
Abstract
Objectives
To describe trends in breast cancer mortality in 14 Italian regions representing 90% of the Italian population, and in the country overall, in relation to the diffusion of organized or opportunistic breast cancer screening programmes.
Methods
Estimated annual percent change (EAPC) was calculated for three time-periods (1980–1989, 1990–1999, 2000–2008). To estimate the age-adjusted and age-specific EAPC, trends in mortality based on annual data were examined using a log-linear regression model, and the year of death as a regressor variable.
Results
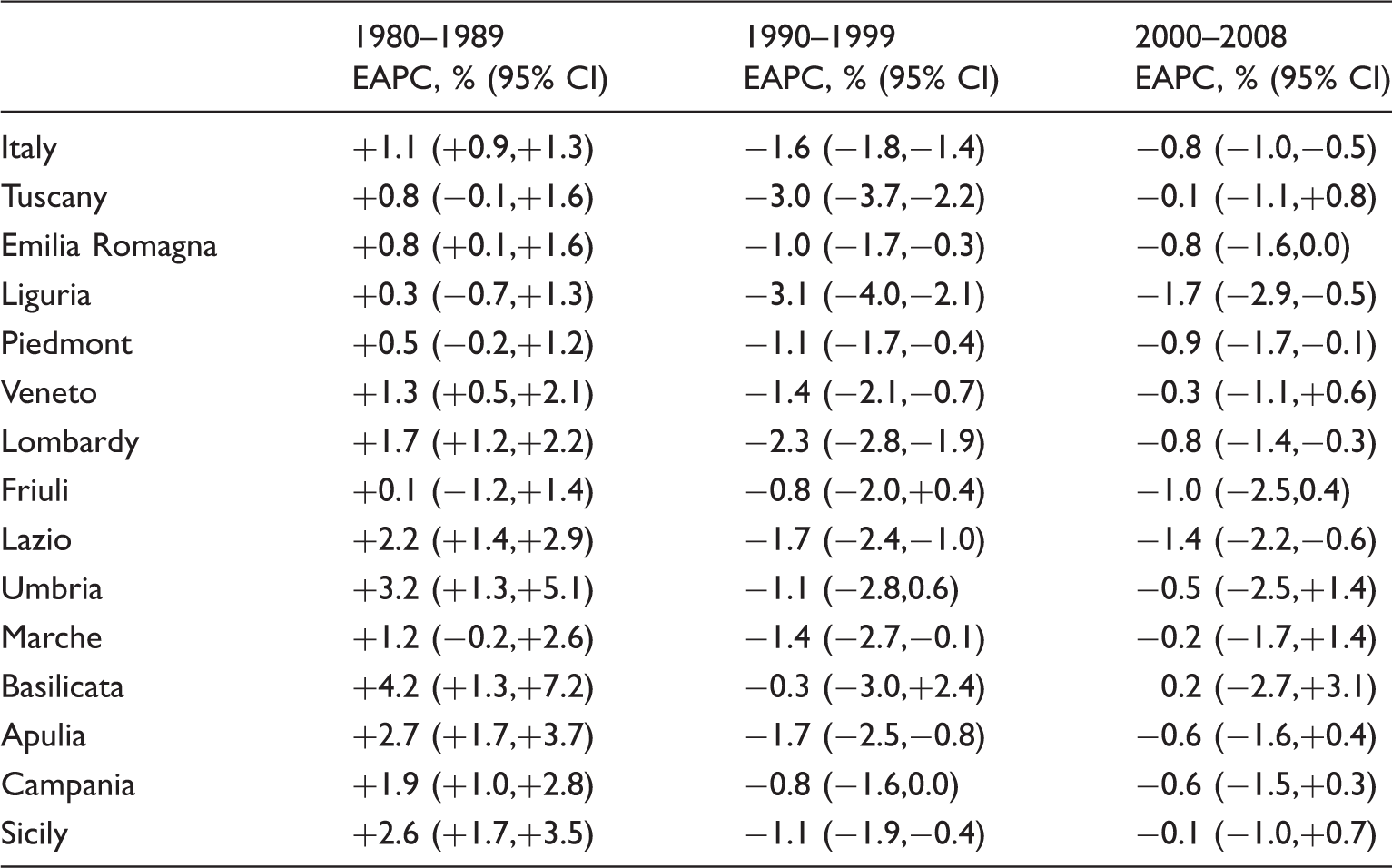
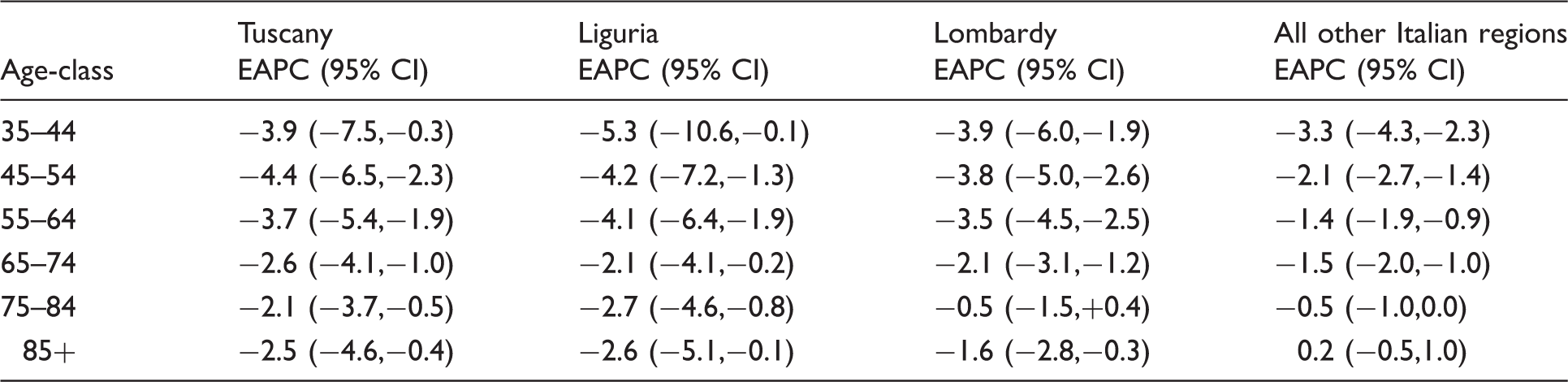
In the period 1980–1989 an increasing trend was observed in Italy overall (EAPC = +1.1%; 95% confidence interval [95%CI]: + 0.9%; + 1.3%) and in the 14 regions. In the second decade a decreasing trend was recorded both overall in Italy (EAPC = −1.6%; 95CI:−1.8%;−1.4%) and in all the regions. Between 2000–2008 a slightly decreasing trend was observed in Italy overall (EAPC = −0.8%; 95%CI:−1.0%;−0.5%). A steeper and earlier decrease compared with the rest of Italy was observed in 1990–1999 in Liguria (EAPC = −3.1%; 95%CI:−4.0%,−2.1%), Lombardy (EAPC = −2.3%; 95%CI:−2.8%;−1.9%), and Tuscany (EAPC = −3.0%; 95%CI:−3.7%;−2.2%), mainly due to the 55–64 age−group. There were significant EAPCs between −4.1% and −3.7% in these three regions, 2.5–3.0 times greater than in the rest of Italy (EAPC = −1.4%).
Conclusions
This earlier decline in three Italian regions could be partially attributable to local organized screening programmes implemented earlier than in the rest of Italy, and to opportunistic screening that became more common in 1990s.
Introduction
Breast cancer is the leading cause of death and the most common cancer among women, in both economically developed and developing countries, 1 and represents 29% of all cancers in Italian women. 2 In recent years breast cancer mortality rates have levelled or begun to decline in many Western countries. In Europe the age-adjusted mortality rates declined by 6.9% between 2002 and 2006, with the largest falls in northern European countries. 3 We aimed to describe breast cancer mortality trends in Italy as a whole and also in 14 Italian regions, that represent 90% of the Italian population, in relation to the diffusion of organized or opportunistic breast cancer screening programmes.
Methods
Number of deaths for breast cancer, person-years, and crude rates (per 100,000) women, 1980–2008 in Italy overall and by region.
