
Abstract
Objective
Cytological screening for anal cancer precursors is not always possible. We investigated digital ano-rectal examination (DARE) as a means of early anal cancer detection in HIV-positive men who have sex with men (MSM).
Methods
We recruited 327 HIV-positive MSM aged 35 and over from clinics with HIV physicians in Melbourne, Australia, to receive an annual DARE. We analyzed baseline data from patient questionnaires regarding general, anal and sexual health, adverse effects from the anal examination, cancer worry, and quality of life.
Results
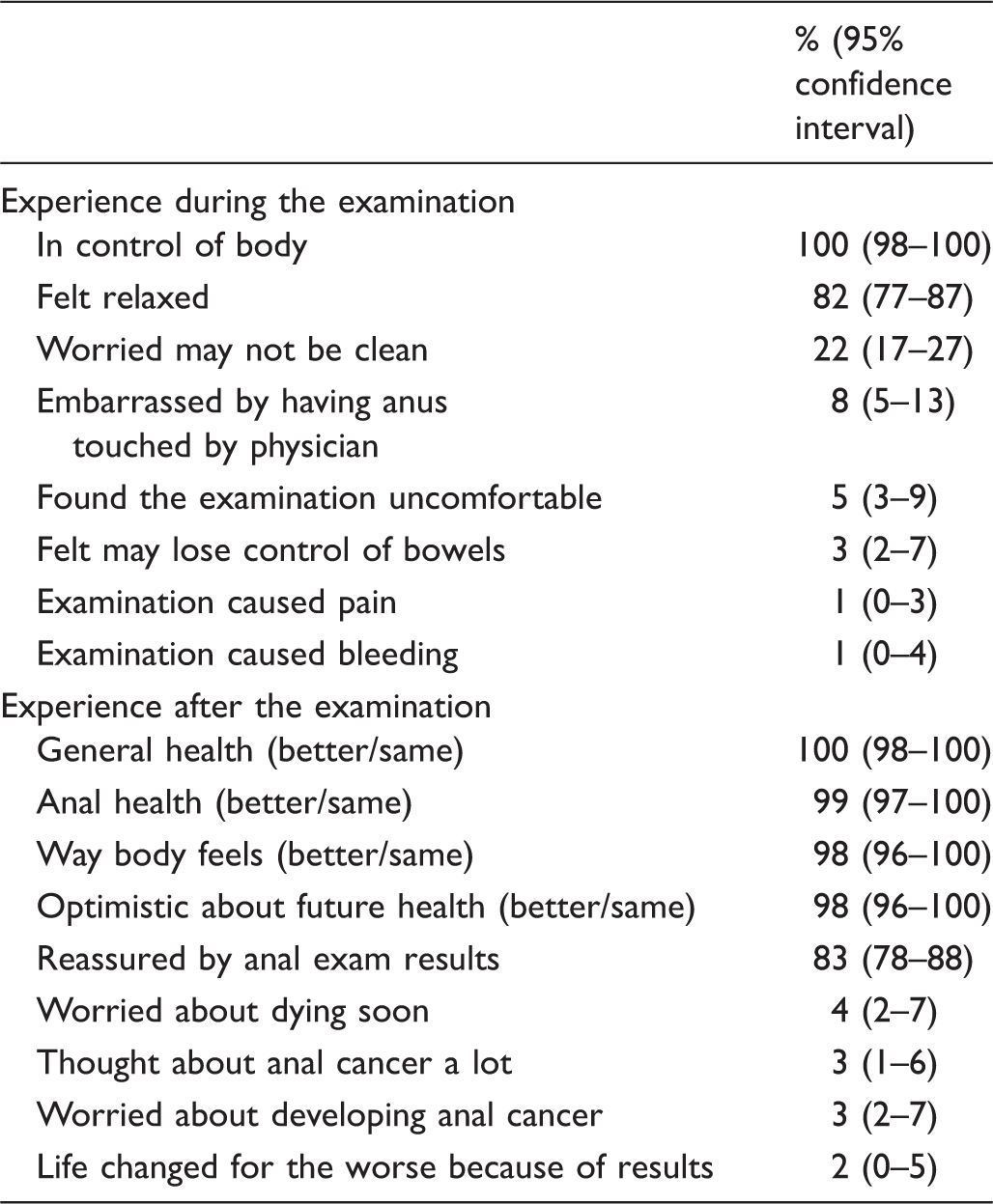
The majority of men (82%, 95% CI:78–87) felt relaxed during the DARE, 1% (95% CI:0–3) complained of pain, and 1% (95% CI:0–4) reported bleeding after the examination. Nearly all men (99%, 95% CI:96–100) were willing to continue with an annual DARE. Quality of life was unaffected with utility scores of 0.76 before examination vs. 0.77 two weeks after examination, (p = 0.41). An anal abnormality was detected in 86 men (27%, 95% CI:22–31), with one anal cancer identified. The specialist referral rate following DARE was 5% (95% CI:3–8). Recruitment rates were significantly associated with the clinic setting (sexual health centre 78%, general practice 13%, hospital 14%, p = 0.002) and specialty (sexual health physician 67%, general practitioner 20%, infectious disease physician 14%, p = 0.031).
