
Abstract
Objective
To evaluate compliance by age, gender, and screening round in the population based Stockholm/Gotland colorectal cancer screening programme.
Methods
All individuals aged between 60 and 69 living in the counties of Stockholm and Gotland (Sweden) have, since 2008, successively been included in a colorectal cancer screening programme using biennial faecal occult blood tests (Hemoccult®). Personal invitations including test kits have been sent to home addresses, and individuals with a positive test result have been called to a defined clinic for an assessment colonoscopy. Descriptive statistics have been used to evaluate different aspects of compliance.
Results
Over the five-year period 2008–2012, more than 200,000 individuals from nine different birth cohorts have been invited, with a compliance rate of approximately 60%, which increased by age, female gender, and subsequent screening round. In total, 4,300 individuals (2.1%) with positive tests were referred to assessment colonoscopy, where 213 colorectal cancers were diagnosed. The compliance with the follow-up colonoscopies varied by year, and ranged from 85.6–92.4%.
Conclusion
The strong organization of the programme contributed to a high compliance rate, that increased by screening round. The lower participation rate among men and among individuals at younger ages needs further attention.
Introduction
Colorectal cancer (CRC) is the third most common cancer in the world, with an increasing incidence, even in countries where incidence was previously low (eg. Asian countries). 1 The natural history of CRC is adequately understood, and there is an early detectable stage where treatment could be offered. 2 The primary purpose of CRC screening is to reduce the disease-specific mortality in the population, but as removal of the precursor stages (adenomatous polyps) has a protective effect against colorectal cancer development,3–5 recent randomized trials of screening with sigmoidoscopy also have demonstrated a decrease in CRC incidence.6–8
In 2003 the Council of the European Union issued recommendations to screen for CRC with faecal occult blood tests (FOBT) in men and women aged 50–74. 9 As a result, national CRC screening programmes with guaiac-based FOBT have started in Europe 10 (eg. in Italy 11 and the UK 12 ). The recommendations were based on the results from three randomized controlled trials demonstrating a net CRC mortality reduction of 16 %,13–15 and were updated in the 2010 European Guidelines for Quality Assurance in CRC screening. 16
In 2006 the Stockholm County Council decided to introduce an organized CRC screening program following a model that successively invited birth cohorts between ages 60 and 69. 17 The primary objective of this study was to evaluate compliance by age, gender, and screening round, during the five years over which the programme has been running.
Methods
The target group of the screening programme comprises all residents in Stockholm County aged 60–69 according to the Swedish population register (updated daily). 18 There are no exclusion criteria. Screening starts at age 60, based on the experience from the United Kingdom, and Finland.12,17 There is the option to expand the programme to a wider age range at a later stage. In 2009 the target group expanded to include the island of Gotland. Two birth cohorts were randomly invited every year to be included in the programme. This enables evaluation of the programme’s effect on CRC mortality.
In 2008 all individuals aged 62 and 66 (ie. born in 1946 and 1942, respectively) were centrally invited, without involvement of primary health care physicians, to participate in the screening programme. A test-kit containing three guaiac-based faecal occult blood tests (gFOBT [Hemoccult®]) and instructions on how to perform the test was sent to the individuals’ homes, with an invitation letter, information on CRC screening, and a prepaid return envelope (Figure 1). Simultaneously, electronic referrals with the individual bar codes to enable registration of results after analysis were sent to the laboratory. People with negative test results (three negative tests) were informed by letter. In the letter, and in order to reduce the risk of false negatives, the individuals were advised to see a doctor if they had any bowel symptoms. Individuals with positive tests (at least one out of three tests positive) were electronically referred to a defined local endoscopy clinic, and offered an assessment colonoscopy within two weeks. Referred individuals then follow the endoscopy clinics’ guidelines regarding bowel preparation and re-call procedures. Individuals with faulty tests were sent new test kits.
