
Abstract
Objective
Little research exists on what predicts individual return to screening after a false-positive faecal immunochemical test in a population bowel screening programme. We aimed to quantify the impact of false-positive faecal immunochemical test in the first round of screening on re-attendance in BowelScreen, the National Bowel Screening Programme in Ireland.
Methods
A retrospective cohort study was conducted. False-positivity was defined as a positive faecal immunochemical test with subsequent colonoscopy showing no evidence of malignancy or surveillance requirement. In those with a false-positive faecal immunochemical test, logistic regression was used to predict repeat participation in the second round.
Results
Of 196,149 individuals who attended the first screening round, 108,075 were eligible and re-invited in the second round, and 93,971 accepted the invitation (86.9%). Second round uptake was higher in faecal immunochemical test-negative individuals compared with those having false-positive results (87.5% vs. 73.1%; p < 0.001). Older age (odds ratio (OR) 0.75; 95% confidence interval (CI) 0.60–0.94), computed tomography colonography (unsuitability/failed colonoscopy) (OR 0.40; 95% CI 0.21–0.73), and longer duration from screening invitation to faecal immunochemical test result (OR 0.991; 95% CI 0.9872–0.995) were predictors of non-re-attendance in the next screening round.
Conclusion
There is a significant reduction in re-attendance rates for individuals with false-positive faecal immunochemical test results. The letter sent following a negative colonoscopy is being reviewed to ensure that it provides adequate encouragement to re-attend. There are roles for screening promotion and for Gastroenterologists and Advanced Nurse Practitioners to emphasize the importance of regular faecal immunochemical tests after a negative colonoscopy.
Introduction
In Ireland, colorectal cancer is the second most common incident cancer in males and third most common in females. 1 Over a 20-year period from 1994–1998 to 2010–2014, five-year survival for colorectal cancer in Ireland increased from 48% to 62% in males, and 52% to 63% in females; however, in 2013–2015 colorectal cancer accounted for 13% of male cancer deaths (second highest cancer death) and 10% of female cancer deaths (third highest cancer death). 1
BowelScreen, the National Bowel Screening Programme in Ireland, sits within the governance of the National Screening Service. The BowelScreen Programme screens individuals aged 60–69 every two years. It is one of the first national population bowel screening programmes to use faecal immunochemical testing (FIT) for population screening. 2 Eligible individuals are invited to participate by post, and those giving verbal consent by telephone are sent a self-administered FIT kit. These kits are returned to a central laboratory. Individuals with a positive result (>45 µg/Hb/g faeces) are offered a colonoscopy in one of 14 internationally approved colonoscopy units throughout the country. If FIT positive individuals are unsuitable for colonoscopy, or if colonoscopy cannot be completed, computed tomography colonography (CTC) is offered. 3 The BowelScreen Programme commenced in late 2012, with the first round completed in 2015 and the second round completed in late 2017. The uptake rate in the first round of screening was 40.2% against a standard of ≥50%.2,3 Because a high uptake rate of screening is required to achieve reduction in incidence and mortality rates of bowel cancer, factors that may influence uptake need to be understood in order to reduce or eliminate the barriers to screening.
Previous studies have suggested that prior experience with cancer screening may influence a patient’s willingness to continue future screening.4–7 Our previous work on BreastCheck, the National Breast Screening Programme in Ireland, showed that in women with a false-positive result, first breast screening, older age, open surgical biopsy, and longer duration from recall to non-malignant diagnosis were significant predictors of non-re-attendance. 4 There is limited research on return to bowel screening after a false-positive guaiac faecal occult blood test (gFOBT), and no research after a false-positive FIT. Taksler et al. showed that women with false-positive colorectal cancer gFOBT screening results were less likely to engage in future breast cancer screening 5 ; however, qualitative studies have shown that false-positive gFOBT results were unlikely to undermine confidence in the bowel screening programme.6,7
In the first round of the BowelScreen Programme, the FIT positive rate was 5% and 9788 individuals were referred for colonoscopy. 2 In this study, a false-positive FIT test was defined as a positive FIT test with a subsequent colonoscopy showing no evidence of malignancy or adenoma(s) requiring surveillance. Such individuals were offered a repeat FIT in two years as part of routine screening. The aim of this research was to quantify the impact of false-positive FIT screening results in the first round on re-attendance in the second round.