Conclusion
Annual DARE to detect anal cancer in HIV-positive MSM was acceptable for patients, with minimal side effects. Strategies to increase HIV physician’s patient recruitment would be needed if DARE were to be implemented in anal cancer screening.
Introduction
Anal cancer is relatively rare in the general population (annual incidence rate 1–2 per 100,000),1,2 but some subpopulations (eg. HIV-positive men who have sex with men [MSM]) have high incidence rates (65–110 per 100,000 person-years), 3 comparable with other common cancers (eg. colorectal and lung) in the general population. 4 Anal cancer is the most common non-AIDS-defining malignancy in those living with HIV in developed countries. 5
Anal cancers are often detected too late for optimal treatment outcomes, with an average size of 2.9 cm at diagnosis in HIV-positive patients. 6 As most anal cancers are visible and/or palpable for some time before definitive diagnosis, 6 screening using regular digital ano-rectal examination (DARE) and peri-anal inspection may detect these cancers earlier, potentially resulting in less morbidity and mortality. A study of 6,411 patients with primary invasive anal cancer showed that cancers less than 2 cm at diagnosis had an 80% 5 year-survival compared with 45–65% when the cancer was more than 2 cm and 20% for cancers that had metastasized. 7 A French series of 69 patients with anal cancers less than 1 cm reported a 100% 5 year survival. 8 Although there may be theoretical advantages of implementing DARE for HIV-positive MSM, it is currently recommended by very few national guidelines, based on expert opinion. 9 DARE’s effectiveness in reducing morbidity and mortality from anal cancer, and the feasibility of its implementation for the proposed screening population remain unclear. 10 To evaluate DARE among HIV-positive MSM in a randomized controlled trial would require an estimated 22,000 patient years of follow up to detect a clinically significant difference in anal cancer detection between those receiving DARE and those not (using incidence rate of 100 per 100,000 and 80% power to detect a 1.5 cm mean difference in tumour size). Given that the reduction in mortality due to cervical cancer screening only became apparent decades after the implementation of the screening programme, 11 we propose that if we can demonstrate minimal harm to patients from an annual DARE, it may be reasonable to implement this screening programme and retrospectively analyze mortality differences between screened and unscreened populations. One study, from a single centre and involving only 102 participants, found 4-monthly DARE to be highly acceptable to HIV-positive MSM. 12 Our current study differs in that it evaluates the acceptability of an annual DARE (4-monthy DAREs are unlikely to be sustainable in the long-term) for a larger number of men, from multiple centres, and will provide quality of life measures of the screened population.
In a recent survey of Australian HIV physicians, 86% (95% CI: 71–95) considered screening for anal cancer to be important. 13 As most HIV patients in Australia see an HIV physician at least annually, we evaluated the feasibility of incorporating DARE into a medical consultation by HIV physicians working in a variety of medical settings (sexual health centre, hospital outpatient clinic, or general practice). Our primary aims were to assess patient uptake and experience of DARE, and to assess the physician’s likelihood of recruiting patients for screening within their clinical setting. Secondary aims were to identify anal abnormalities detected and the specialist referral rates which would have an impact on the costs of this screening.
