
Abstract
Objective
Anal cancer is relatively common amongst HIV positive men who have sex with men (MSM), but little is known about the anal cancer screening practices of HIV physicians, and whether digital ano-rectal examination (DARE) is utilized for this. To determine the practice of anal cancer screening among HIV physicians, and to identify any barriers for implementing DARE as a method for anal cancer screening.
Methods
36 physicians from a sexual health centre, 2 tertiary hospital infectious diseases outpatient clinics, and 2 general practices completed a questionnaire on their practice of anal cancer screening amongst HIV positive MSM. Physicians were asked about their confidence in using DARE for anal cancer screening, and whether they perceived barriers to implementing this in their clinic.
Results
Most physicians (86%, 95% CI: 71–95) thought that anal cancer screening was important, but only 22% (95% CI: 10–39) were currently screening. Reasons for not screening were the absence of guidelines (87%, 95% CI: 60–98), lack of time (47%, 95% CI: 30–65), and concern about patient acceptability of DARE (32%, 95% CI: 17–51). Whilst 67% (95% CI: 49–81) of physicians felt confident in performing a DARE, only 22% (95% CI: 10–39) were confident in recognizing anal cancer using DARE.
Conclusion
Although HIV physicians were aware of the need for anal cancer screening among the HIV + MSM population, few were routinely screening. If DARE were to be incorporated into routine HIV care, guidelines recommending screening and up-skilling of HIV physicians to recognize anal cancer are needed.
Keywords
Introduction
Anal cancer is the most common non-AIDS-defining malignancy in those living with HIV in Australia. 1 Although incidence rates are low in the general population, MSM living with HIV are at highest risk for anal cancer, with rates comparable with other malignancies such as colon and prostate cancer. 2 Despite this, there remains little guidance from national professional bodies advising how to screen for anal cancer. Anal cancer screening can be achieved either by detecting early cancers using digital ano-rectal examination (DARE) or precursor lesions (anal squamous intraepithelial lesions) using anal cytology and/or high resolution anoscopy. 3
In Australia, there are only a few places that offer anal cytological services, and it is unknown whether HIV physicians are currently regularly screening using DARE. Potential barriers to implementing screening using DARE alone are unknown. Understanding barriers to implementation is important if DARE screening was to be introduced into routine HIV care. The aim of this study was to determine current attitudes and practice of anal cancer screening in a sample of HIV physicians.
Methods
Physicians from a convenience sample of five sites in Melbourne, Australia, were asked to complete a paper survey. Melbourne Sexual Health Centre is a sexual health clinic with an HIV clinic staffed by sexual health physicians and infectious disease physicians. The Alfred Hospital and Monash Medical Centre are major urban tertiary hospitals with HIV outpatient clinics staffed by infectious disease physicians. Prahran Market Clinic and Centre Clinic are metropolitan primary care clinics staffed by specialized HIV trained general practitioners. In Victoria, there are 5750 people living with HIV 4 , more than half of whom are cared for by the centres included in this study.
Survey instrument
The survey included questions on the physician’s specialty, age, gender, and number of HIV positive MSM patients seen in a week and in a year. Attitude towards anal cancer screening was determined using a Likert scales for: “How important do you feel it is to screen for anal cancer in HIV positive MSM?” and confidence of performing DARE and anoscopy, recognizing an anal cancer using DARE, and managing a lesion which may be an early cancer. Barriers for implementing DARE were determined by free text.
Statistics
Descriptive statistics were performed using Minitab (v. 16.1.0). Survey responses among the three groups of clinicians were compared using chi square and student’s t test.
Results
Forty-two questionnaires were distributed, with a response rate of 86%; 8 of 8 sexual health physicians, 14 of 16 general practitioners, and 14 of 18 infectious disease physicians completed the survey. Fifty-eight percent of physicians surveyed were male.
Current practice of anal cancer screening in Victoria
Although the majority (86%) of physicians said it was ‘important’ or ‘very important’ to screen for anal cancer, only 22% were currently screening for anal cancer. Of the eight physicians currently screening, three performed annual external examination only, and five used DARE. Of those using DARE, three performed it annually, one 2-yearly, and one ‘occasionally’. Of the three physicians performing annual DARE, only 80, 50 and 10% of their patients actually received DARE annually. Populations targeted for screening included ‘HIV + MSM’ (no age range given), ‘older HIV + MSM’, ‘>40 year old HIV + MSM’, and ‘HIV + males’.
Most physicians (87%) did not screen, stating lack of guidelines as their reason. The main barrier to screening was lack of time and uncertainty of the acceptability to patients (Box 1).