Methods
Data are routinely collected on all individuals and patients attending the BowelScreen Programme. An anonymized dataset was obtained for analysis with approval from the BowelScreen Clinical Director. This was a retrospective study focusing on a cohort of individuals who attended bowel screening in the first screening round and remained eligible for screening in the subsequent screening round. This cohort consisted of individuals in the first screening round, who were FIT negative or had a false-positive FIT, as defined above. Those who exited the eligible age-range, who were detected with cancer, or who were undergoing follow-up surveillance were excluded, as they were not eligible for screening in the next round. Participation rates were then compared between the false-positive FIT and FIT negative groups, overall, and stratified by age and gender.
In those with a false-positive FIT, the effects of age group (≤64 or ≥65), gender, CTC, biopsy, duration (in days) from bowel screening invitation to FIT result, and waiting time (in days) for colonoscopy appointment (after individuals were deemed suitable) on repeat participation in the second screening round were examined.
We used the chi-square test for comparison of proportions (e.g. comparison of proportions of false-positive FIT and negative FIT returning in the second round of screening) and the t-test to compare means (e.g. comparison of mean waiting time for colonoscopy in those who attended in second round and those who did not attend). Factors significant in univariate analysis and age and gender (as important potential confounders) were entered into a logistic regression model to determine independent predictors of re-attendance in the next bowel screening round. Interaction terms were tested in the model (age×duration, age×CTC) but were not found to be significant. IBM SPSS Statistics Version 24 was used. Ethics exemption for analysis of existing data was obtained from the University College Dublin Research Ethics Committee.
Results
From 196,149 individuals in the study database who attended the first screening round, 108,075 were eligible and re-invited in the second round. Of these, 105,276 were FIT negative and 1999 had a false-positive FIT test in the first round; 8062 underwent colonoscopy, giving a false-positive rate of 24.8%. In the second round 93,971 accepted a repeat FIT, giving an acceptance rate of 86.9%. Individuals with a negative FIT in the first round had a significantly higher uptake in the second round (92,133/105,276; 87.5%) than those who received a false-positive result in the first round (1461/1999; 73.1%). This finding was similar in all subgroups after stratification by age and gender (Table 1).
Comparison of re-attendance at next screening of false-positive FIT with those not recalled to assessment.
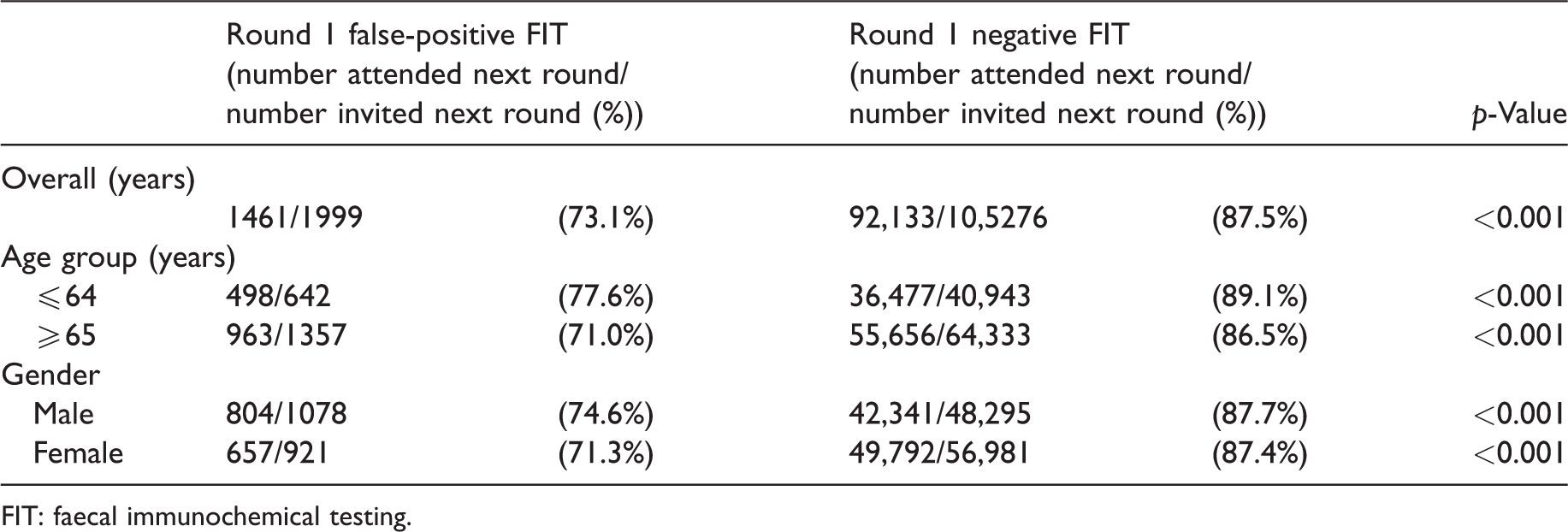
FIT: faecal immunochemical testing.
Table 2 shows the univariate analysis of factors associated with re-attendance in the subgroup of individuals with false-positive FIT results. Those in the younger age group (≤64) were significantly more likely to re-attend the subsequent bowel screening round compared with the older age