenosine-perfusion imaging is indicated in patients unable to exercise. Adenosine imaging is also indicated in patients with a left bundle branch block or a ventricularly paced rhythm. Myocardial perfusion imaging may play an important role in women in the diagnosis of microvascular disease (abnormal perfusion imaging in a patient with normal epicardial coronary arteries) [19]. The sensitivity and specificity of nuclear stress testing and stress echocardiography are not significantly different [98]. From the standpoint of accuracy and cost–effectiveness, the optimal diagnostic strategy in women with CHD is not quite known. All of the noninvasive tests have a potential for artifact. At present, test selection should be dictated by availability and local expertise.
There are new and evolving imaging techniques that may play a role in the detection of subclinical CHD. Their role is not yet defined. They include: computed tomography (CT) with calcium scoring, MRI and carotid intima-media thickness (IMT).
Calcification of the coronary arteries occurs in the presence of atherosclerosis. Its presence is not specific for obstruction of the coronary itself. Coronary artery calcium (CAC) scores reflect the total burden of atherosclerosis [102]. The higher the CAC score, the greater the prevalence of obstructive disease. A low CAC score is associated with a low adverse event rate. At present, the exact role of CAC is unclear. It may be helpful to further risk-stratify asymptomatic patients at intermediate risk of CHD. Updated guidelines are available to help facilitate appropriate use of CT for patients with chest pain and those who are asymptomatic [103]. High-quality data from large cohorts are needed to establish female-specific CAC risk.
Cardiovascular MRI (CMR) has evolved significantly in the past decade. This modality will probably become an accepted technique to assess for myocardial ischemia. CMR has the potential to directly visualize coronary stenosis [104] as well as assess flow within the coronaries [105], although the ability to fully visualize the coronary arteries is still limited. Myocardial perfusion, metabolism and wall motion (during rest and stress) are additional data that can be obtained. However, there is limited information supporting the role of CMR in CHD detection specifically in women.
High-frequency carotid ultrasound to detect subclinical atherosclerosis in the carotid artery, including the thickness of the IMT, has been studied as a marker for CHD risk in women. Observational data demonstrate that carotid IMT is strongly associated with the risk of cardiovascular events, after adjustment for traditional risk factors [106,107]. However, once again, the clinical use of carotid IMT has not been specifically shown to result in improved outcomes.
Treatment
Currently, there is no difference in the treatment recommendations for CVD based on sex or age except for primary prevention with aspirin. However, women tend to receive more nitrates, calcium-channel blockers, diuretics and sedatives than men, and are less likely to receive aspirin, β-blockers and statins [108–110]. Given the significant morbidity and mortality associated with CVD in women, equally aggressive management with known effective therapies is warranted in elderly women.
The elderly population requires some important differences in the approach to medical management. The elderly have a lower lean body mass and decreased renal function. Thus, the bio-availability and metabolism of medications can be altered in the elderly. In addition, medication side effects can be more pronounced. Therefore, slow titration of medications is necessary.
Aspirin was demonstrated to be as beneficial in women as it was in men in the Antiplatelet Trialists' Collaboration for secondary prevention [111], and is also an important part of initial therapy when women present with an acute coronary syndrome. In the Women's Health Study, aspirin was not beneficial for primary prevention of a myocardial infarction except for women over 65 years of age [112]. However, aspirin was found to be beneficial in the prevention of stroke in all women in this study. Other commonly used cardiovascular medications include β-blockers, which have shown a clear benefit in women after myocardial infarction similar to that observed in men [113]. Angiotensin-converting enzyme inhibitors have not been specifically studied in women, but appear, from substudies, to be equally efficacious and clinicians should use the same criteria for their use in women as that for men [114]. Statins may have a greater benefit in women with CHD and guidelines for therapy of elevated cholesterol are identical for men and women.
There are some conflicting data as to whether women benefit from early invasive therapy in regard to a non-ST segment myocardial infarction. Women with low risk scores upon presentation with an acute coronary syndrome appear to have a nonsignificant trend toward a worse outcome with an early invasive strategy; men with a low risk score had no benefit or harm [115]. Women did have significantly higher rates of bleeding after percutaneous coronary interventions (PCIs) compared with men. The 2007 update from the ACC/AHA task force recommends that women with unstable angina or a non-ST elevation myocardial infarction be managed similarly to men, using the same criteria for noninvasive and invasive testing [116]. Women who have high-risk features benefit from an early invasive strategy. In a review from the Can Rapid Risk Stratification of Unstable Angina Patients Suppress Adverse Outcomes With Early Implementation of the ACC/AHA Guidelines (CRUSADE) national quality improvement initiative, women were less aggressively treated compared with men [26]. They were less likely to undergo cardiac catheterization and PCI compared with men.