Flow chart of the invitation process of the colorectal cancer screening programme of Stockholm/Gotland.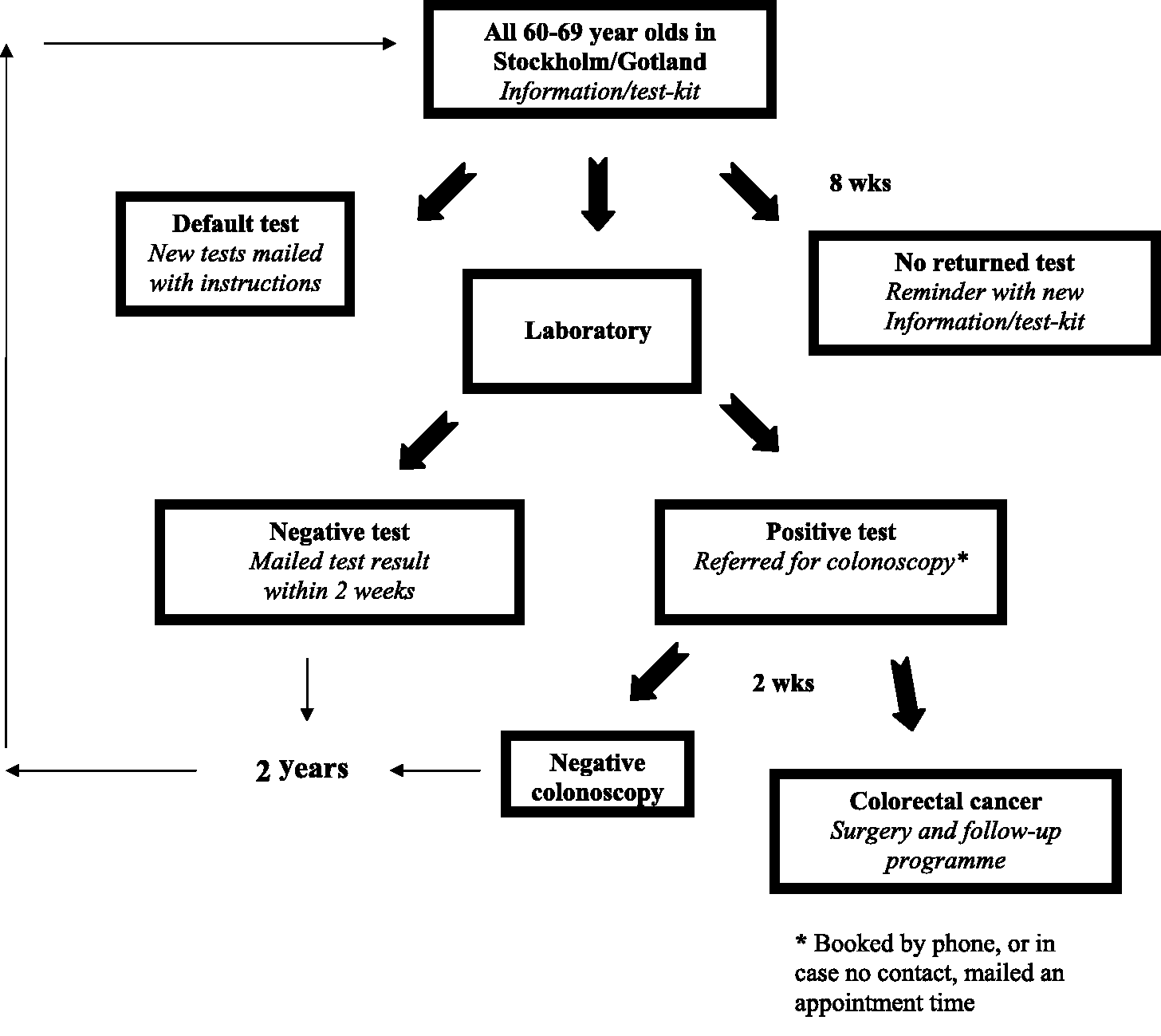
Compliance by invitation year, screening round, and gender among randomized birth cohorts of the general population aged 60–69* invited to biennial Hemoccult® screening in the Stockholm/Gotland programme.