Methods
HIV-positive MSM aged 35 and over from a sexual health centre, a tertiary hospital HIV outpatient clinic, and two high HIV case load general practices in Victoria, Australia, were eligible to participate in the study. The study rationale and procedures were provided at an education session in each clinic, and individual physicians volunteered to participate. At the time of clinic attendance, eligible men were informed about the project through the recruiting clinician. Posters and brochures of the study were also available in the patient waiting area in each recruiting site. Men expressing interest in the study were given a plain language statement about the study and a consent form to sign. To be included in the study, men must have adequate English and comprehension skills, and be able to give informed consent. Men were excluded if they were already diagnosed with anal cancer. The recruiting centres were compensated $50(AUS) per patient for recruitment and time spent in ensuring completion of questionnaires. Each recruiting centre had an allocated research assistant who reminded physicians (via emails) about the study throughout the recruitment period. Consenting study participants agreed to an annual DARE for two years, ie. three examinations, at baseline, 1, and 2 years. Participants completed four written surveys (paper or online) at baseline, and 2 weeks after each DARE (baseline, 1 year, and 2 years), answering validated questions 12 , 14 regarding general, anal, and sexual health, possible adverse events from DARE, cancer worry, and quality of life measures.
Recruiting physicians received training on how to conduct DARE using a rectal examination model (http://limbsandthings.com/au/products/rectal-examination-trainer-mk-2/) designed for training in detecting prostate cancer, as there were no equivalent training models for anal cancers. During the training, physicians accessed a website (www.anal.org.au/clinician) featuring an educational video explaining the examination, and providing a diagnostic flowchart and extensive library of photos for common anal conditions. Physicians were encouraged to use this website throughout the study.
To evaluate the DARE recruitment rate, we retrospectively recorded the number of HIV-positive MSM aged 35 and over who presented to each recruitment site for each recruiting physician over the recruitment period (6 months). Physicians completed a baseline questionnaire about their perceived importance of anal cancer screening, confidence in using DARE, in recognizing anal cancer, in managing a potential anal cancer, the current caseload of HIV patients seen, and barriers to implementing DARE in their practice.
We analyzed baseline data containing patient questionnaires from recruitment and two weeks after the first DARE, and the physician questionnaires. Patient demographics and experiences were analyzed descriptively. Five-point responses were collapsed into two categories, either “very much/quite a lot/a fair bit” or “a little/not at all”. 95% confidence intervals were calculated for proportions using the modified Wald method. To test statistical significance between groups, chi-square and Wilcoxon-Mann-Whitney test were used for categorical data, and student’s t-test for normally distributed data. One-way ANOVA was used to determine whether the mean of a dependent variable was the same in more than two unrelated independent groups. We defined ‘high recruiters’ as physicians who recruited above the average rate. All analyses were performed using STATA (StataCorp. 2013. Stata Statistical Software: Release 13. College Station, TX: STatCorp LP). Texts from the freehand box were grouped according to themes. Clinical findings for DARE were abstracted from the medical records by the research nurse and summarized (by JO) according to perianal and intracanal abnormalities.
Quality of life data were analyzed from the short-form health survey(SF-12) which contained 12 validated questions measuring the physical and mental health of an individual. 14 These data were converted to a utility score using the University of Sheffield’s SF-6D classification for describing health. 15 The SF-6D estimates a preference-based single index measure for health using general population values, allowing utility scores to be obtained for generating quality-adjusted life years used in cost-effectiveness studies. A utility score quantifies health-related quality of life between 0 and 1, where 0 equates to death and 1 to perfect health. This is a useful measure as it combines the effects of health interventions into a single index, providing the means to compare across different disease areas.
This research was approved by the Alfred Health Human Ethics Committee (Project 246/12).
Results
Demographics of participants.
