
Abstract
Objective
High viral load of oncogenic human papillomavirus (HPV) significantly increases risk of CIN 2 or worse (CIN 2+) lesions. Semi-quantitative estimation of oncogenic HPV viral load by Hybrid Capture 2 (HC2) correlates well with viral load estimated by real-time polymerase chain reaction. We correlated viral load estimated by HC2 with colposcopy and histology diagnosis, to determine if high viral load could detect the CIN 2+ lesions missed by colposcopy in HPV positive women.
Methods
Using HPV testing by HC2, 39,728 women were screened. Positive results were categorized into low-positive, intermediate, and high viral load groups, based on relative light unit/cut-off ratios. HPV-positive and some HPV-negative women underwent colposcopy and biopsy.
Results
A total of 278 CIN 2+ lesions were detected. Detection rate of CIN 2+ was significantly higher in intermediate and high viral load groups. Nearly half (48.3%) of CIN 2+ and 80.4% of CIN 3+ lesions missed or under-diagnosed by colposcopy had viral load in intermediate to high ranges. Risk of CIN 2+ in the high viral load group was 46 times higher than HPV-negative women, even when colposcopy was apparently normal.
Discussion
Women with intermediate or high viral load should have multiple punch biopsies, even if colposcopy is apparently normal or suggests low grade lesions. Women with high viral load and suspected low grade lesion on colposcopy may be considered for ‘see-and-treat’, as their risk of CIN 2+ is nearly 200 times higher than HPV-negative women.
Introduction
Although oncogenic Human Papillomavirus (HPV) infection is the primary cause of cervical cancer, in the majority of infected women the virus clears spontaneously, and the women do not develop the disease. The specificity of HPV detection tests is sub-optimal in screening for cervical cancer. 1 Triaging HPV positive women by Pap smear cytology or genotyping is recommended to identify those at higher risk for colposcopy referral, but such triaging is not always feasible, and all HPV positive women will require colposcopy referral. Colposcopic evaluation of HPV positive women is not standardized and no definite guidelines exist regarding the indications of punch biopsies and excisional biopsies.
The risk of high grade cervical intraepithelial neoplasia (CIN) significantly increases with high viral load of oncogenic HPV types, especially type 16.2,3 High HPV viral load is also associated with higher risk of persistent infection and future development of CIN 2 or worse (CIN 2+).4-7 However, the measurement of HPV viral load by real time polymerase chain reaction (RT-PCR) based assays is still too complex to be used in routine clinical settings.
The Hybrid Capture 2 (HC2) high-risk HPV DNA test (QIAGEN, Gaithersburg, USA)8,9 provides semi-quantitative estimation of viral load, which has been observed to correlate well with the viral load estimated by RT-PCR. Many countries are likely to introduce HPV testing as the primary cervical cancer screening test. We correlated the viral load estimated by HC2 with colposcopy and histology diagnoses, to assess the predictive value of viral load in detecting high grade lesions among the HPV-positive women with no visible abnormality, or minor changes on colposcopy. A high predictive value may justify punch or excision biopsies in this group of women to improve detection of CIN 2+ lesions.
Methods
Women aged 30-60 were screened for cervical cancer by HPV test in a population-based demonstration programme in eastern India. Trained health workers used a soft brush to collect cervical samples, which were transported to the laboratory in the Specimen Transport Medium (STM™, QIAGEN, Gaithersburg, USA). HPV DNA status for thirteen high-risk types (types 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59 and 68) was determined by the HC2 high-risk HPV DNA Test.
HC2 is a nucleic acid hybridization assay with signal amplification that utilizes micro-plate chemiluminiscent detection technique. The intensity of light emitted after signal amplification is measured as relative light units (RLU), which denote the presence or absence of target DNA in the specimen. For each specimen, an RLU/cut-off (RLU/CO) value is calculated as the ratio of the specimen luminescence relative to the luminescence of the 1.0 pg/ml HPV-16 cut-off standard. The RLU/CO value reflects a semi-quantitative estimation of the cumulative viral burden from one or more of the thirteen oncogenic HPV genotypes in the specimen. In our study, women with an HC2 test RLU/CO value of ≥1.0 (signifying at least 5000 viral copies in the sample) were considered positive.