Experience of DARE
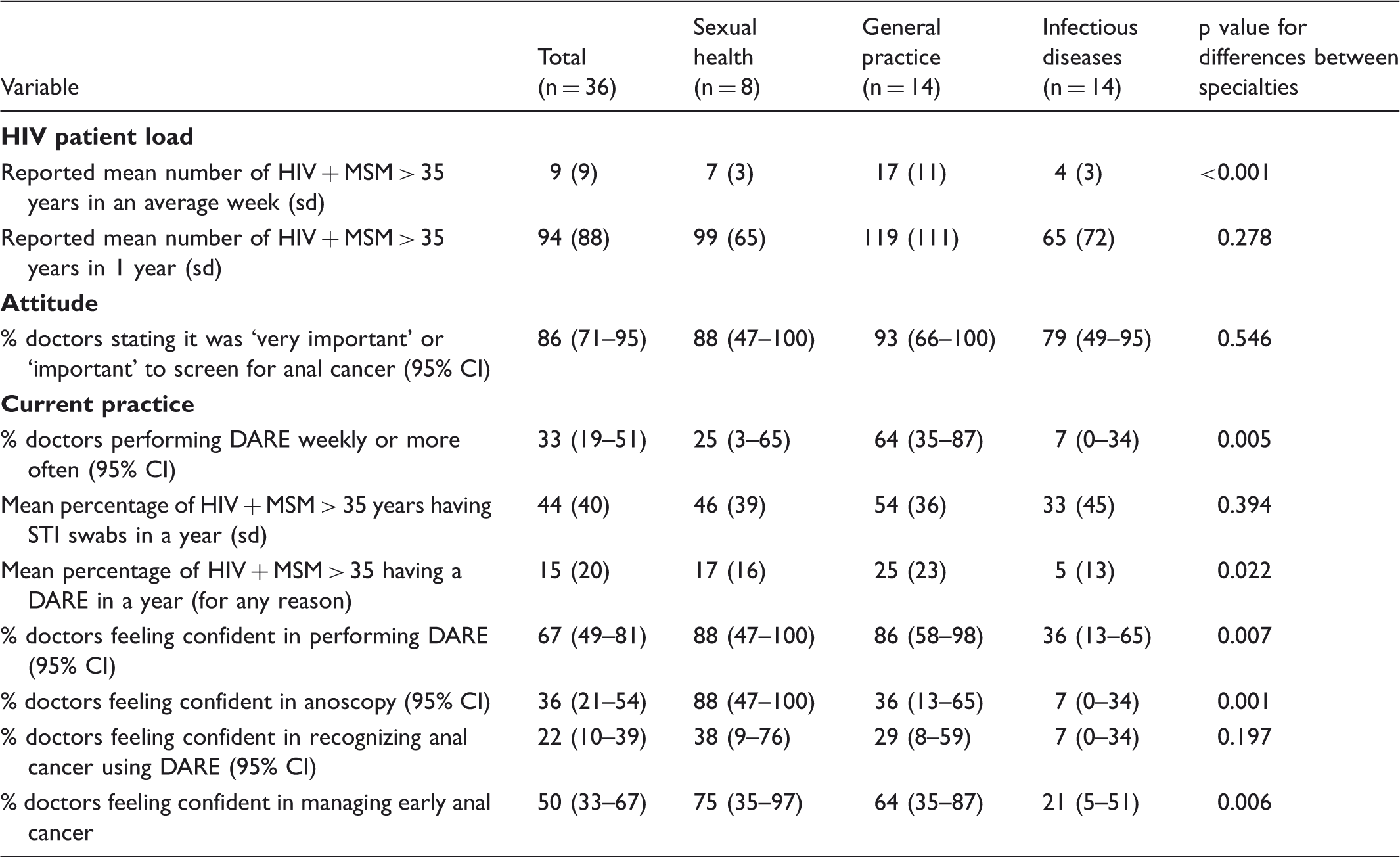
One third of physicians reported performing at least one DARE per week on any patient. The group reporting most DAREs was the general practitioner group (64%) and the group reporting least DAREs, the infectious disease physicians (7%).
Physicians reported that an average of 15% of HIV positive MSM in their practice had a DARE for any reason in a year. However nearly half (44%) of HIV patients would have an annual anal swab for detection of sexually transmitted infections, with the majority of these being patient self-collected. Whilst the majority (67%) of physicians stated that they were confident in performing a DARE, only a minority (22%) stated confidence in using DARE to detect an anal cancer.