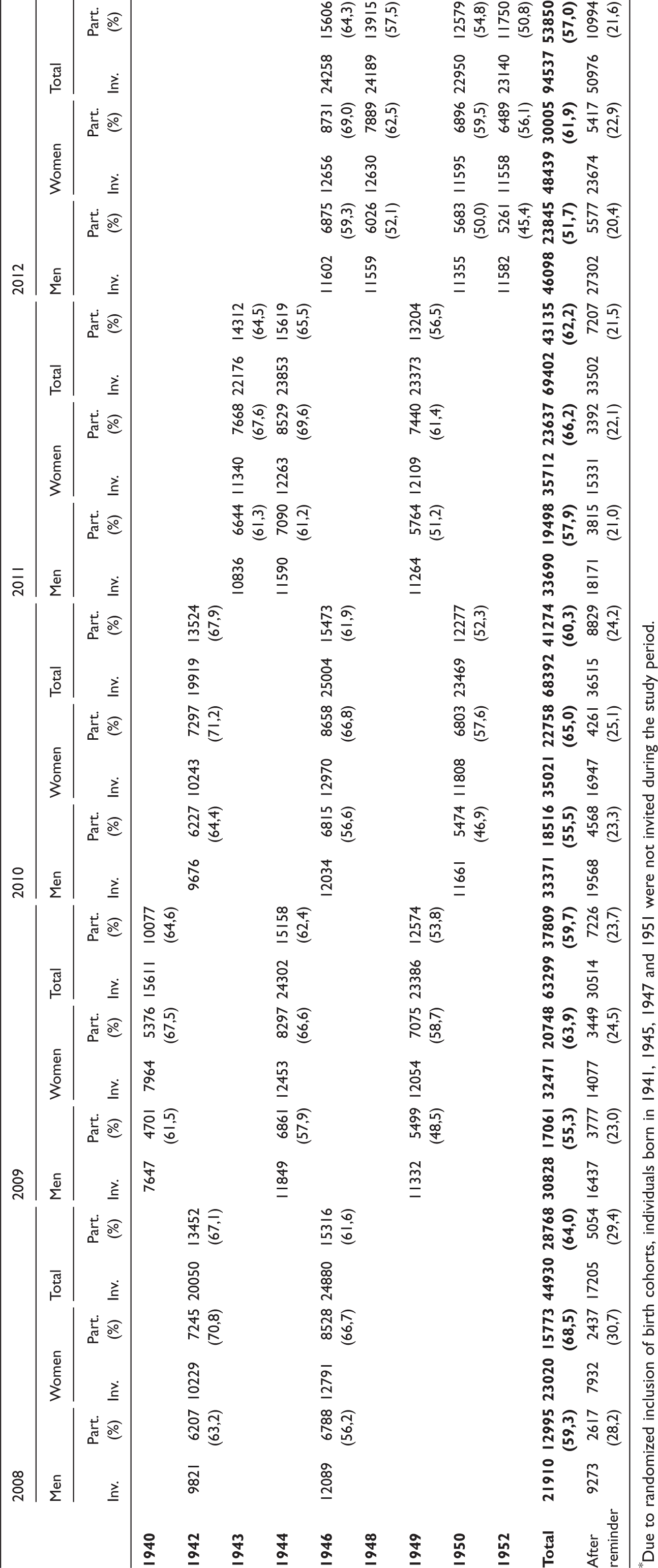
*Due to randomized inclusion of birth cohorts, individuals born in 1941, 1945, 1947 and 1951 were not invited during the study period.
All invitations, returned test results, findings at assessment colonoscopy, and histopathological diagnosis of findings are registered into the IT system designed for the screening programme. As part of the quality assurance of the programme, the records of the participating individuals were continuously linked with the Swedish Cancer Register maintained by the National Board of Health and Welfare. 19,20
Statistical analysis
Compliance rate was calculated as a percentage by dividing the number of participating individuals by all invited individuals, by screening round and gender, among birth cohorts. Compliance rate was also calculated by gender and age group (60–64, 65–69). The positive predictive values (PPV) were calculated by dividing the number of true positive test results, ie. confirmed CRC, by the total number of positive tests.
Results
More than 340,000 invitations to 200,000 individuals from nine accumulated targeted birth cohorts were sent during the five year period 2008–2012 (Table 1). The compliance rate by year of invitation varied from 57.0 to 64.0%. Nearly 40,000 individuals (19.2% of the total number of participants) did participate after the written reminder (sent out eight weeks after invitation) during this five year period (Table 1). In 2010, 8.0% of participants had been non-participants when invited in the previous round; for 2011 and 2012, the same figures were 9.6% and 7.6%, respectively. Approximately one third of invitees were non-participants at all rounds.