HPV positive women were recalled for colposcopy. Cervical punch biopsies were obtained from all of these women, irrespective of colposcopy findings. Colposcopy was also performed on the HPV negative women who were symptomatic, had visible cervical abnormality, or were positive on other screening tests. Biopsies were obtained in these women only if colposcopy suggested low grade lesions or worse.
The HC2 test and histopathology reporting were performend at Chittaranjan National Cancer Institute (CNCI). All the women provided written informed consent prior to participating in the study. The Human Research Ethics Committee of CNCI approved the study protocol.
HC2 positive women were classified according to the log-range scale definition of viral load suggested by Lorincz et al. 2 We considered RLU/CO values of 1.0 - <10.0 to be low positive, 10.0 to <100.0 intermediate, and 100.0 or more as high viral loads. The distribution of the RLU/CO values by age, menopausal status, and final diagnosis was presented as proportions. The distribution of final diagnosis and the combined colposcopy findings and RLU/CO values were also presented as proportions. The effect of RLU/CO values and combined colposcopy findings and RLU/CO values on the final diagnosis was assessed using logistic regression models. The crude and age adjusted regression analyses are presented using odds ratios (ORs) and their 95% confidence intervals (CIs). Receiver operating characteristic (ROC) curves were obtained to assess the performance of HC2 in detecting CIN 2 or worse (CIN 2+) and CIN 3 or worse (CIN 3+) at different positivity thresholds. Linear weighted kappa values were estimated to assess the strength of agreement between colposcopy and histology diagnoses. All statistical analyses were carried out using Stata version 12 software (STATA Corp, Texas, USA)
Results
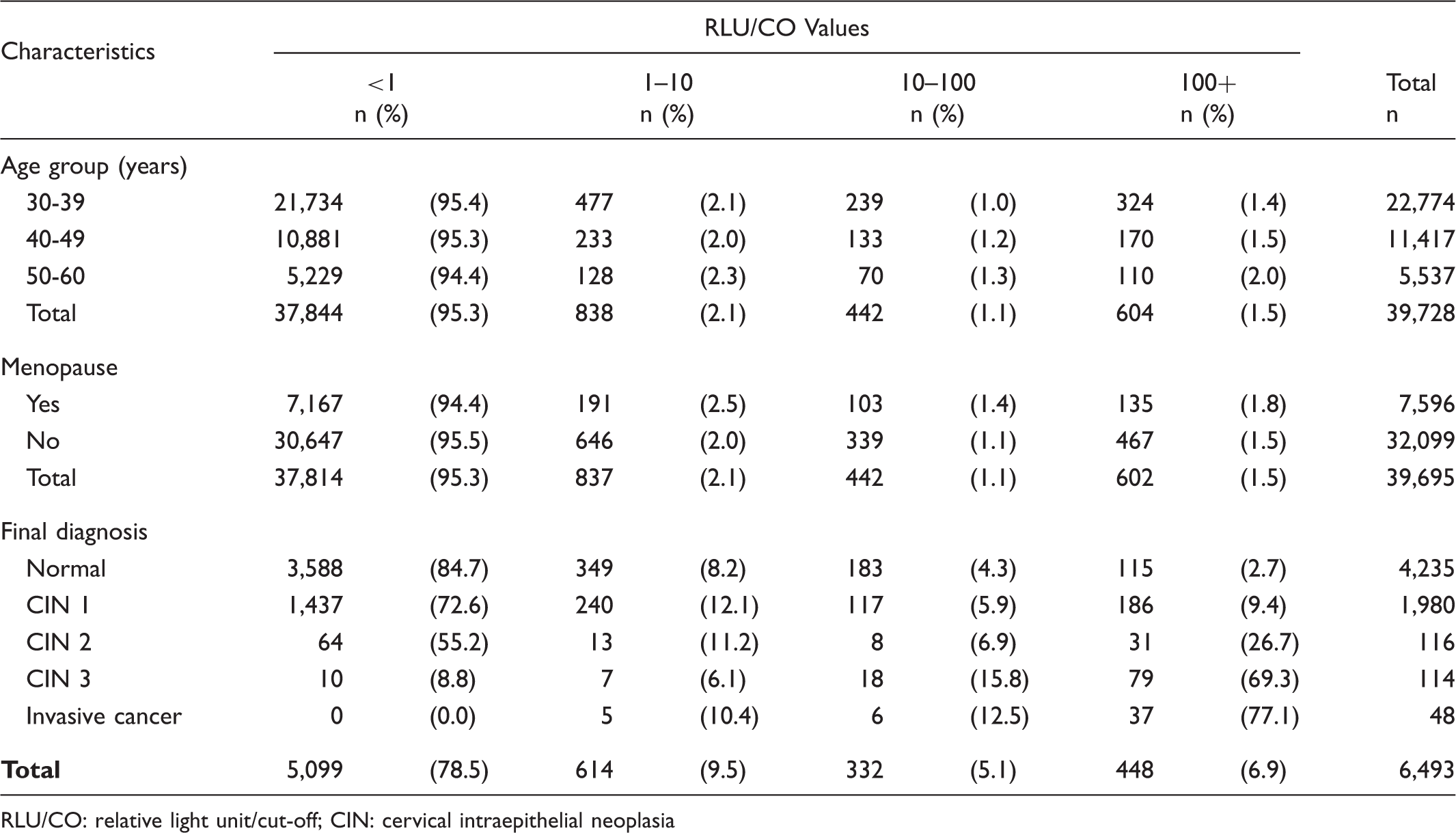
Between April 2010 and August 2014 39,728 women were screened by HC2; 1884 (4.7%) tested positive. The subsequent diagnostic procedures (colposcopy and/or biopsy) performed in these two groups are shown in Figure 1. Among the HPV positive women, 838 (44.5%) were in the low positive (RLU/CO = 1 - <10), 442 (23.5%) in the intermediate (RLU/CO = 10 - <100), and 604 (32.0%) in the high (RLU/CO = > 100) categories of viral load. There was no significant difference in the distribution of viral load either by age groups (X2 = 3.3, d.f. 4; p = 0.50) or menopausal status (X2 = 0.112; d.f. 2; p = 0.94) (see Table 1).