Discussion
Despite anal cancer being perceived as important by the majority of HIV physicians, few are currently regularly screening for it using DARE. The main barriers identified were lack of guidelines recommending that it should occur, perceived lack of time, and uncertainty regarding patient acceptability. This finding of low rates of anal cancer screening using DARE was consistent with a Canadian HIV study, where only 10% of patients received anal cancer screening by DARE and/or cytology. 5
Doctor’s HIV patient load, attitude towards anal cancer screening and current practice according to specialty.
This is the first study to specifically evaluate the practicalities of using DARE as a method of anal cancer screening among HIV physicians. The barriers identified in this paper, and the significant differences between the specialties, may aid the education and training information needed if DARE were to be incorporated into anal routine HIV care. A limitation of the study is the small sample size. Future studies could include HIV physicians from other states, to increase the study power to delineate differences according to physician specialty, HIV experience, gender and age.
Conclusion
Reasons for not screening and barriers for screening.
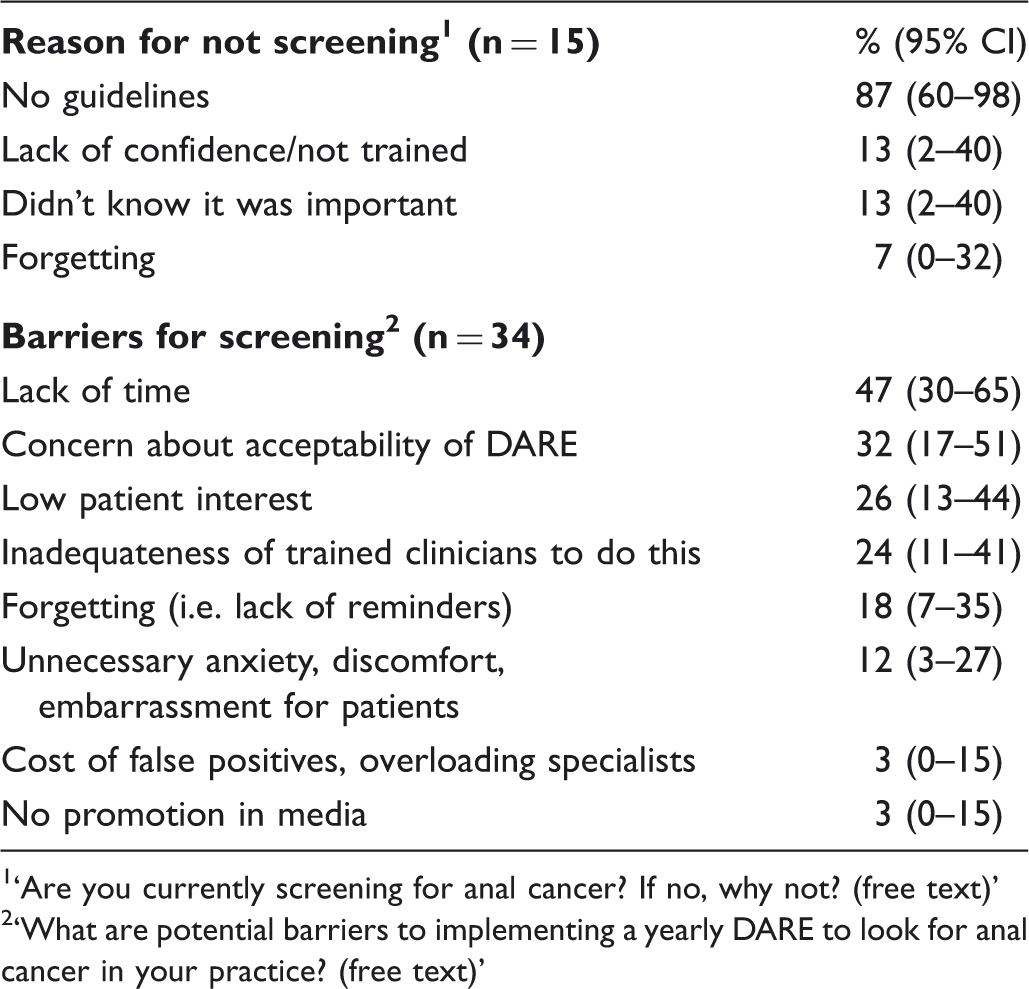
‘Are you currently screening for anal cancer? If no, why not? (free text)’
‘What are potential barriers to implementing a yearly DARE to look for anal cancer in your practice? (free text)’
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.