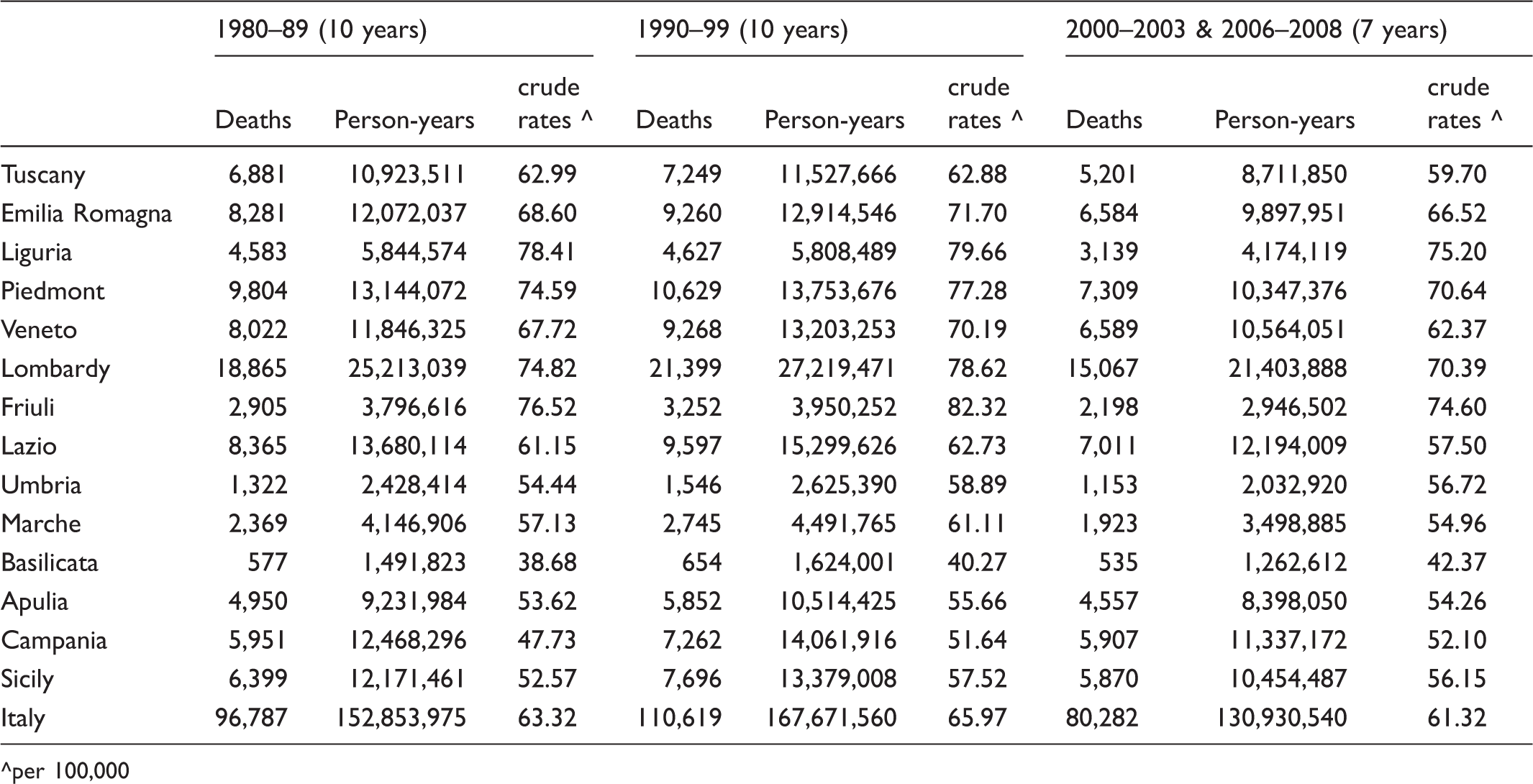
^per 100,000
To calculate the age-adjusted and age-specific Estimated Annual Percent Change (EAPC), trends in mortality based on annual data were examined, using a log-linear regression model, and the year of death as a regressor variable.
Results
Mortality rates for Italy as a whole showed an increasing trend up to 1989, after which rates began to decrease, and then level out after 2000 (Figure 1). A similar trend was observed for the 14 selected regions (Figure 1).