Flowchart of the diagnostic work up of screen positive and screen negative women. Distribution of viral load estimated as RLU/CO values by characteristics of the women. RLU/CO: relative light unit/cut-off; CIN: cervical intraepithelial neoplasia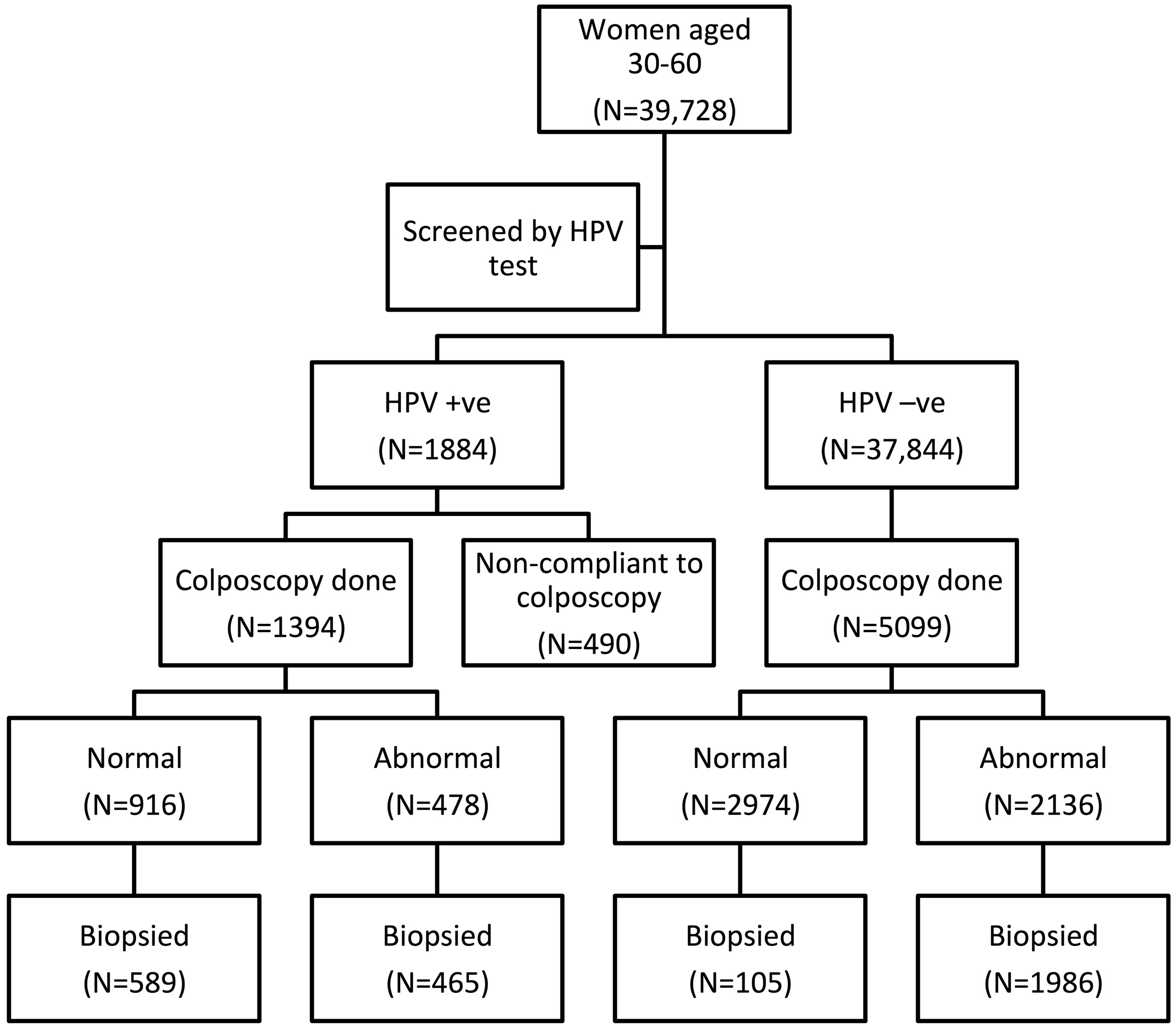
Colposcopy was performed on 1394 HPV positive and 5099 HPV negative women; 3145 had satisfactory histology reports. In the entire cohort of screened women, 116 CIN 2, 114 CIN 3, and 48 invasive cancers were diagnosed on histology. The final diagnosis of ‘normal’ cervix was based on histology or colposcopy, if histology was unavailable. The sensitivity and specificity of HC2 to detect CIN 3 or worse lesions, after adjusting for verification bias, were 91.2% and 96.9% respectively, (for details see our earlier publication). 10
The ROC curve analysis was performed using different HPV positivity cutoffs to detect CIN 2 or worse (CIN 2+) and CIN 3 or worse (CIN 3+)(see Figure 2). The manufacturer’s recommended RLU/cut-off of 1.0 had the best combination of sensitivity and specificity to detect CIN 2+ or CIN 3+.
Receiver operating characteristics (ROC) curve analysis using different HPV positivity cut-offs to detect CIN 2 or worse (CIN 2+) and CIN 3 or worse (CIN 3+).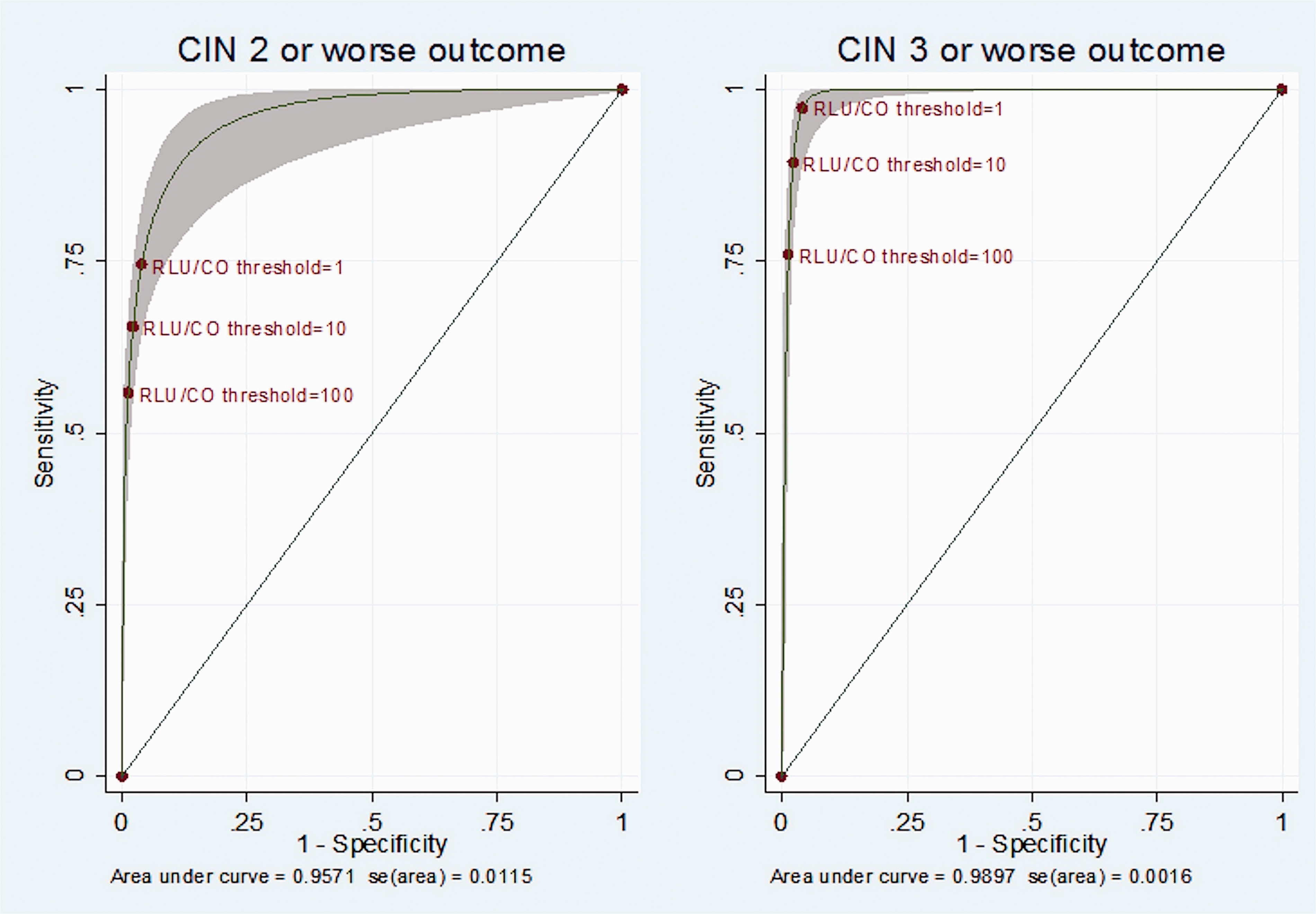