group (≥65) (77.6% vs. 71.0%; p = 0.002). Those who underwent CTC were significantly less likely to re-attend in the next screening round (52.7% vs. 73.7%; p = 0.001). Those who underwent biopsy were significantly more likely to re-attend (72.4% vs. 78.2%; p = 0.036). The duration (in days) from screening invitation to FIT result (Table 2) was 11.4 days shorter for those who re-attended in the second round of bowel screening than those who did not (44.3 vs. 55.7days; p < 0.001). Gender (males 74.6%, females 71.3%) and waiting time (34.5 vs. 32.4 days) for colonoscopy appointment after individuals were deemed suitable were not significantly associated with re-attendance within this cohort on univariate analysis.
Post false-positive FIT re-attendance by age, gender, CT colonoscopy, biopsy, and duration from screening invitation to FIT result.
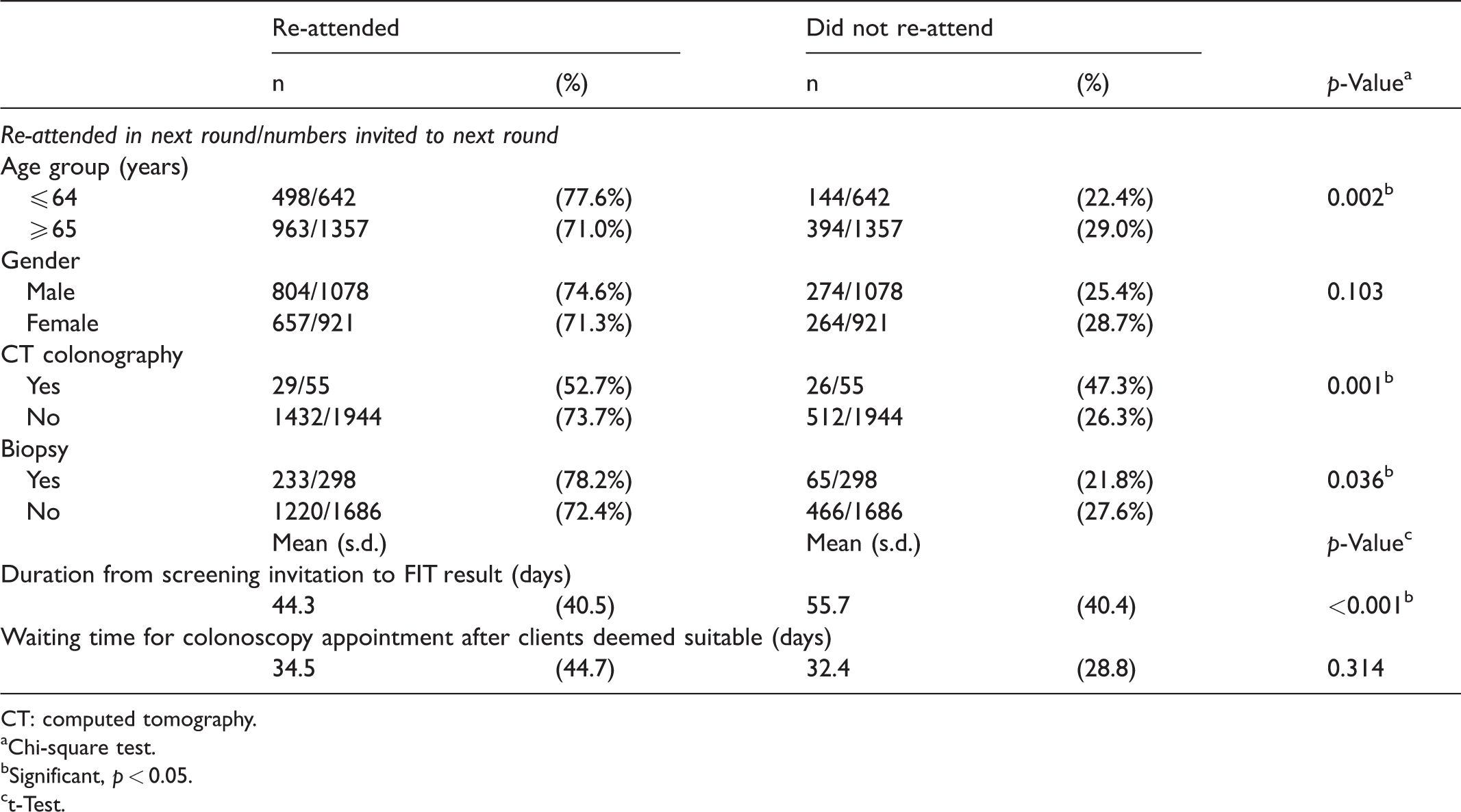
CT: computed tomography.
Chi-square test.
Significant, p < 0.05.
t-Test.
Age group, gender, CTC following a failed colonoscopy or in individuals unsuitable for colonoscopy, having a biopsy, and duration (in days) from screening invitation to FIT result were all entered into a logistic regression model (Table 3). Older age (adjusted odds ratio (OR) 0.75; 95% confidence interval (CI) 0.60–0.94), CTC (adjusted OR 0.40; 95% CI 0.21–0.75), and longer duration from bowel screening invitation to FIT result (adjusted OR 0.994 per day; 95% CI 0.992–0.996) all remained as significant predictors of non-re-attendance.
Logistic regression: predictors of attendance at next screening round post false-positive FIT.