Age-standardized breast cancer mortality rates (x100,000) for the whole Italy and for Lombardy (Northern Italy), Emilia-Romagna, Tuscany (Central Italy), Apulia (Southern Italy).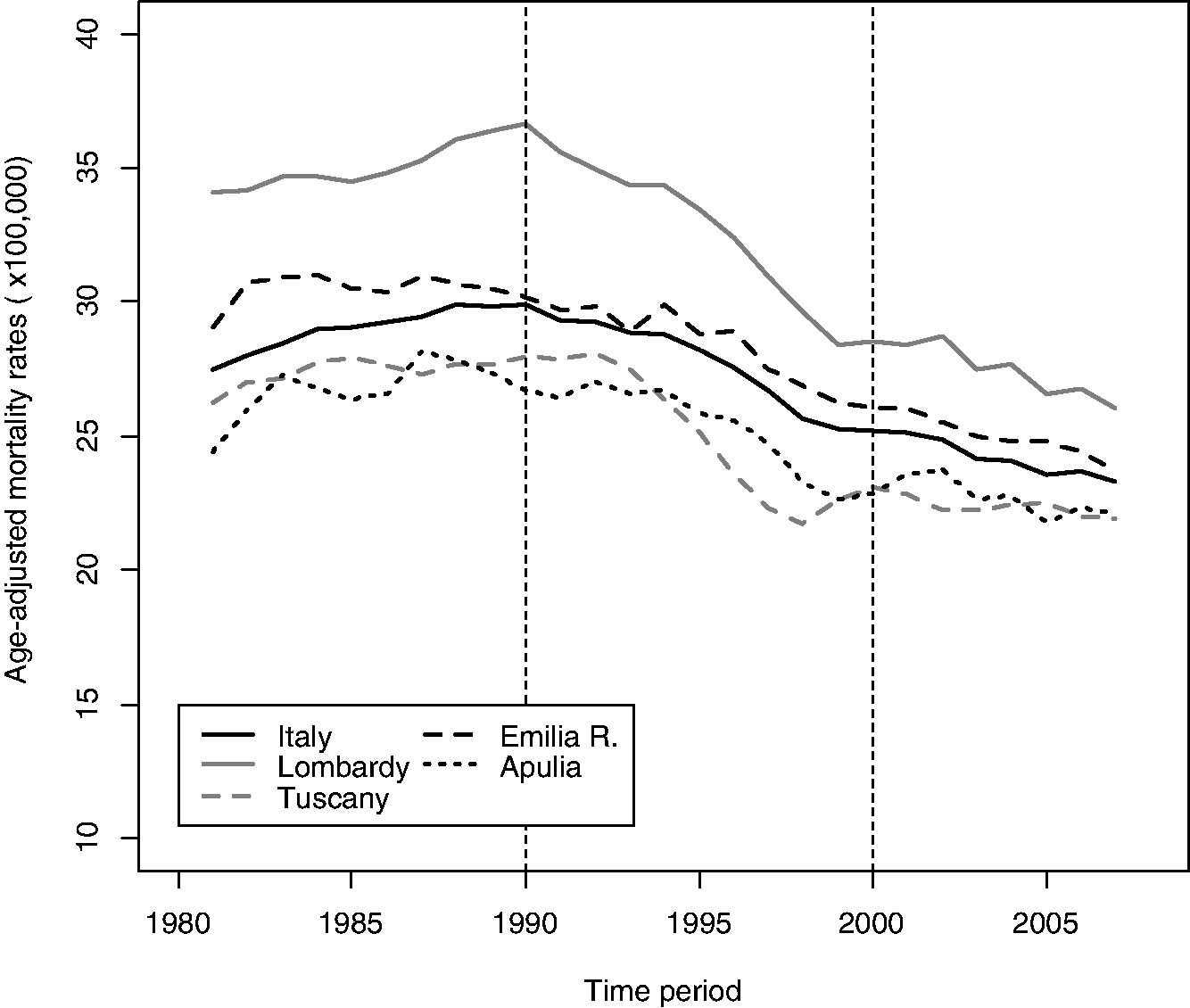
Age-adjusted Estimated Annual Percent Change (EAPC) with 95% confidence intervals for the whole of Italy and by region, for the three decades 1980–1989, 1990–1999, 2000–2008.
The rank of regions in Figure 1 remained much the same from 1980 to 2008: ie. high mortality regions in 1980 were still high mortality regions in 2008, but the magnitude of the difference had decreased. Most of the convergence appeared to have occurred since the late 1990s.
