
Abstract
Although post-transplant cyclophosphamide (PTCy) is widely used to prevent graft-versus-host disease (GVHD), its protective effect remains inadequate in patients undergoing myeloablative haploidentical peripheral blood stem cell transplantation (haplo-PBSCT). We retrospectively evaluated the efficacy of PTCy combined with either pre-transplant or post-transplant antithymocyte globulin (ATG) for GVHD prevention in 114 haplo-PBSCT recipients. The PTCy+FTATG group (n = 74) received ATG at a total dose of 5 mg/kg on days −3 to −1, together with PTCy at 25 mg/kg on days +3 and +4. The PTCy+PTATG group (n = 40) received PTCy at 50 mg/kg on days +3 and +4, followed by ATG at 2.5 mg/kg on day +8. Both univariate and multivariate analyses showed that PTCy+FTATG prophylaxis significantly lowered the risk of grade II–IV acute GVHD (9.5% vs 27.5% [HR 0.24; 95% CI: 0.10–0.59; P = 0.002]) and grade III–IV acute GVHD (5.4% vs 17.5% [HR 0.19; 95% CI: 0.07–0.54; P = 0.002]). The 2-year cumulative incidence of chronic GVHD was 16.7% in the PTCy+FTATG group and 27.5% in the PTCy+PTATG group (P = 0.15). At 2 years, overall survival (OS), progression-free survival (PFS), and graft-versus-host disease-free relapse-free survival (GRFS) were 87.8% vs 72.5% (P = 0.04), 82.2% vs 65.0% (P = 0.03), and 78.1% vs 55.0% (P = 0.005), respectively. These results suggest that half-dose PTCy combined with low-dose pre-transplant ATG may be a promising strategy for GVHD prophylaxis.

Keywords
Introduction
Peripheral blood stem cells (PBSCs) are increasingly used in haploidentical hematopoietic cell transplantation (haplo-HCT) because they are more readily available and eliminate the need for donor anesthesia and the risks associated with bone marrow (BM) harvest. However, compared with BM, PBSC grafts provide faster engraftment and may lower relapse risk. Still, they are also linked to a significantly higher incidence of both acute and chronic graft-versus-host disease (GVHD) 1 . Therefore, minimizing GVHD in recipients undergoing haploidentical peripheral blood stem cell transplantation (haplo-PBSCT) remains a major clinical priority.
Post-transplant cyclophosphamide (PTCy) is an established and effective approach for GVHD prophylaxis. However, in patients undergoing myeloablative conditioning (MAC) haplo-PBSCT, PTCy alone often does not provide adequate GVHD control and may be associated with adverse effects such as delayed engraftment and increased infections2–5. In comparison, high-dose antithymocyte globulin (ATG)-based regimens are associated with substantial rates of infection, non-relapse mortality (NRM), and other treatment-related complications6,7. Combining PTCy with ATG may offer complementary or synergistic protection against GVHD while allowing dose reduction to limit toxicity.
Several recent studies have evaluated different combinations of PTCy and ATG for GVHD prevention in patients undergoing haplo-HCT. However, most available evidence comes from recipients treated with reduced-intensity conditioning (RIC)8–13. In comparison, data on the most effective combination strategy in the MAC haplo-PBSC setting, particularly regarding the optimal timing and dosing of ATG, remain scarce. The timing of ATG administration, whether before or after transplantation, may significantly influence immune reconstitution and subsequent clinical outcomes.
In this single-center retrospective study, we examined recipients of MAC haplo-PBSCT who received combined PTCy and ATG prophylaxis, with particular emphasis on the effect of ATG timing (pre-transplant vs post-transplant) on transplantation outcomes, aiming to identify a more effective prophylactic strategy.
Methods
Patients
This retrospective study included consecutive patients who underwent MAC haplo-PBSCT at West China Hospital, Sichuan University, between June 2015 and December 2024. Eligible patients were 14–65 years of age, had a diagnosis of hematological malignancy based on World Health Organization (WHO) criteria, and met transplantation indications according to risk stratification defined by the National Comprehensive Cancer Network (NCCN) guidelines. Patients with severe hepatic, renal, pulmonary, or cardiac dysfunction were excluded.
Donor
All patients received grafts from related haploidentical donors with at least one antigen mismatch at HLA-A, HLA-B, HLA-C, or HLA-DRB1. All recipients were screened for donor-specific antibodies (DSAs) against both class I (HLA-A, HLA-B, HLA-C) and class II (HLA-DR) antigens. Patients with DSAs showing a mean fluorescence intensity (MFI) >2000 received plasmapheresis or rituximab to lower the MFI to <2000 before transplantation. Donors were mobilized using a granulocyte colony-stimulating factor (G-CSF) at 7.5–10 μg/kg/day. PBSCs were collected on days 5 and 6, aiming for a CD34+ cell dose of ≥2 × 106/kg of recipient body weight.
