
Abstract
Objectives
Analysis of screening uptake usually dichotomizes women into attenders and non-attenders, though many women respond positively to some but not all invitations. This paper studies these intermittent attenders.
Methods
A cohort of 8,571 women invited for consecutive breast screens in the Northern Ireland Breast Screening Programme were followed in a study linking screening and census records. Multivariate logistic analysis was used to analyze the characteristics of those who attended both times (consistent), once (intermittent or ‘one-time only’), or not at all (non-attenders).
Results
Overall, 15.5% of women attended once and 13.4% were non-attenders. Non-attenders were characteristically disadvantaged (as measured by social renting, car access, and employment status), less likely to be married, and more likely to be healthy. One-time attenders were younger, and suffering poor health, though there was no association with either social renting or employment status. Privately rented accommodation and city living was associated with both one-time attendance and non-attendance.
Conclusions
One-time attenders are an important and distinct subgroup of screening invitees in this analysis. Their distinct characteristics suggest that transitory factors, such as change in marital status, ill-health, or addressing difficulties through change of residence are important. These distinct characteristics suggest the need for different approaches to increase attendance, among both intermittent attenders and those not attending at all.
Introduction
Cancer is a leading cause of mortality worldwide and accounts for three of the top ten causes of death for high income countries. 1 The World Health Organization (WHO) has identified three evidence-based strategies to reduce and control the global burden of cancer: preventing cancer from occurring, detecting cancer earlier, and managing patients with cancer. 2 Early detection is predicated on the assumption that the earlier in its natural history a cancer is detected, the more effective treatment is likely to be. 1 In the United Kingdom (UK) recommendations regarding screening programmes are produced by the National Screening Committee (UK NSC), and based on evidence from randomized controlled trials demonstrating that the programme reduces mortality and morbidity. 3 However, for these programmes to be effective, the attendance of the target population at screening must be consistent and at the recommended intervals - a one-off attendance will not ensure early detection of cancer. 4 Currently, UK programmes include screening for cervical, breast, and more recently bowel cancer. Yet, despite these being free at the point of delivery across the UK, a significant proportion of people do not take up the invitation to attend. For example, between 2002 and 2010 the breast screening programme in England has (for women aged 53-64) shown average yearly coverage of approximately 75% for those invited. 5 Investment is therefore required to promote and encourage uptake of screening across the target population, so that any potential benefits of the programme are realized.
There is evidence to suggest that levels of non-attendance at screening are not uniformly distributed throughout the eligible population. For example Chui (2003) noted differences in attendance at screening services by social and ethnic background. 6 However, because of a dearth of UK-based research, an accurate picture of variation in screening uptake among different societal groups is currently not available. 6 While targeted efforts to improve uptake and repeat attendance at screening programmes have the ability to improve outcomes, these can be effective only when it is clear how uptake and re-attendance vary across the population.
Most published studies concentrate on comparing women who attend for screening with those who do not. This ignores an important intermediate group who attend intermittently, and who may have different characteristics and reasons for non-attendance from those who consistently attend. This study explores the demographic, socio-economic, and baseline health characteristics associated with uptake and re-attendance over two successive rounds of screening in the Northern Ireland Breast Screening Programme (NIBSP).
Methods
The dataset was constructed by linking data from the National Breast Screening System (NBSS) to the Northern Ireland Longitudinal Study (NILS). The process is described more fully elsewhere. 7 The analysis dataset comprised women identified in the Census, and followed up over two screening cycles to identify attendance patterns. The NBSS holds information about eligibility and uptake of breast screening in Northern Ireland. NILS is a representative 28% sample (approximately 500,000 people) of the Northern Ireland population, formed by the linkage of the Health Card Registration system and the 2001 Census returns. 8 The screening data and NILS data were linked using an encrypted Health Service identifier as the matching field, a process carried out by the respective data custodians within the secure setting in the Northern Ireland Statistics and Research Agency (NISRA). The key matching field (Health and Care Number) was subsequently removed, and the resultant anonymized research dataset held in a secure setting by the Registrar General for Northern Ireland. At no time were patient identifiable data available to the research team. The study was approved by the local ethics committee (ref: 07/NIR01/90).