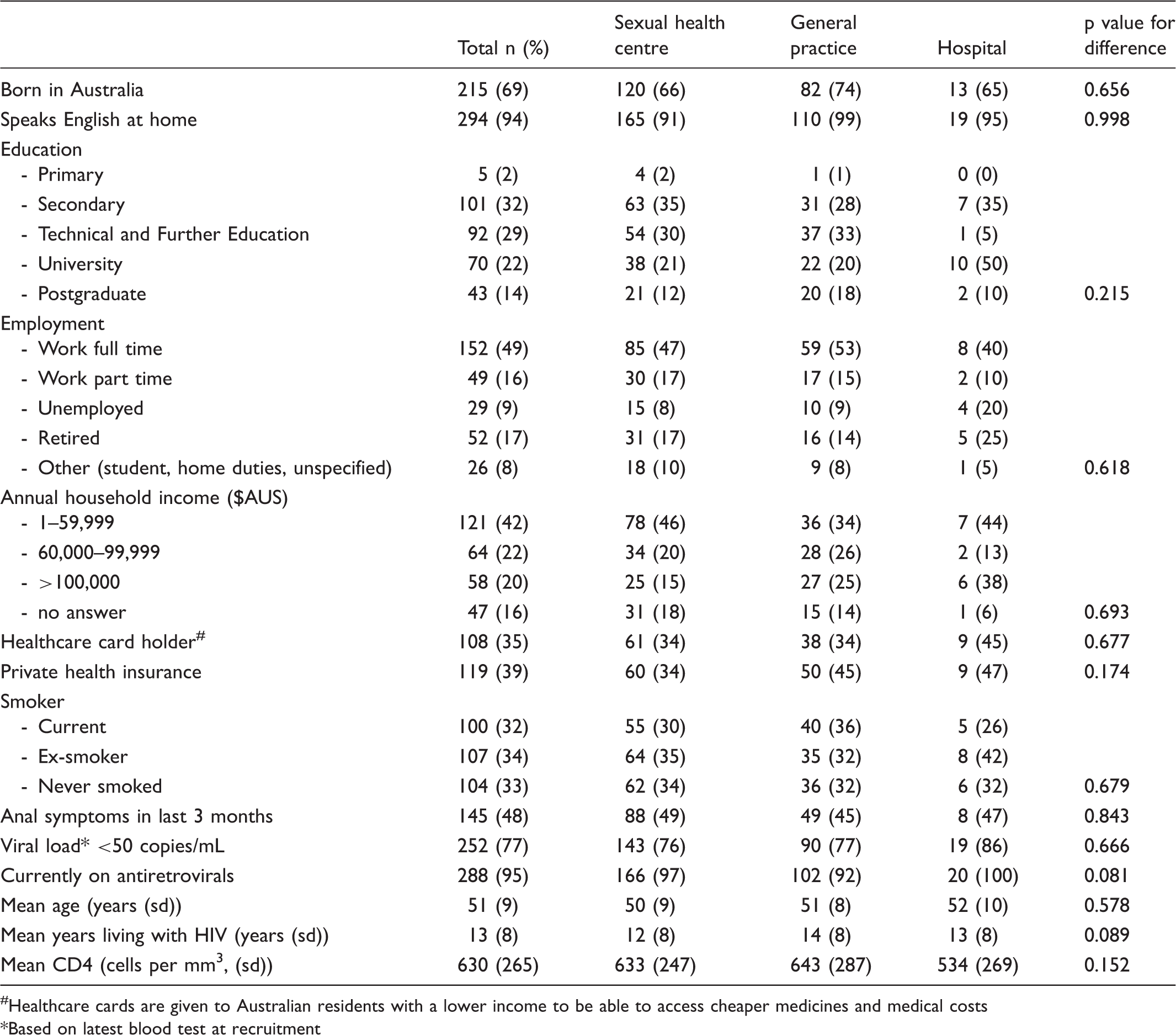
Healthcare cards are given to Australian residents with a lower income to be able to access cheaper medicines and medical costs
Based on latest blood test at recruitment
Number of men who reported anal symptoms within the last 3 months (n = 311)*.