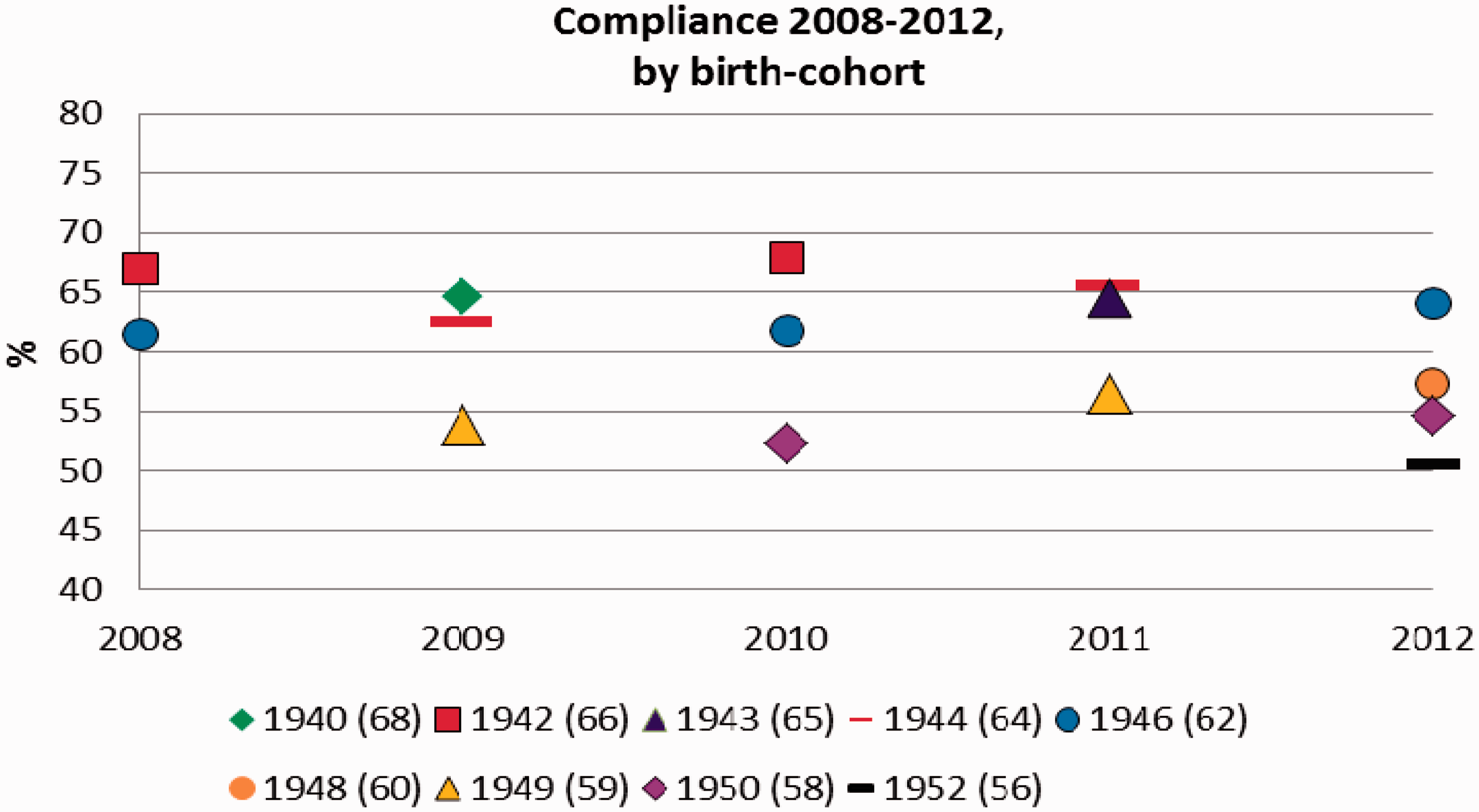
In general, women were more frequent participants (range by year and age group: 56.1–71.2%) compared with men (range 45.4–64.4%) (Table 1, Figure 2). An increase in participation rate for the older age group was also seen both for men and women (Figure 2). All re-invited birth cohorts showed increased compliance by second and third screening round (Table 1, Figure 3).