Women aged between 48 and 52 at the 2001 Census and who were subsequently invited for two breast screens between April 2001 and October 2007, with the initial screen being their first, were included. If an invited woman reorganized her appointment and attended the screen at any stage within six months of the original invitation, she was included as an attendee. This covered two complete screening rounds, from 2001–2004 and 2005–2007. The lower age allowed inclusion of women who would have reached the eligible age for a first screen (50 years) by the end of the first screening round in 2004. Women living in communal establishments, or who were receiving treatment or otherwise being investigated (including repeat mammograms for technical reasons), and women with incomplete information (from NBSS or NILS) were excluded from the analysis.
The sample included a cohort of 8,571 women who received two screening invitations during the study period and who had corresponding Census-based information available. The cohort was split into three distinct groups, based on attendance at both screening rounds. The first group (consistent) comprised women who attended both screening appointments. A second (intermittent or ‘one-time’) group comprised women attended only one of the two screening appointments (589 women attended the first screen but not the second, and 738 women attended the second but not the first screen). Initial analyses showed that women who attended only the first screen were broadly similar, in terms of age and demographic characteristics, to women who attended only the second screen. Women attending the second but not the first screens were generally of a higher socio-economic status than women who attended the first but not the second. The final group (non-attenders) included women who did not attend either screen.
All characteristics of women in the cohort were as recorded on the Census form and selected as factors shown, from other studies, to be associated with screening uptake. Age was included as an independent variable, although the group of women was very similar in age and fell within a small age range (categorized as <50, 50–52). Marital status was categorized as married/co-habiting, never married, or a third group combining those widowed, separated or divorced (as analyses showed similar levels of uptake in these women). Four census-based indicators of socio-economic status were included: the National Statistics Socio-Economic Classification, highest educational attainment (ranked as: university level, ‘A-level’ or equivalent, ‘O-level’ or equivalent, and no qualifications), household car availability (two or more cars, one car, no car access), and housing tenure (owner occupier, private renter and social renter). 9 Two census-based measures of self-reported health were also included: the presence of limiting long term illness (with a yes/no response), and general health in the year preceding the Census (with three responses – good, fairly good, and not good). An indicator of the urban/rural character of the area in which the respondent lived was included, divided into two areas – Belfast Metropolitan Area and the rest of Northern Ireland, as previous research has shown that uptake is lower in cities.10–12
Multivariate logistic regression using STATA version 10 was used to explore the relationship between uptake of breast screening (comparing one-time attenders with consistent attenders, and the non-attenders with consistent attenders) and the socio-demographic and socio-economic variables. Using those classed as consistent attenders as the reference category, two sets of logistic regression analyses were carried out, separately comparing the one-time attenders and those never attending screening with the consistent attender group. A step-wise approach was taken, with the final model arrived at using a parsimonious approach, including those variables shown in previous models to be significant or to demonstrate a large effect size. Variables found to be significant or to have a relatively large effect size in either of the comparisons against consistent attenders were included in the final models.