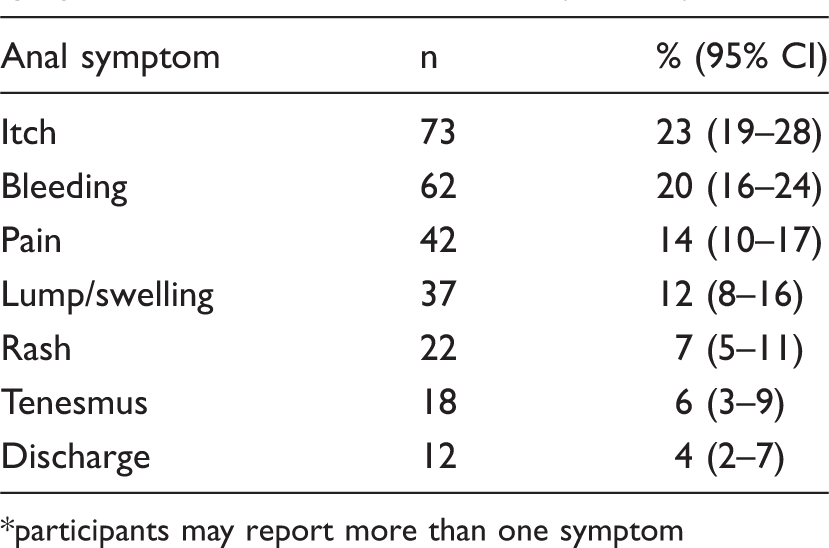
participants may report more than one symptom
Characteristics of HIV physicians according to recruitment site (n = 31).
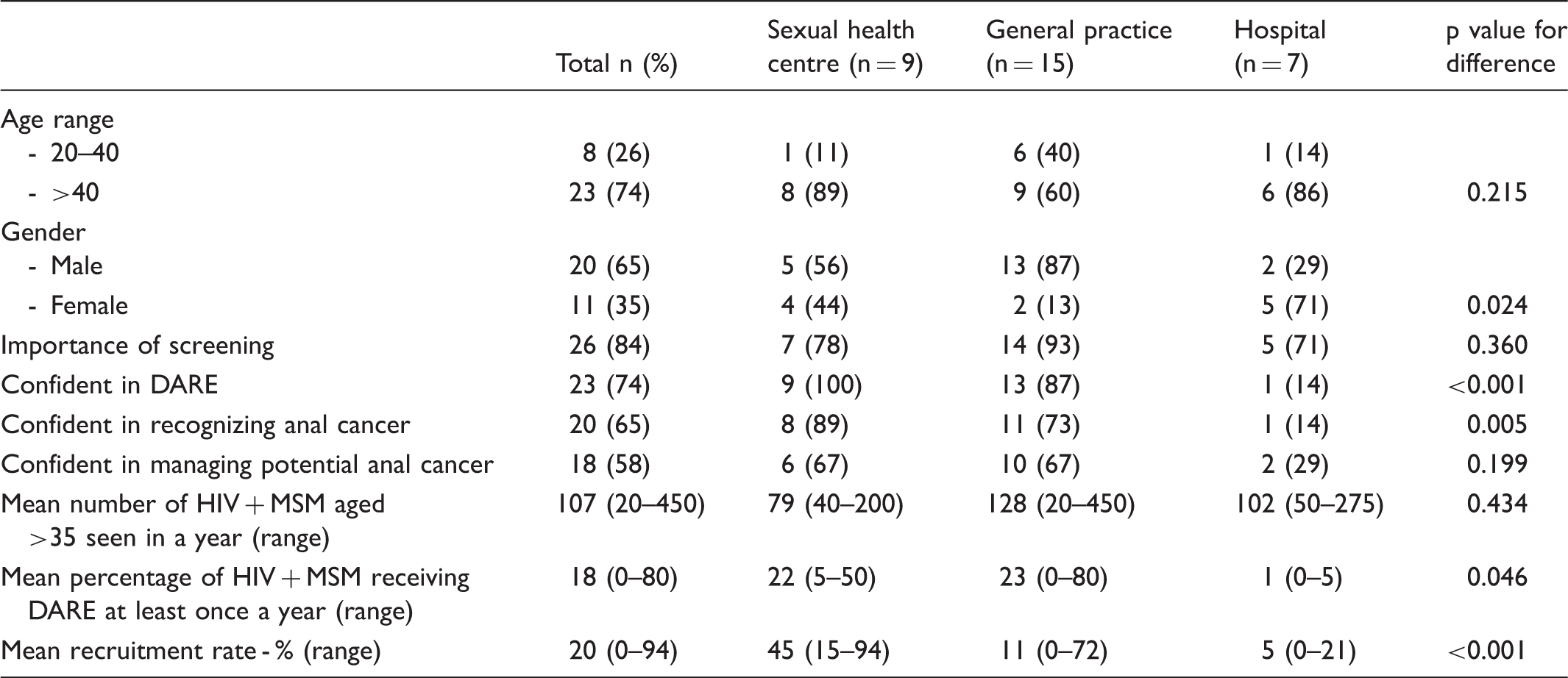
The average recruitment rates by site were sexual health centre 45%, general practice 11%, and hospital 5% (p value for difference < 0.001). Average recruitment rate per clinician was 20%, varying from 0 to 94%. ‘High recruiters’ (those who recruited above the average rate) were significantly associated with the clinic setting (sexual health centre 78%, general practice 13%, hospital 14%, p = 0.002) and specialty (sexual health physician 67%, general practitioner 20%, infectious disease physician 14%, p = 0.031). There were no significant associations between being a high recruiter and the mean age of HIV-positive MSM seen in a year (p = 0.210), physician’s age (p = 0.610) or gender (p = 0.717), or the physician’s confidence in conducting a DARE (p = 0.165), recognizing anal cancer (p = 0.214), or managing a potential anal cancer (p = 0.353). Physicians stated that their