The severity of the disease correlated well with rising viral load. The adjusted ORs for CIN 3 diagnosis in women with low positive, intermediate, and high viral loads were 7.0, 34.2, and 236.8 respectively (p for trend <0.001) compared with the HPV negative women. The positive predictive values (PPV) of the HPV test increased simultaneously with higher cut-off values. The PPV of low positive and intermediate viral loads to detect CIN 2+ lesions were 4.1% and 9.6% respectively, and sharply increased to 32.8% in the women with high viral load.
Final diagnosis by combined colposcopy diagnosis and estimated viral load.
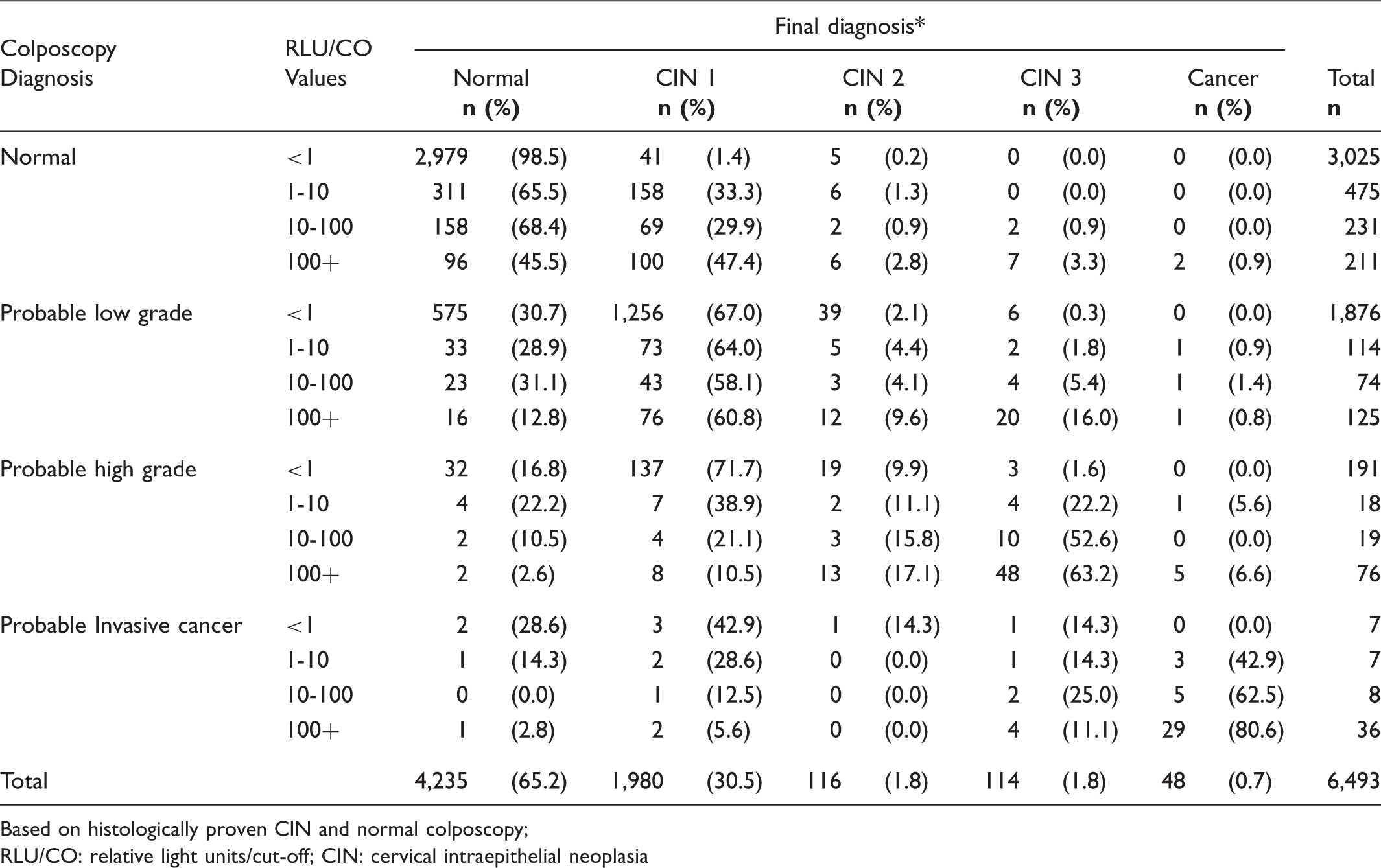
Based on histologically proven CIN and normal colposcopy;
RLU/CO: relative light units/cut-off; CIN: cervical intraepithelial neoplasia
Effect of combined colposcopy diagnosis and viral load on CIN 2 or worse lesions.
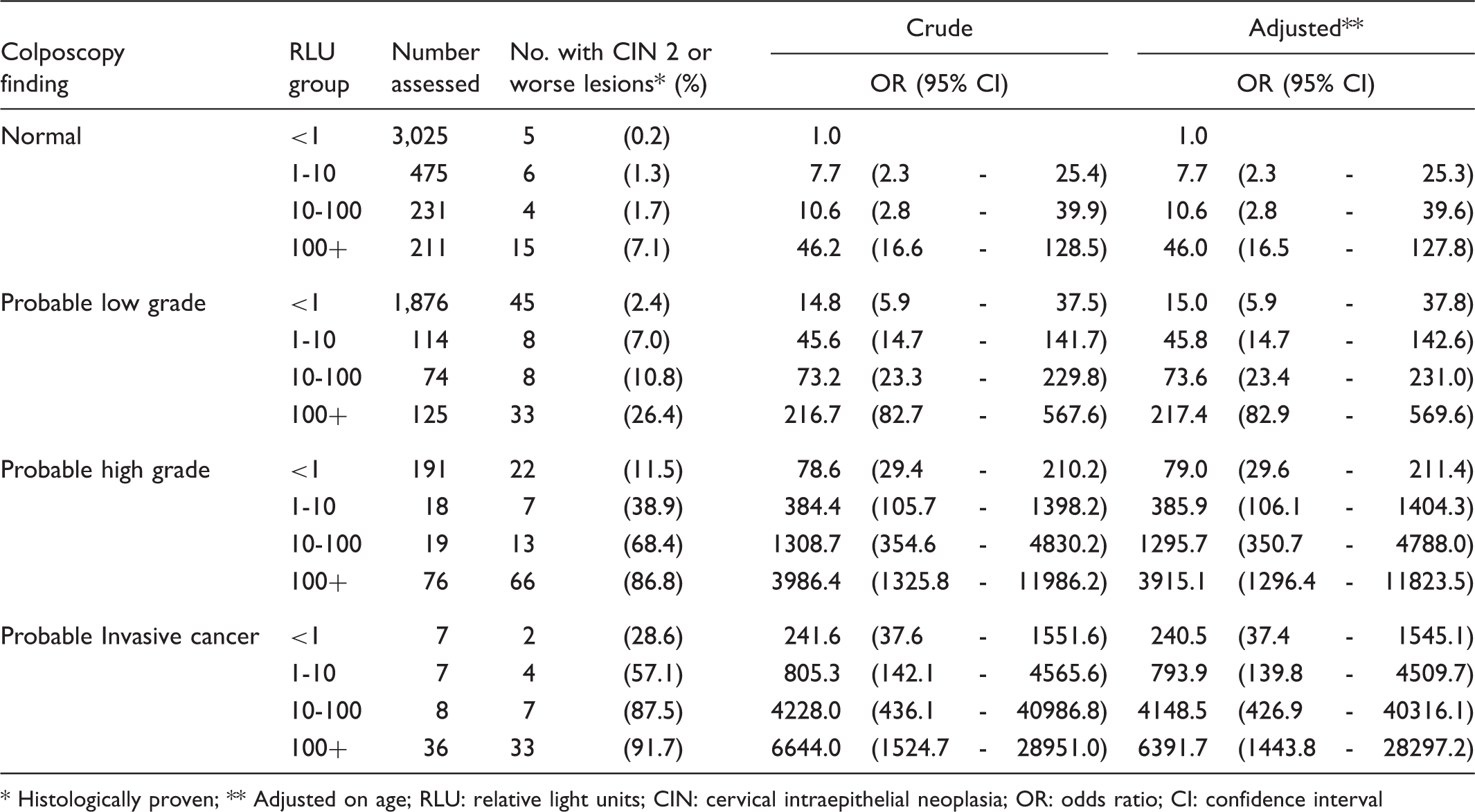
Histologically proven; ** Adjusted on age; RLU: relative light units; CIN: cervical intraepithelial neoplasia; OR: odds ratio; CI: confidence interval
Discussion