Results
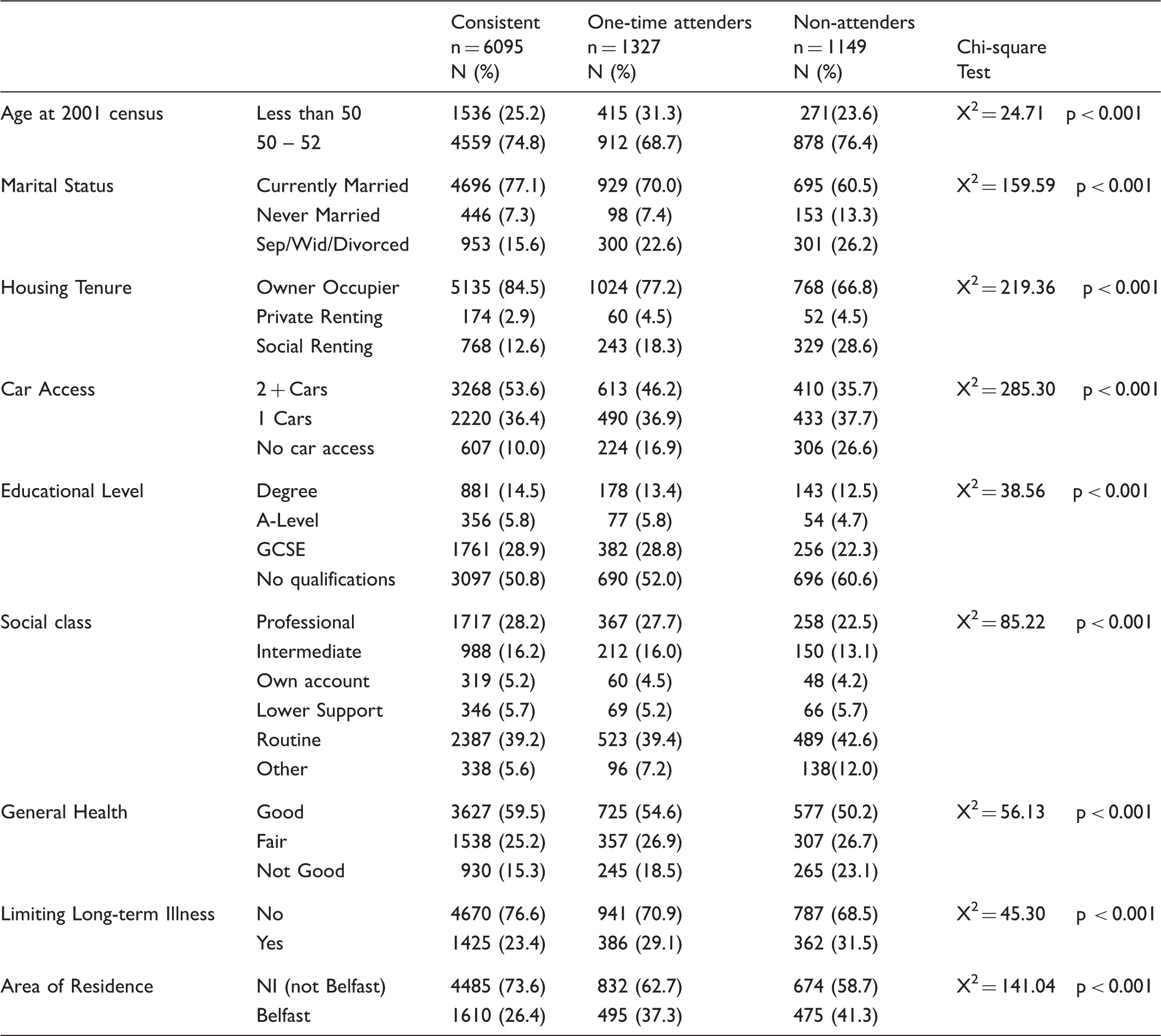
The analysis dataset comprised 11,931 women invited for their first breast screen between 29 April 2001 and 28 October 2004. Of these women, 8,571 were invited for a second routine breast screen during the following screening round (2005 to 2007), enabling analysis of the same cohort of women over two successive screening rounds. Therefore 3,360 women were not invited for a second screen (Figure 1 outlines the reasons for non-invitation). The sample was aged between 48 and 52 at the 2001 Census, with 74% aged 50–52. As the screening round length is 36 months, all women aged 48–52 at the time of the 2001 Census will have received their first screening invitation during the period 2001–2004. Almost three quarters were married (74%), with 18% separated, widowed or divorced, and 8% never married. The majority of women (81%) were owner occupiers, with 15.6% in social rented accommodation. Half of the sample had access to two or more cars, with only 13.3% having no household car access. Over half of the women recorded that they had no formal educational qualifications, and almost 40% were in routine occupations. While over half the women reported having ‘good’ general health, 16.8% reported their general health as ‘not good’. Approximately three quarters reported no limiting long-term illness. Just under one third of the sample lived in the Belfast Metropolitan Area (BMA).