Conditioning regimen
MAC regimens were tailored according to disease type, risk category, patient age, and performance status. Patients with acute myeloid leukemia (AML) or myelodysplastic syndrome (MDS) received the Flu+Bu+Ara-C (FBA) regimen. Those with high-risk relapse or undergoing salvage transplantation were treated with the Ara-C+Bu+CDA (ABC) regimen, while patients with concurrent myelofibrosis or extramedullary disease received the TT+Bu+Flu (TBF) regimen. Patients with acute lymphoblastic leukemia (ALL) received either the FBA or TBF regimen. Drug doses within these regimens were as follows: busulfan (Bu) 3.2 mg/kg/day for 4 days (reduced to 3 days when combined with thiotepa [TT]), fludarabine (Flu) 30 mg/m2/day for 5 days, cladribine (CDA) 5 mg/m2/day for 5 days, cytarabine (Ara-C) 1 g/m2/day for 5 days, and TT 5 mg/kg/day for 2 days.
GVHD prophylaxis
Patients were divided into two groups according to their GVHD prophylaxis regimen. The PTCy plus pre-transplant ATG group (PTCy+FTATG, n = 74) received ATG at a total dose of 5 mg/kg from day −3 to day −1, followed by PTCy at 25 mg/kg/day on days +3 and +4. The PTCy plus post-transplant ATG group (PTCy+PTATG, n = 40) received high-dose PTCy at 50 mg/kg/day on days +3 and +4, followed by ATG at a total dose of 2.5 mg/kg on day +8.
All patients also received additional immunosuppression with cyclosporine A, initiated on day +5 as an intravenous infusion at 3 mg/kg/day and adjusted to maintain a whole-blood trough concentration of 300–400 ng/mL. After recovery of gastrointestinal function, cyclosporine A was converted to an oral formulation targeting a trough level of 200–300 ng/mL, with tapering started at 4–5 months after transplantation. Mycophenolate mofetil was given at 10 mg/kg twice daily from day +5, reduced to 500 mg once daily on day +35, and discontinued on day +100. Acute GVHD (aGVHD) was treated with methylprednisolone at 1–2 mg/kg/day. Second-line therapies, including basiliximab, ATG, or Janus kinase 1 and Janus kinase 2 (JAK1/2) inhibitors, were used in patients with disease progression after 3 days of treatment or in those who did not improve after 7 days.
Definitions
The study endpoints included overall survival (OS), progression-free survival (PFS), graft-versus-host disease-free relapse-free survival (GRFS), time to neutrophil and platelet engraftment, aGVHD, chronic graft-versus-host disease (cGVHD), cumulative incidence of relapse (CIR), and NRM. Neutrophil engraftment was defined as the first of 3 consecutive days with an absolute neutrophil count (ANC) >0.5 × 109/L. Platelet engraftment was defined as a platelet count ≥20 × 109/L maintained for 7 consecutive days without transfusion support.
All patients underwent follow-up evaluations on day +28, including BM morphology, flow cytometry, and chimerism analysis. Donor chimerism was measured using short tandem repeat–polymerase chain reaction (STR-PCR). Complete donor chimerism was defined as ≥95% donor-derived leukocytes. Relapse was defined as the reappearance of >5% blasts in the BM or the development of extramedullary disease. NRM was defined as death from any cause other than relapse.
PFS was defined as the time from haplo-PBSCT to disease relapse or death while in remission. OS was defined as the time from haplo-PBSCT to death from any cause. A GRFS event was defined as the occurrence of grade III–IV aGVHD, severe cGVHD, relapse, or death from any cause after transplantation. The diagnosis and grading of aGVHD were based on the Glucksberg (International Bone Marrow Transplant Registry, IBMTR) severity index, whereas cGVHD was diagnosed and classified according to the revised Seattle criteria14,15.
Statistical analysis
Continuous variables with non-normal distribution are presented as medians with ranges or interquartile ranges. For univariate analyses, continuous variables were compared using the Mann–Whitney U test, whereas categorical variables were analyzed using the chi-square test. Kaplan–Meier methods were applied to estimate GRFS, PFS, and OS. Cumulative incidence was calculated for aGVHD, cGVHD, CIR, and NRM, with death treated as a competing risk for CIR, relapse as a competing risk for NRM, and relapse or death as competing risks for aGVHD and cGVHD. Univariate comparisons of GRFS, OS, and PFS were performed using the log-rank test, while the Fine–Gray test was used for univariate analyses of cumulative incidence outcomes.
Multivariate analyses were conducted using Cox proportional-hazards models for survival endpoints and competing-risks regression models for CI outcomes. The final multivariate models included recipient age, disease status before transplantation, GVHD prophylaxis regimen, and the female donor-to-male recipient combination as covariates. A two-sided P value <0.05 was considered statistically significant.
All statistical analyses were performed using SPSS Statistics version 26 (SPSS Inc./IBM, Armonk, NY, USA) and R version 4.3.2 (R Development Core Team, Vienna, Austria). Figures were generated using R version 4.3.2 and GraphPad Prism version 8.4.0 (GraphPad Software, Boston, MA, USA).
Results
Patient characteristics
A total of 114 consecutive recipients who underwent haplo-PBSCT at West China Hospital of Sichuan University between June 2015 and December 2024 were included in this study. Baseline characteristics and transplantation data are summarized in Table 1. The underlying diseases comprised AML/MDS (n = 65), ALL (n = 37), chronic myeloid leukemia (CML, n = 3), and other hematologic malignancies (n = 9).