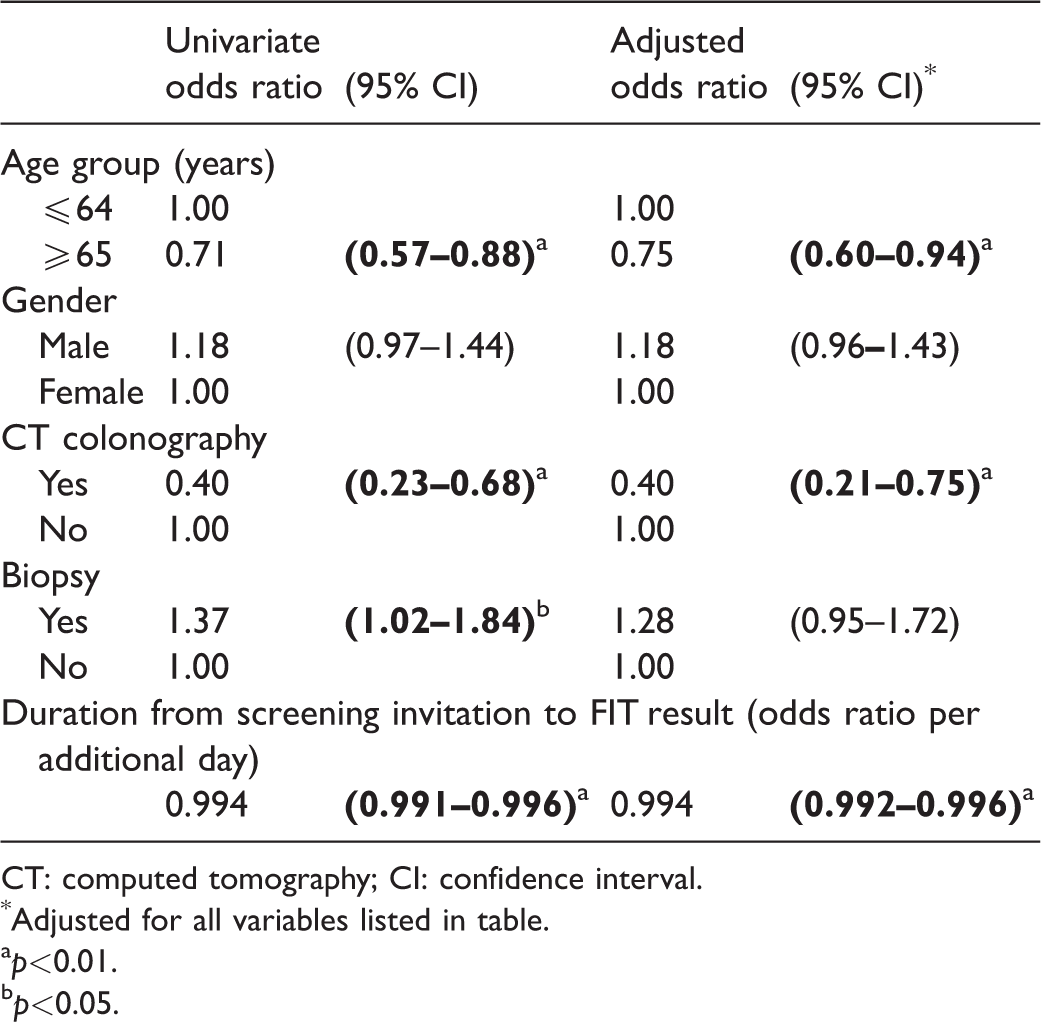
CT: computed tomography; CI: confidence interval.
Adjusted for all variables listed in table.
p<0.01.bp<0.05.
Discussion
This study shows a significant reduction in re-attendance rates for individuals after a false-positive FIT result in the first round of bowel screening, when compared with those who had a normal FIT result. Overall, this reduction was seen in older and younger individuals, and in both genders. This is an important finding as mortality rates are high for clinically presenting colorectal cancer, and every effort needs to be made to maintain adherence to screening throughout the age range called for screening (which in Ireland is age 60–69 with plans to extend to 55–74). Regular colorectal cancer screening is important for preventing new colorectal cancers from developing as well as for early identification of existing colorectal cancers. 8
A good quality negative colonoscopy means a very low chance of significant pathology within 3–5 years, so it can be reassuring for those who are false-positive. Some individuals may be aware of this and it could contribute to the reduced subsequent uptake; however, we have no data to support this hypothesis yet.