Flow diagram showing the process of identifying the final sample of women for analysis.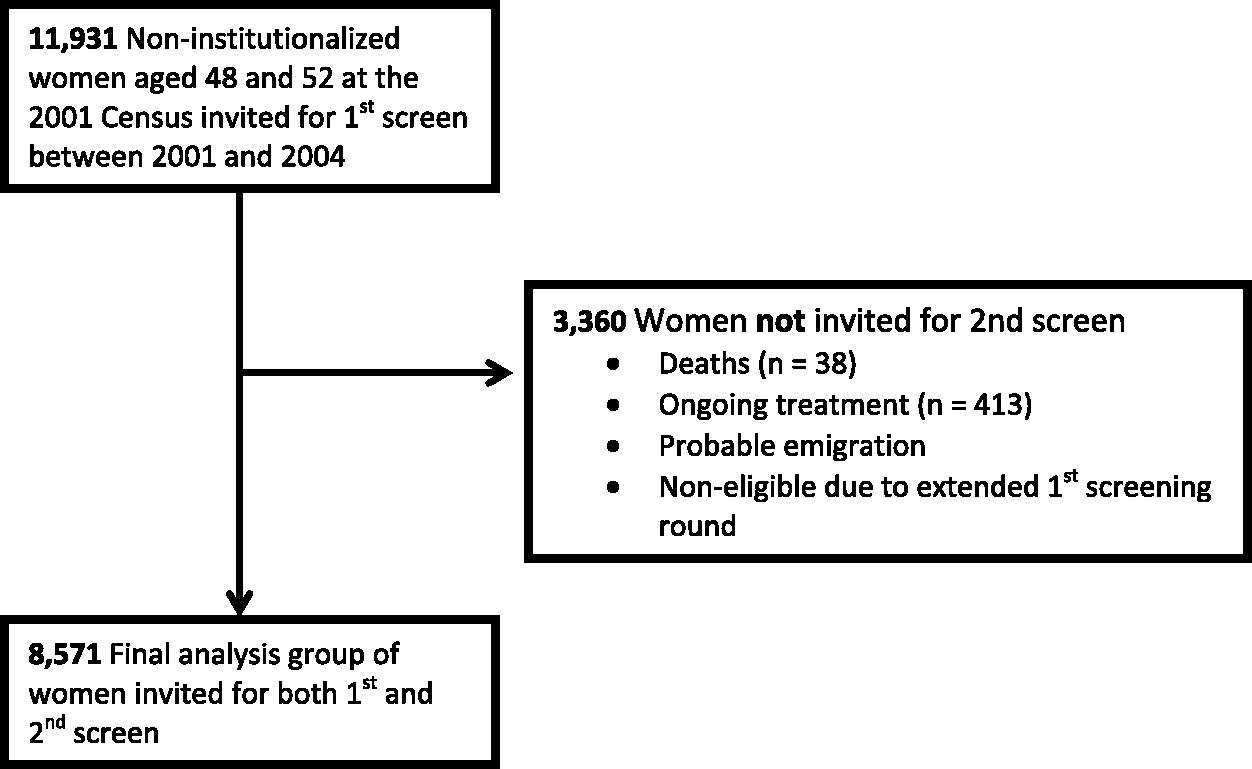
Demographic, socio-economic, health status and area-level characteristics in the three groups differentiated by attendance levels at two successive screening rounds. Figures in brackets represent the percentage of that group which falls into each category.
Comparing one-time attenders and non-attenders with consistent attenders at breast screening, adjusted for those demographic, socio-economic, health status and area-level variables found to be significant in model-building analyses. Results represent odds ratios (OR) and 95% Confidence Intervals.