Treatment recommendations for a ST-elevation myocardial infarction in women are generally the same as in men. In most studies, women tend to receive fibrinolytics less often than men, and are more likely to experience a delay in presentation to the emergency room and initiation of therapy [117–119]. Women have a higher mortality and morbidity rate with fibrinolysis compared with men, but it is unclear if this may be secondary to the older age at presentation and to the higher rates of diabetes, hypertension and prior heart failure observed in women [119–121]. In the elderly patient, there have been some conflicting data as to the benefit of fibrinolytic therapy. In the Cooperative Cardiovascular Project, a nonrandomized study investigating 7864 Medicare patients eligible for fibrinolytic therapy where 34% were over the age of 75 years, they found no benefit with fibrinolytic therapy in those over 75 years of age, while there was benefit in those 65–75 years of age [122]. In those over 75 years, the greatest hazard was in the women who had a 60% increased risk of 30-day mortality. However, these data were challenged by the Fibrinolytic Therapy Trialists' (FTT) overview, which combined data from nine randomized trials and found that the 35-day mortality rate in the 5788 patients who were over 75 years was lower in those who received fibrinolytic therapy than in those who did not (24.3 vs 25.3%, respectively) [123]. There was a similar absolute risk reduction in the elderly as in the younger patients, with a lower proportional reduction in the elderly. Not surprisingly, these elderly patients had greater complications, including intracranial hemorrhage. The current scientific statement from the AHA and Society of Geriatric Cardiology supports the use of fibrinolytic therapy in those up to the age of 85 years, when eligible, because of the demonstrated mortality benefit, but in older patients there is no strong consensus because of the paucity of data and increasing risk of complications [124]. With primary PCI, women have higher rates of in-hospital and longer term mortality compared with men [125,126]. However, this difference disappears when multivariate analysis is performed, which adjusts for the older age and higher rate of comorbidities [125,127]. In one study of aggressive PCI in all patients, women actually had a lower mortality than men after adjustment for older age, and a higher prevalence of diabetes and hypertension [128]. After primary PCI, women tend to have more myocardium salvaged, resulting in smaller infarct size, compared with men [129]. In the elderly, PCI has small but significant benefits compared with fibrinolytics, but again there are limited data in those over the age of 80 years [124]. Importantly, more elderly patients will meet the criteria for reperfusion therapy by PCI compared with fibrinolytics and, therefore, can receive the benefits from reperfusion when available. In patients with cardiogenic shock who undergo early revascularization, women appear to have the same benefit as men [130]. However, in the subgroup analysis of those over the age of 75 years, the same benefit with early revascularization was not observed [131]. Despite this finding, elderly women with an acute myocardial infarction should be considered for reperfusion therapy, especially with PCI.
Conclusion
Rates of heart disease mortality are decreasing. However, a wide disparity still exists between men and women. Risk-factor profiles are necessary to determine life-long cardiovascular risk since women have a high lifetime risk of CVD. The clinician must recognize that symptoms may be vague and more difficult to interpret, especially in the elderly woman. Nonetheless, there are appropriate diagnostic modalities available to help define cardiovascular risk in women. Evidence-based guidelines exist to help identify and treat women at risk and are not vastly different from the approach employed in men. An important goal must be to educate both the physician and the patient, in order for both to recognize the importance of CVD prevention and treatment in women.
Future perspective
Older women will continue to be at risk for CHD and to represent an increasing portion of the population with CHD. Primary prevention will need to focus more on life-long risk of CHD in women, and secondary prevention strategies in older women need greater adherence to the current guidelines. Older women are less often optimally managed for their heart disease. Symptoms of heart disease and myocardial infarction in the older woman makes the diagnosis more challenging, so continued physician and patient awareness programs are needed. Newer testing modalities, such as CT and MRI, may have greater benefit in the diagnosis of CHD in this population, but specific studies in older women are warranted to determine an optimal diagnostic testing modality. Further studies specifically evaluating older patients and older women are needed to better identify the optimal treatment regimen in these patients.
Information resources
Information on NCRR is available at www.ncrr.nih.gov
Information on Re-engineering the Clinical Research Enterprise can be obtained from http://nihroadmap.nih.gov/clinicalresearch/overview-translational.asp
Executive summary
Cardiovascular disease is the leading cause of death in women and requires aggressive risk reduction in accordance with a woman's lifetime risk of heart disease.
Given the aging population and the epidemics of obesity, metabolic syndrome and diabetes, increases in coronary heart disease (CHD) will continue.
Women have greater impact from the risk factors of diabetes, hyperlipidemia and smoking compared with men, but also receive more benefit from treatment.
Women have more symptoms associated with CHD, such as dyspnea, fatigue and nausea, and less obstructive coronary disease compared with men.
Treadmill exercise testing has a lower sensitivity and specificity in women compared with men, and adjunctive imaging may be of greater benefit.
The American College of Cardiology/American Heart Association guidelines recommend exercise testing in women with an intermediate pretest probability of CHD (based on their symptoms and risk factors), those with normal resting electrocardiograms and those who are capable of exercising.
There is no difference in the treatment recommendations for CHD based on sex or age and, when indicated, treatment should include aspirin, β-blockers, statin therapy and angiotensin-converting enzyme inhibitors.
For women with a non-ST elevation myocardial infarction, they may not achieve the same benefit of an early invasive approach, however, high-risk women should still undergo revascularization.
For ST-elevation myocardial infarctions in women over the age of 80 years, there are limited data on the efficacy of fibrinolysis, thus individualized care is needed that takes into account the increased risk of bleeding complications and increased mortality risk from the myocardial infarction. Primary percutaneous coronary intervention in older women may have greater benefit over fibrinolytics when available.
In elderly women, because of their lower lean body mass and decreased renal function, dose adjustments to medications are important.
Footnotes
This publication was made possible by grant number 1 KL2 RR024151–01 from the National Center for Research Resources (NCRR), a component of the National Institutes of Health (NIH), and NIH Roadmap for Medical Research. Its contents are solely the responsibility of the authors and do not necessarily represent the official view of NCRR or NIH. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.