Compliance in the Stockholm/Gotland colorectal cancer screening programme of the general population aged 60–69 by screening year, age group and gender. Compliance in the Stockholm/Gotland colorectal cancer screening programme of the general population aged 60–69 by screening year and birth cohort (age at start of programme in 2008).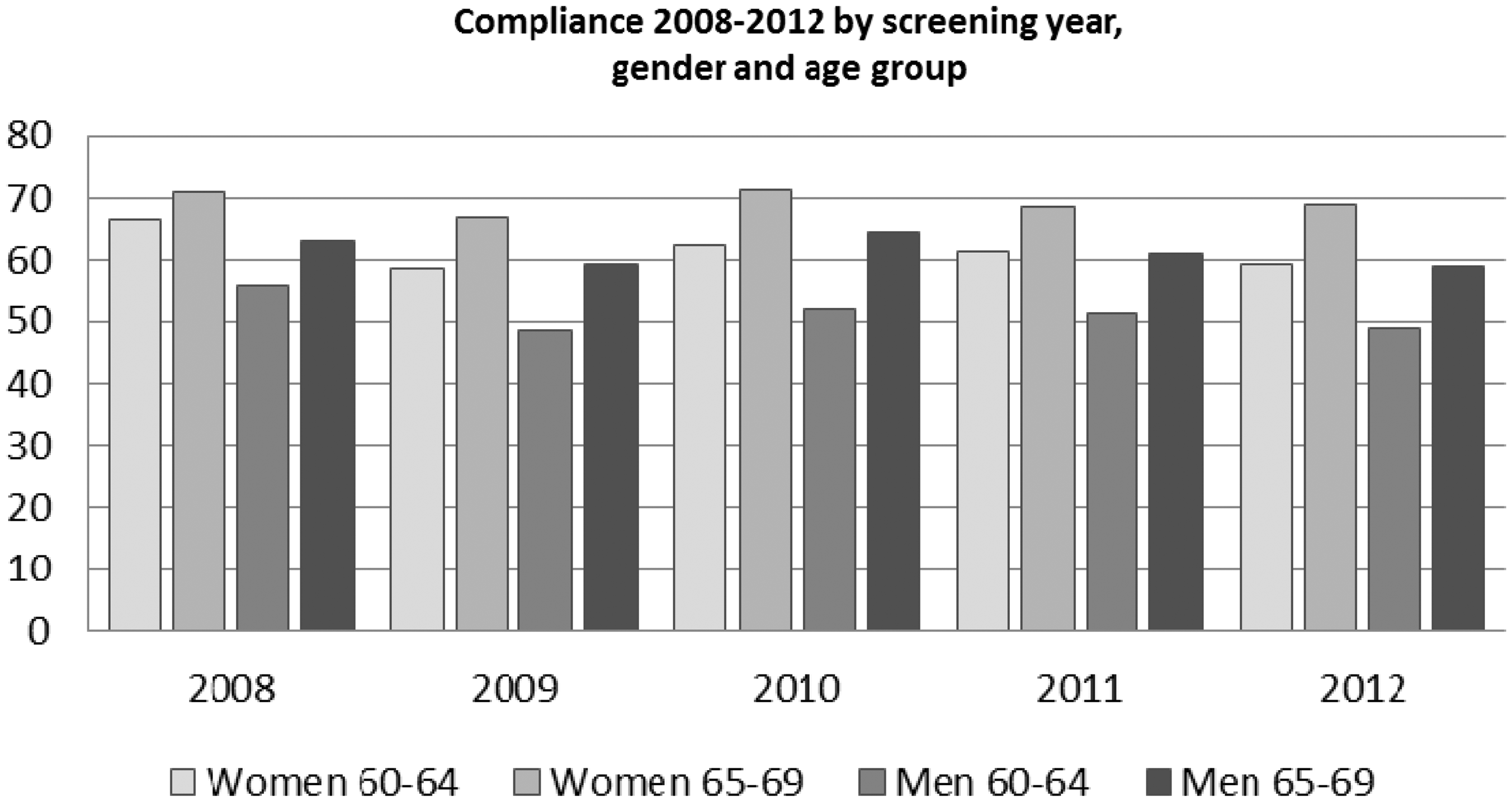
Participants, faecal occult blood test (Hemoccult®) result, compliance with colonoscopy, diagnosed colorectal cancer (CRC), and adenoma by year and screening round in the Stockholm/Gotland screening programme.