HC2 was originally developed as a qualitative test to detect the presence of any of the 13 commonest HPV types for cervical cancer screening. Because the HC2 assay result is reported as a semi-quantitative value, the crude viral load can also be measured by the test. Several studies assessing the risk of cervical neoplasias with various levels of viral load estimated by HC2 have attempted to refine the specificity of the test using higher cut-offs for positive tests.11-13 Outcomes of the studies varied due to different study populations and methodologies. The originally recommended RLU cut-off of 1.0 for test positivity gives the best combination of sensitivity and specificity, though some authors still recommend using a higher threshold (of 2 or even 4) to improve the specificity of HC2. 14
Our results indicate that the strong correlation between the viral load estimations by HC2 and higher grades of cervical neoplasias can be used to improve the detection of high grade lesions, if HPV test positive women are triaged by colposcopy.
Traditionally, cytology and colposcopy results have been used collectively for the management of women with suspected lower genital tract neoplasias. Colposcopy performed on women with abnormal cytology has the advantage that cytology provides some indication of the degree of abnormality and the tissue diagnosis to be expected. 15 Even so, there is significant under-diagnosis of high grade lesions, including CIN 3, especially if lesions are small.16,17 A meta-analysis of studies from 1960 to 1996 estimated the sensitivity of colposcopy in detecting CIN3 as ranging from 54 to 85%, even though most colposcopies were performed on cytology positive women in these studies. 18 Colposcopy is more challenging and is reported to perform sub-optimally in non-cytology-based programmes. We also observed this in our study. Colposcopy can both over-diagnose and under-diagnose lesions in HPV positive women. 19
Another limitation of colposcopy triage of HPV positive women is that the recommendations for further diagnostic work up and management are not as well defined as they are for triaging cytology-positive women. In the presence of any grade of cytological abnormality, punch biopsies are recommended if any atypical features are seen on the transformation zone on colposcopy. If cytology is persistently abnormal, the transformation zone should be excised, even if colposcopy is normal. Lesions extending inside the canal, or the non-visualization of the squamo-columnar junction (SCJ) in presence of high grade cytology are other indications for excision biopsies.