All the selected regions showed similar mortality trends, except for Tuscany, Liguria, and Lombardy, which, in the second decade, showed significantly steeper decreases than those observed in other regions: EAPCs in Tuscany, Liguria, and Lombardy were −3.0% (95% Confidence Interval [95%CI]: −3.7,−2.2), −3.1% (95%CI: −4.0,−2.1), and −2.3% (95%CI: −2.8, −1.9), respectively, in comparison with the rest of Italy (EAPC: −1.0, 95%CI:−1.5,−1.2).
Age-specific (35–74) Estimated Annual Percent Change (EAPC) with 95% confidence intervals for the regions Tuscany, Liguria, and Lombardy, and for the other Italian regions in the decade 1990–1999.
Discussion
Trends in breast cancer mortality rates for the whole of Italy and in the Italian regions were in accord with those observed for Europe, with a peak in mortality in the late 1980s and a decrease thereafter. 3 In the Liguria, Lombardy, and Tuscany regions a steeper and earlier decrease in mortality was observed in the decade from 1990–1999 compared with the rest of Italy, mainly due to the 55–64 age group.
The decline in mortality rates has been attributed both to an increasing frequency of early diagnosis through mammography screening and access to more efficient treatments, including adjuvant chemotherapy or tamoxifen, and improved radiotherapy and surgery.5–11 It has been estimated that less than one-third of the 21.3% decline in mortality of women aged 50–69 (those involved in screening programme) in the United Kingdom in the period 1990–1998 was due to screening, the remainder being due mainly to improved treatment. 12 Another estimate reported that of the 47% reduction in breast cancer mortality recorded in East Anglia (England) after the introduction of service screening, 60% was due to earlier diagnosis, and 40% to innovations in therapy. 13 In the period 1990–2008 in Catalonia, Spain, mortality reduction attributable to screening was 12.7%, to adjuvant treatments 12.4%, and to both interventions 23.7%, showing that 50% of the reduction can be attributed to screening and adjuvant therapy. 14 The estimates of the impact of screening mammography on breast cancer mortality ranged from 10% from regional mortality data 15 to 20% from trial results. 16
In most Italian regions, organized screening programmes in the age group 50–69 began early in the 2000s or sooner. In 23 rural municipalities covering around 20% of the female population in the province of Florence, organized screening started at the beginning of 1970s. 17 Brescia, Lombardy, followed in 1988, and the remainder of the Florence province (about 27% of the Tuscan female population) in 1990. Screening commenced in Turin, Piedmont, in 1992, in Reggio Emilia in 1994 and in the other Emilia-Romagna provinces in 1996–1998. In the Tuscan provinces other than Florence and in most Veneto provinces it started in 1998–2000.17,18
Our results do not exclude the potential contribution of opportunistic screening to mortality reduction. A recent analysis of breast cancer incidence and mortality trends in Europe 19 suggested that mammography screening was widespread even in the absence of organized screening programmes. In some Italian areas during the 1990s opportunistic mammography 20 covered less than 20% of the target population. In 1991 in Emilia-Romagna about 87,660 mammograms were performed within the target population (about 767,553 women aged 45–74), covering 11.4% of the target population [Naldoni C, personal communication], and in Veneto in 1993, about 112,000 mammograms were performed covering around 17% of women aged 40–49 and 5% of women aged 50–69. 21
Most of the convergence of breast cancer mortality rates amongst regions seemed to have happened since the late 1990s (Figure 1), a period that was crucial for the development of organized screening and the introduction of new treatments.
One limitation in our study is that figures are not available for the 1990s in Italy on the use of adjuvant chemotherapy or tamoxifen, or on opportunistic screening. It is, therefore, not possible to draw strong conclusions regarding the relationship between screening onset and decline of breast cancer mortality by region.
Another limitation could be due to the codes of causes of death, as between 1980 and 2008 at least two different revisions of the International Classification of Disease were used to code cause of death. Although coding disparities could cause some variations in rates, they are not likely to compromise the comparability of data over time, because differences between revisions are minor for breast cancer.
Conclusions
Our study showed that in three Italian regions an earlier and steeper decline in breast cancer mortality could be partially attributable to local organized screening programmes implemented earlier than in the rest of Italy, and to opportunistic screening that became more common in 1990s.
Footnotes
Declaration of conflicting interests
None to declare.
Funding
None to declare.
Acknowledgements
We thank Dr. Carlo Naldoni, Department of Public Health, Emilia-Romagna Region, and Dr. Manuel Zorzi, Venetian Tumour Registry for having found figures for the 1990s regarding opportunistic mammography in their regions.