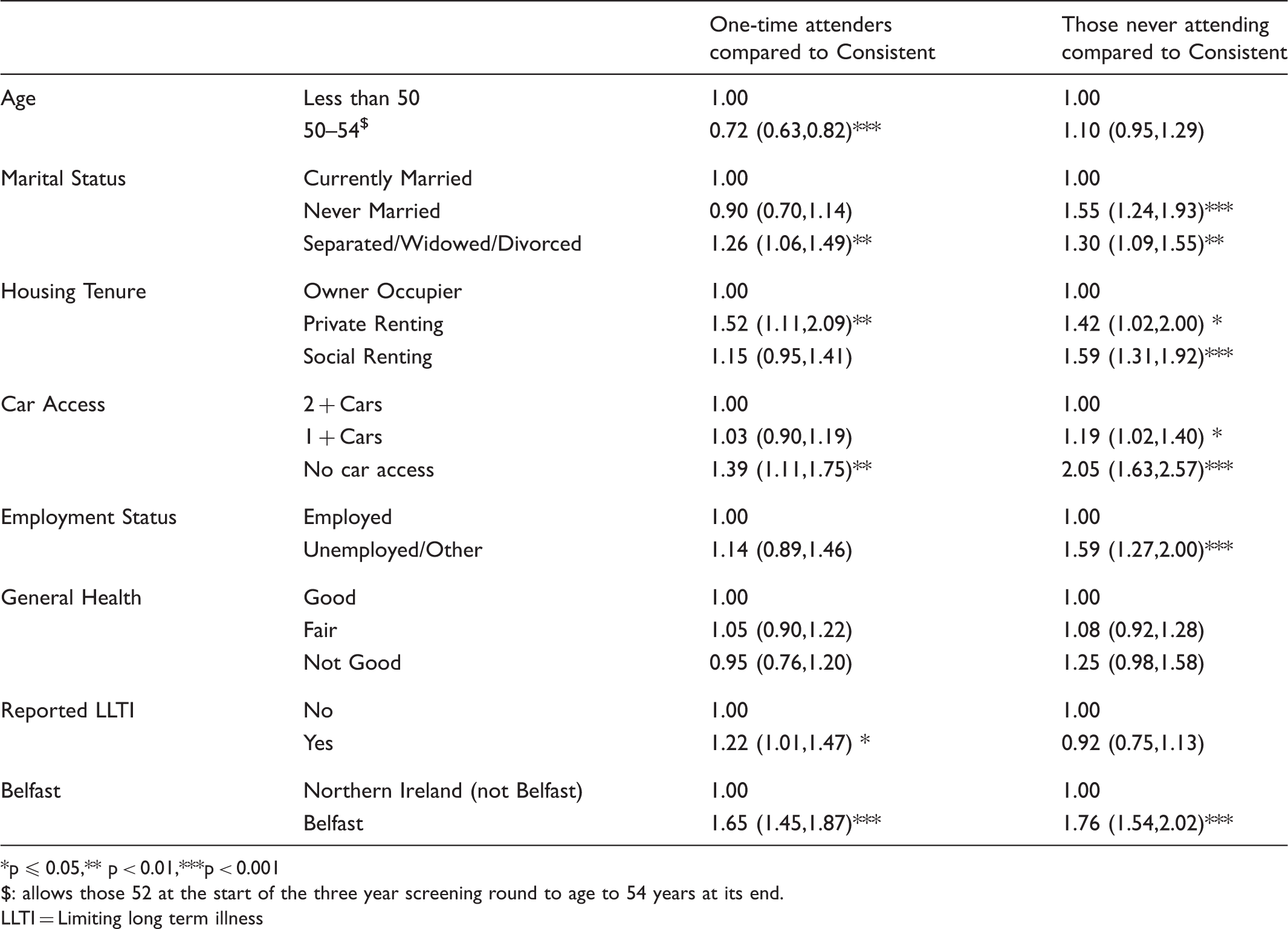
p ≤ 0.05,** p < 0.01,***p < 0.001
: allows those 52 at the start of the three year screening round to age to 54 years at its end.
LLTI = Limiting long term illness
In comparison with those consistently attending (Table 2), one-time attenders are more likely to be younger, to be separated, widowed or divorced (Odds ratio [OR] = 1.25: 95% confidence interval [CI] = 1.06, 1.49), to live in privately rented accommodation (OR = 1.52: 1.11, 2.09), to report a limiting long term illness, to live in a household with no access to cars, and to live in Belfast.