In the subgroup of individuals with a false-positive FIT, we found that older age was a predictor of non-re-attendance. This is contrary to the uptake of screening in the first screening round of the BowelScreen Programme, where rates were somewhat higher in older individuals. 2 Individuals with a longer time between bowel screening invitation to FIT result in the first round were also less likely to return at the subsequent screening round. This finding could relate to some lack of engagement of the individual in providing consent to the BowelScreen Programme and/or the individual delaying undertaking and returning the FIT test by post to the BowelScreen Programme. It could also relate to a longer period of anxiety waiting for the result from the BowelScreen Programme, despite the fact that the BowelScreen Programme has consistently performed extremely well against its target of sending results within four weeks of receipt of the sample at the laboratory, with almost all individual results sent within two weeks in the first screening round.2,9 Research by Lo et al. in the NHS Bowel Screening Programme showed that late return of the FOBt test kit by the individual was consistently associated with lower uptake in subsequent rounds. 10 In a study by Parker et al., anxiety scores measured in 100 test-positive patients were highest after notification of a positive test and before investigation by colonoscopy. 7 In patients with false-positive results, scores fell the day after colonoscopy, and remained low one month later. The study by Lo et al., examining predictors of repeat participation in the NHS bowel cancer screening programme, found that among those who remained eligible for routine screening, a definitive abnormal gFOBT result was strongly associated with lower subsequent uptake. In addition, failure to comply with follow-up examinations in a previous screening episode was also independently associated with lower repeat uptake. 10
The finding of reduced re-attendance following CTC was somewhat unexpected. A retrospective analysis of NHS Bowel Screening Programme patient experience by postal questionnaire of screens from a FOBt-based screening programme where CTC was performed when colonoscopy was incomplete or deemed unsuitable found only small differences in test-related discomfort. CTC was well tolerated as a completion procedure. 11 Most reports of studies comparing comfort experiences between CTC and optical colonoscopy favour the former,12,13 but this is not invariable.14,15 A United States report found that Black and Hispanic subjects had a preference for CTC over optical colonoscopy compared with Whites. 16 In this study, individuals undergoing CTC following a failed colonoscopy or unsuitability for colonoscopy, perhaps with greater anxiety or the effect of having further procedures, were less likely to return for subsequent bowel screening.
Previous work on BreastCheck (the National Breast Screening Programme in Ireland) found that in women who had a false-positive result, older age and a longer time between recall to assessment and final confirmation of non-malignant diagnoses were significant predictors of non-re-attendance in the subsequent breast screening round. 4 Although this study cohort consists of both men and women, the results presented in this paper concur with the BreastCheck findings, although the breast screening study showed that women who underwent biopsy were less likely to re-attend the subsequent screening round, which does not agree with our result. It may be possible that this is because the biopsy is taken during the endoscopy procedure and may be considered by the individual as part of the procedure. In addition, the biopsy was taken under sedation, whereas breast biopsies are taken under local anaesthetic as a follow-up test at assessment.
A major strength of this study is that it uses high-quality data from a large database originating from a national programme (BowelScreen). Colonoscopies conducted within the BowelScreen Programme were all carried out at screening colonoscopy units accredited by the Joint Advisory Group on Gastroenterology in the UK. 17 The study has some limitations. Adverse events during colonoscopy in the BowelScreen Programme are very low, and the numbers precluded analysis. In addition, a small number of individuals who did not attend colonoscopy or CTC may have gone outside the public screening programme and attended a private institution for their colonoscopy. These individuals would be likely to hold private health insurance and be of higher socioeconomic status. We could not include these individuals and acknowledge that they may differ. Data on socioeconomic status are not collected by the BowelScreen Programme or by any of the adult population cancer screening programmes run by the National Screening Service. Such data would be an important addition.
Barriers may differ between groups, such as individuals attending for the first time compared with those attending for a second or subsequent screening. Further follow-up of the BowelScreen Programme will determine whether having a false-positive result in a subsequent bowel screening round has a similar impact on re-attendance. The letter sent to patients following a negative colonoscopy is being reviewed to ensure that it provides adequate encouragement to re-attend, along with sufficient information to make an informed choice when next called for screening. Screening promotion officers can also advise General Practitioners (Family Doctors), and there is also a role for Gastroenterologists and Advanced Nurse Practitioners delivering colonoscopy results to emphasize the importance of regular FIT tests after a negative colonoscopy.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.