No standard protocols are currently available for colposcopy triage to evaluate the HPV positive women, as all positive women are expected to have cytology triaging. HPV testing will be used increasingly as a primary screening test in many settings where high quality cytology is not available for triaging. There is an urgent need to standardize the indications for punch biopsies or excisional biopsies in HPV positive women in special situations, such as normal colposcopy in presence of repeatedly positive HPV test, low grade abnormalities on colposcopy, non-visualization of the SCJ, or an apparently low grade lesion extending inside the canal.
In our study, as in earlier studies, a number of CIN 2+ lesions were detected by random punch biopsies in colposcopically normal HPV positive women. 20 Yang et al. ascribed this to non-visualization of lesion on colposcopy due to ‘thin CIN’. 21 We observed that most of the missed high grade lesions were due to erosion, inflammatory changes, and small lesion size in the younger women. In the absence of a cytological clue to the expected morphological abnormality, colposcopists encounter a diagnostic pitfall in such conditions.
The results of our study emphasize the importance of considering viral load during decision making in colposcopy. Women with higher RLU/CO on HC2 had significantly elevated risk of harbouring high grade neoplasias, even with normal colposcopy or suspected minor abnormalities only. Of the 25 CIN 2+ cases detected on random biopsies in HPV positive women with apparently normal colposcopy (N = 917), 19 were from the women with RLU/CO values of 10.0 or above (N = 442). CIN 2+ lesions were detected in nearly one third of all the women with high viral load (RLU/CO = > 100.0). In this very high risk group, excision biopsy may be justified if the transformation zone is of type-3 with an apparently low grade lesion extending to the canal, or with no visible lesion. Further evidence is needed on these practical issues to enable specific recommendations to be made.
In cytology-based screening, abnormal cytology with a suspected high grade lesion on colposcopy is a valid indication for treatment, even without histological confirmation (see and treat). In our study, treatment of all colposcopically suspected high grade lesions would have resulted in a 66.5% (202/304) overtreatment rate. This rate would have reduced to 22.1% (21/95) by treating only the suspected high grade lesions with intermediate or high viral loads. Viral load estimation can be a useful adjunct to colposcopy to select cases for ‘see and treat’ in HPV detection based screening.
The principal criticisms of viral load estimation by HC2 are that it is merely a semi-quantitative assessment of the load of a pool of high-risk HPV types, and does not include methods to adjust for difference in the number of cells collected (specimen cellularity). Gravitt et al. studied the direct correlation between the viral loads estimated by HC2 and by HPV 16 RT-PCR. 22 They observed linearity and good correlation between the two assays across the entire dynamic range of values measured. The cellularity in the samples did not influence the estimation of viral load with HC2. Prétet et al. also corroborated that high risk HPV load estimated by HC2 correlate with HPV16 load measured by RT-PCR. 23 In the Taiwan Cooperative Oncology Group (TCOG) study, viral load estimated by RT-PCR to quantify HPV 16, 18, 52, or 58 correlated well with the viral load estimated by HC2. 24 Their multi-centric study also observed good correlation between the tests to determine viral load change (increased or not increased) at baseline, and at six months follow-up, to predict disease progression from low grade to high grade lesions.
Semi-quantitative estimation of viral load by HC2 can be used with colposcopy to select cases for punch biopsies or excisional biopsies, to improve the detection rates of high grade CIN. Viral load estimation can also help to select cases for ‘see and treat’ during colposcopy. The high PPV of RLU/CO cut-off of 10.0 may also justify sending women with viral load above this value directly for colposcopy, if reliable cytology or genotype triaging is not feasible. Further evidence is required to formulate clinical recommendations in favour of these new paradigms.
Footnotes
Acknowledgements
The statistical analysis of data, interpretation of results and the preparation of the draft manuscript describing and discussing the results were undertaken at the International Agency for Research on Cancer, Lyon, France, during an International Cancer Technology Transfer Fellowship award provided by the Union for International Cancer Control (UICC) to Dr. Partha Basu. The demonstration project was partially supported by funds provided by QIAGEN, India, to the Chittaranjan National Cancer Institute, Kolkata, India. The funding agency did not have any role in the conduct of the study, data analysis and preparation of the manuscript. Dr. Partha Basu completed this work when he was on staff at Chittaranjan National Cancer Institute, Kolkata, India.
Disclosure of conflict of interest
None to declare.