main obstacles to anal cancer screening related to lack of time during the consultation (52%, 95% CI: 35–68), a perception that patients may not find DARE acceptable (52%, 95% CI: 35–68), a lack of confidence in utilizing DARE for anal cancer screening (16%, 95% CI: 7–33), and a lack of evidence for screening (16%, 95% CI: 7–33).
Additional data on why men declined to participate were available from the 267 men approached at the sexual health centre. Of these, 187 (70%, 95% CI: 64–76) consented to participate. Of the 80 men who declined to join the study, 48% (95% CI: 36–60) stated they were not interested, 31% (95% CI: 21–43) had no time, and 17% (95% CI: 10–28) had other reasons (will do it next time, overwhelmed with other medical issues, already in another research project, or no reason given). Only 4% (95% CI: 1–11) declined because of anticipated discomfort in receiving the DARE. Similar data were not available from the high HIV case load general practice or the hospital clinic.
Men’s experience of DARE (n = 234).
Examination findings from DARE and visual inspection (n = 325).
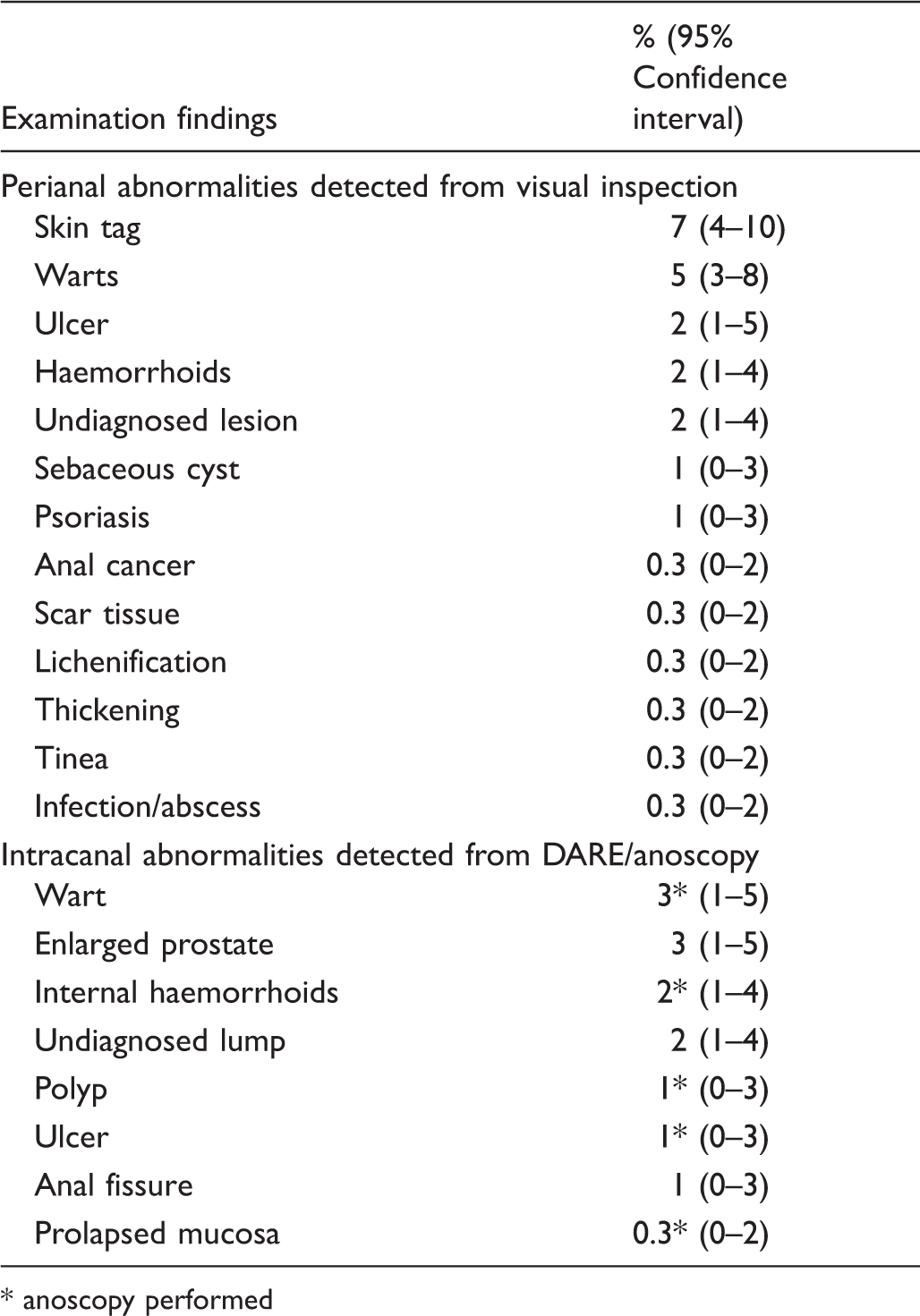
anoscopy performed
Discussion
This study provides data on the experience of enrolling those with highest risk for anal cancer (ie. HIV-positive MSM) into an annual screening programme using DARE. Implementing a DARE was feasible with respect to patient acceptability, minimal psychological and physical harm, and low specialist referral rates. However, we also demonstrated considerable differences between clinical settings in relation to patient recruitment and specialist referral rates. These findings indicate that DARE is likely to be significantly easier to introduce in settings such as sexual health centres where physicians manage more anal conditions. The referral rate, and therefore cost, will be higher, at least initially, in services with limited experience in managing anal conditions (such as infectious diseases departments). This highlights the need for targeted training in conducting an anal examination if high screening coverage is to be achieved, and unnecessary referral and costs are to be contained.