Discussion
This study used a census-based record linkage methodology to examine the characteristics of women invited to two consecutive breast screens in the NIBSP. To our knowledge this is the first analysis of its kind to have been undertaken in the UK. It has demonstrated that intermittent non-attenders (‘one-time’) are both an important and distinct subgroup of screening invitees, representing approximately 15% of women invited for screening over a two cycle period, and displaying different characteristics from both those attending consistently and those who did not attend either round.
The study also provides evidence that the factors determining non-attendance may differ between the one-time attenders and those who did not attend either round (although these two groups have not been formally compared). Being separated, widowed, or divorced predicted one-time attendance, while being never-married did not, suggesting that these life-events may have some impact on attendance patterns. Marital status is a proxy indicator for family/social support networks, so it may be that the support issue is more positively associated with attendance at screening than marital status per se. While the literature generally reflects a positive association between marriage and screening re-attendance, this finding has not previously been reported.13–15 While previous research has firmly established the relationship between any attendance at screening and socio-economic status, we found it to be related only to persistent non-attendance.15–18 The weaker relationship between some socio-economic indicators and one-time attendance may suggest alternative interpretations, for example, it is associated with non-access to cars, suggesting difficulties with physical access rather than material disadvantage per se. Similarly, lower attendance levels are associated with private renting, but not social renting, suggesting this may relate to addresses on invitation letters, and that perhaps these women are not receiving their invitations. 10 Finally, the relationship between limiting long term illness and one-time attendance suggests that at least some of this non-attendance may be due to issues related to physical ill-health.
The major strength of this study is the quality of the linked administrative datasets, and the consequent absence of responder burden and bias. However, this is also a source of possible weakness. As already noted, our interpretation of the putative factors contributing to one-time attendance (marital breakdown, physical ill-health, transport difficulties, and addressing issues), while plausible, cannot be substantiated. To do this would require qualitative studies, and few to date have been of sufficient scale to provide results on intermittent attendance. That there was little difference between those who missed the first screen and those who missed the second suggests that any negative experiences (for those women who were previously screened) associated with the process are not significant. It is also possible that the characteristics of some women at the second screen will have changed (some four to six years after the census), and this may introduce misclassification and underestimate the relationships presented here. All women invited to a second screen by the NIBSP were included in the cohort, however, it was not possible to assess the proportion of women who actually received their invitation. The inclusion of women in the analysis who may not have received their invitation, classified as non-attenders (to one or both rounds), may introduce an element of bias.
In this study over 85% of women attended at least one screen but only 71% attended both. Optimal screening procedures are calculated to provide for maximum yield at lowest cost, but programmes will be inefficient if adherence to schedules is poor. If the already noted disruptions related to intermittent attendance are indeed important, then perhaps more persistent recall mechanisms are necessary before individuals are designated as non-attenders. Transport difficulties, if confirmed, might be alleviated by judicious use of mobile clinics, and address inaccuracies (a recognized and recurrent problem) indicate the need to maintain accurate address files. The study re-emphasizes the importance of initiatives aimed at reducing social gradients in attendance levels, as the socially disadvantaged are both less likely to attend a first screening and also to continue missing subsequent appointments. Approximately 40% of those not consistently attending lived in the Belfast metropolitan area, and they were 70% more likely not to attend than their peers living elsewhere in Northern Ireland. This has been noted previously, and represents a major challenge to the efficiency of screening programmes. 19
Footnotes
Declaration of conflicting interests
There are no conflicts of interests and this article, in whole or in part.
Funding
The NILS is funded by the Health and Social Care Research and Development Division of the Public Health Agency (HSC R&D Division) and NISRA. The NILS-RSU is funded by the ESRC and the Northern Ireland Government.
Research ethics
The study was approved by the local ethics committee, the Office for Research Ethics Committee for Northern Ireland (ORECNI) (ref: 07/NIR01/90).
Acknowledgements
The help provided by the staff of the Northern Ireland Longitudinal Study (NILS) and the NILS Research Support Unit is acknowledged. The authors alone are responsible for the interpretation of the data and any views or opinions presented are solely those of the author and do not necessarily represent those of NISRA/NILS.