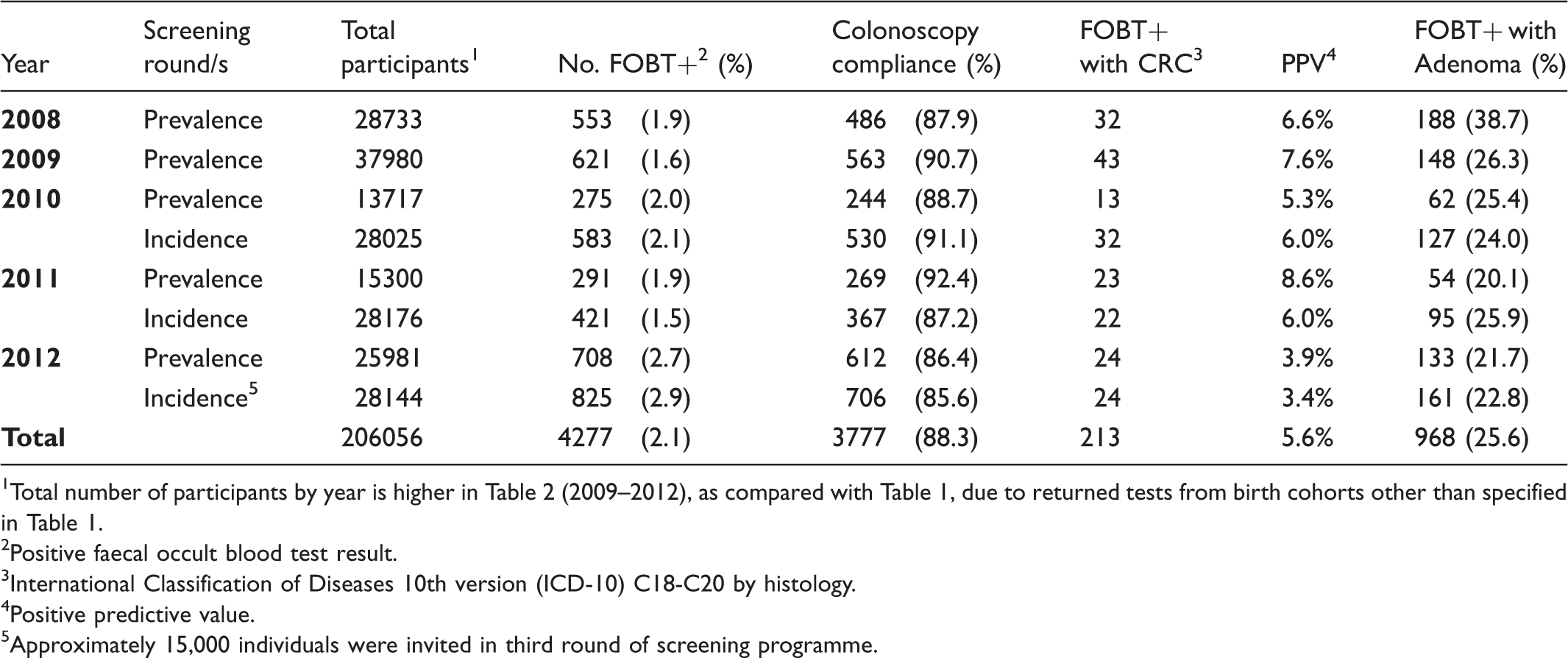
1Total number of participants by year is higher in Table 2 (2009–2012), as compared with Table 1, due to returned tests from birth cohorts other than specified in Table 1.
2Positive faecal occult blood test result.
3International Classification of Diseases 10th version (ICD-10) C18-C20 by histology.
4Positive predictive value.
5Approximately 15,000 individuals were invited in third round of screening programme.
Two hundred and thirteen colorectal cancers were found at colonoscopy and verified by histopathology, generating PPVs from 3.4–8.6% (Table 2). Of the total (nearly) 3,800 colonoscopies, approximately 3,500 were negative for cancer (false positive tests) during the five year period. However, adenomatous polyps were diagnosed in close to 1,000 patients (Table 2).
Discussion
We found a compliance rate of approximately 60% over five years, with a higher participation rate among women, among older age groups, and by subsequent screening round in the regional gFOBT-screening programme of the Stockholm Gotland region. The positivity rate was approximately 2% and the PPV for a diagnosed CRC at assessment colonoscopy was around 6%.