The acceptability of a screening procedure by the screened population is an important criteria in implementing a screening programme. 10 In line with another study evaluating DARE in HIV-positive MSM, 12 we also found DARE to be acceptable with minimal side effects. Almost all (99%) men perceived their general and anal health to be at the same level or better after the examination. Only 1% of men reported pain or bleeding that worried them. It is important to evaluate and monitor psychological health of populations undergoing screening, as adverse psychological impacts due to screening may lead to more harm than benefit. 16 We found that approximately 3% of men reported thinking more about anal cancer, were worried about developing anal cancer, and were worried about dying soon. Half of the men who worried about developing cancer had an anal abnormality detected, but none had anal cancer confirmed. Of those worried about dying soon, none had an anal abnormality detected. Despite this, we found that nearly all (99%) of men were willing to continue receiving an annual DARE as part of their HIV care. The same phenomenon has been observed in women undergoing cervical cancer screening. 17
In our study, the major barrier for implementing an annual DARE related to the physicians, with the average patient recruitment rate of 20%. In contrast, 70% of patients asked to participate in the study accepted. We found significant differences in recruitment rate depending on the recruitment site and specialty, with the sexual health centre and sexual health specialists having the highest recruitment rates. However it is important to acknowledge that low recruitment may also be influenced by other unmeasured factors, eg. patients attending hospital clinics may be co-managed by general practitioners (thus did not accept DARE in the hospital), and other competing priorities (greater complexity of medical issues, other competing research studies). The additional requirements of the study (ie. questionnaires) may have influenced recruitment rates, and it is likely that if patients were offered DARE alone, recruitment rates may be higher. However, the bias towards clinics with more experience in DARE is likely to hold true. Despite these limitations, our study reflects the real-world scenario of the difficulties of introducing a ‘new’ clinical intervention into clinical settings where there are already multiple competing interests for the patient’s and physician’s time. Similar findings were found where, despite a concerted effort to increase anal cancer screening (using DARE with or without anal Pap smear) in an HIV clinic in the USA, only 40% of men received anal cancer screening after two years of the programme. 18 This study, together with our findings, highlights that if anal cancer screening is implemented, strategies to monitor and improve recruitment rates must be addressed. Letters of invitation directly to the patient, mailed educational materials, phone calls, and training activities have been shown to increase breast cancer screening rates, 19 and could be tried in the context of anal cancer screening.
Regularly conducting anal examinations for patients at highest risk for anal cancer has several benefits. Firstly, this may give patients an opportunity to discuss anal issues with their physicians. We found that nearly half of HIV-positive MSM had experienced anal symptoms within the last three months but only 4% had already sought medical attention for the problem. Encouraging physicians to proactively enquire about anal symptoms may also improve the patient’s awareness of early symptoms of anal cancer. One study reported an average of 22 weeks of symptoms before men with anal cancer presented to a health care provider. 6 Furthermore, regularly conducting anal examinations may identify anal pathologies (including anal cancer) in patients reporting no anal symptoms. In our study 61% of men with anal abnormalities detected by their physician reported no symptoms before their examination.
Several issues must be considered in interpreting the data. Firstly, our sample population may not be representative of all HIV-positive MSM, as we chose to recruit patients from the three types of clinical services that HIV patients may visit. Other than the clinic site and specialty of the physician, we were unable to delineate statistically significant differences in physician characteristics (eg. gender, age, confidence of performing a DARE) in relation to the likelihood of recruiting patients for anal cancer screening. A future study with more recruiting physicians would allow further correlational analyses of physician characteristics. This information would be useful for targeting training needs of different groups of HIV physicians. A further issue is that we only collected data on patients who agreed to participate in the study, and the acceptability of DARE may be lower in those who declined. The acceptability of the examination may also differ when repeated. However, the findings of this study (i.e. 99% of men found DARE acceptable), may alleviate fears about DARE being painful or uncomfortable, and may result in higher uptake of screening. We did not measure the impact of the additional requirements of being in a study (reading patient information form, consenting, questionnaires) that may have reduced the recruitment rate of patients.
Conclusion
Conducting an annual DARE for HIV-positive MSM was feasible, with high levels of patient acceptability, no significant harms, and low onward referral rates. However, significant differences in recruitment and referral rates occurred among clinical sites, and specific strategies will be needed to improve patient recruitment rates.
Footnotes
Acknowledgements
The study was funded by an Australian National Health and Medical Research Council Project Grant (568971). We thank all participants of the study and the research coordinators from the various clinical sites – Stuart Cook, Sally Price and Danielle Collins. We also acknowledge the contributions of Marcus Chen, Meredith Temple-Smith, John Kaldor and Sepehr Tabrizi to the study.