The primary measure of effectiveness of a FOBT-screening programme is a decreased disease-specific mortality and, with polypectomy of adenomatous polyps at assessment colonoscopy after a positive test, a decreased CRC incidence. We have randomly included birth cohorts when implementing the programme in the county of Stockholm/Gotland, to be able to compare CRC mortality outcomes and incidence between birth cohorts included or not included in the programme. The eventual reductions attributed to the organized programme will also be related to historical cohorts and counties in Sweden without screening programmes, but the evaluation of the primary outcomes cannot be measured only five years after implementation of the programme. Nevertheless, more than two hundred CRC and approximately one thousand adenomas were diagnosed during the five year period, generating an adenoma detection rate (ADR) of just over 30% (proportion of colonoscopies with CRC or adenoma). The ADR is regarded as a quality indicator of the colonoscopy, 21 and is also dependent on the prevalence in the target population. In our study, the selection of participants with a positive gFOBT resulted in an expected higher ADR than reported from primary colonoscopy screening, 22 but lower compared with the reported first gFOBT screening round in Finland, and the screening programme in the United Kingdom, with ADRs of around 40–45%.23,24
Compliance in a screening programme is another major, but early, surrogate measure of effectiveness. There are few organized programmes that are comparable with ours (target group without selection and test used), but our finding of 60% compliance with FOBT screening, and increasing compliance with subsequent screening round, is higher than previously reported from the United Kingdom (∼55%), and lower than that initially reported from Finland (∼70%).12,17 Other ongoing regional or national colorectal cancer screening programmes with guaiac-based FOBT have reported compliance rates of around 30–40%, decreasing with the supply of opportunistic screening.25–27 Comparing our results with those from other programmes may be problematic if, for example, other programmes exclude morbid people from the denominator when calculating compliance rate. With such exclusions, the denominator will be smaller and, hence, the compliance rate will appear higher compared with a programme without exclusions. 28
In addition, the age ranges covered by the screening programmes must be considered when comparing compliance rates. A highly organized call-recall system and quality assurance is necessary for a screening programme to be effective, 29 and one of the strengths of our programme is the centrally administered invitation process (∼20% of the target population participated after reminder). Our results on higher compliance among women in older age groups (Figure 2) were in agreement with findings from other screening programmes in Europe, and also in Canada.25,30 The presented follow-up colonoscopy drop out of 10–15% after a positive test is a particular challenge, but the rates are similar to those reported from the national organized guaiac-based FOBT programme in the United Kingdom. 12
Speculatively, over time, a more established screening programme with an enlightened and more experienced population might possibly increase compliance, as the targeted population is socialized with the programme. Surprisingly, over the studied five year period, the overall compliance in Stockholm/Gotland decreased by year of the programme (Table 1, Figure 3), but this might be explained by the birth cohorts of younger ages being invited in the later years (Table 1, Figure 3). By contrast, contrary to previous reports of decreasing compliance over time in the Danish FOBT pilot screening programme (nine rounds), 31 in our programme the participation rate increased in the second and third screening rounds (Table 1, Figure 3). We have not investigated the reasons for this, but, speculatively, a positive effect by screening round within that specific birth-cohort could eventually be that non-participants at first round of invitation comply with subsequent rounds. Up to approximately 10% of earlier non-participants comply in the next invitation round. We therefore recommend the continuation of re-inviting non-participants. We interpret increasing compliance at subsequent rounds as an indicator of a perception among invitees that the programme is robust and reliable.
Currently, the regional screening programme of Stockholm and Gotland uses the gFOBT (Hemoccult®) demonstrating CRC mortality reduction in the nineties.13–15 The test is observer-dependent, with a subjective evaluation of a binary negative or positive test result, which is the most likely explanation for the high rate of false positive test results and subsequent low PPV in 2012 (<4% in prevalence and incidence screening rounds), as compared with previous years (Table 2). A PPV of around 10% has been reported from other comparable programmes.12,23 The screening programme of Stockholm/Gotland is considering implementation of a quantitative faecal immunochemical test (FIT). The benefit of a quantitative test is that the programme can determine the cut-off level for a positive test, ie. deciding sensitivity and specificity, and thereby the number of false negative and false positive tests. It is essential, when considering a change in screening test, to take into account not only the ethical issues of unnecessary assessment colonoscopies, but also the colonoscopy capacity of the region.
Conclusion
After five years of colorectal cancer screening with gFOBT in Stockholm Gotland, it is clear that a highly organized programme is a prerequisite for an acceptable compliance rate that increases with subsequent screening rounds. We have confirmed lower participation among men and in younger age groups, and specific efforts are needed to address and increase compliance in these groups.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Acknowledgement
The authors thank Agneta Lissmats (Regional Cancer Centre, Stockholm Gotland) for statistical help.