Characteristics of patients and donors.
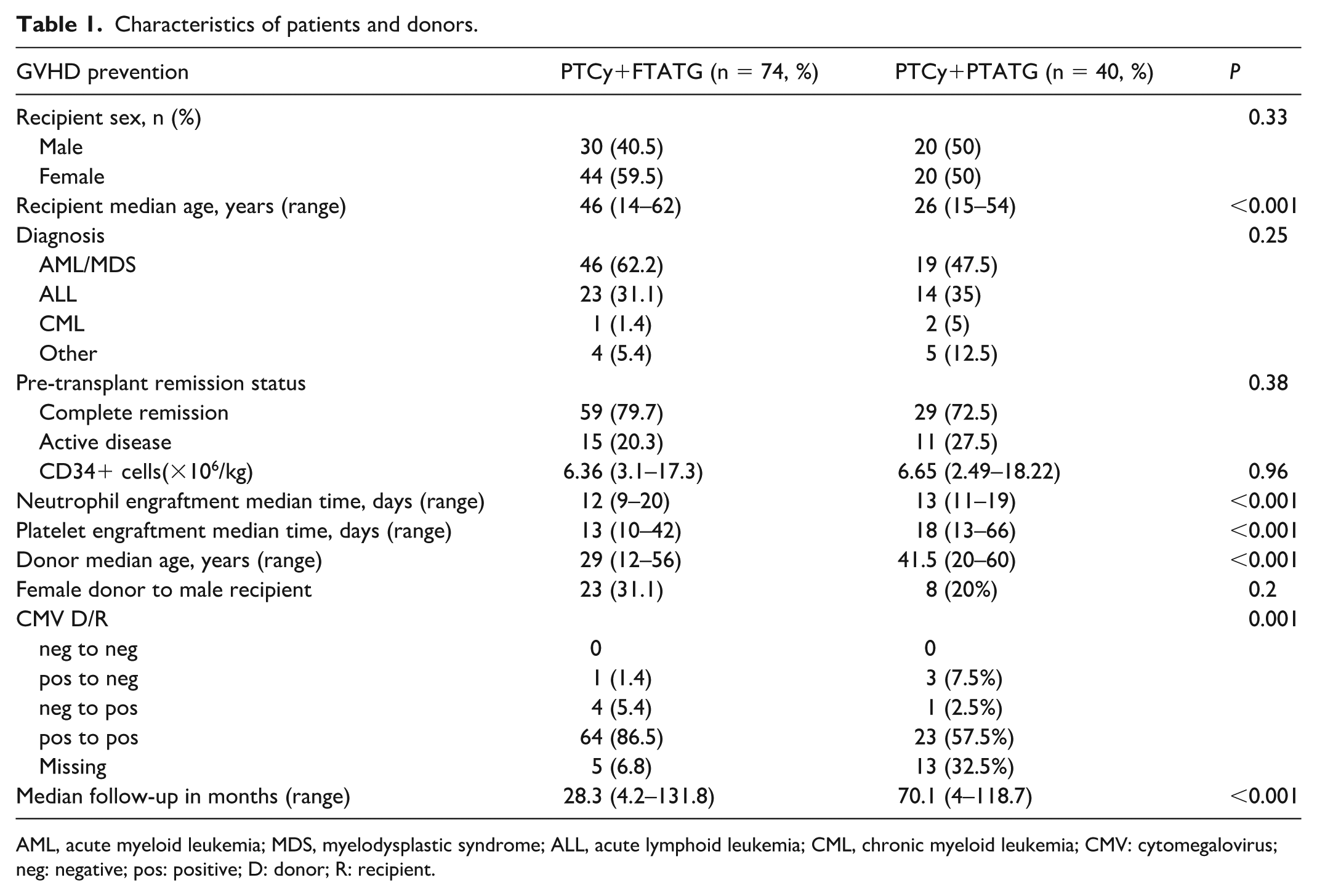
AML, acute myeloid leukemia; MDS, myelodysplastic syndrome; ALL, acute lymphoid leukemia; CML, chronic myeloid leukemia; CMV: cytomegalovirus; neg: negative; pos: positive; D: donor; R: recipient.
The median follow-up duration was 28.3 months (range: 4.2–131.8) in the PTCy+FTATG group (n = 74) and 70.1 months (range: 4.0–118.7) in the PTCy+PTATG group (n = 40). Patients in the PTCy+FTATG group were significantly older than those in the PTCy+PTATG group, with a median age of 46 years (range: 14–62) versus 26 years (range: 15–54), respectively (P < 0.001). In comparison, donors in the PTCy+PTATG group were significantly older than those in the PTCy+FTATG group, with a median age of 41.5 years (range: 20–60) versus 29 years (range: 12–56), respectively (P < 0.001).
No statistically significant differences were observed between the two groups regarding sex distribution, disease category, disease status at transplantation, proportion of female donor-to-male recipient pairs, or infused CD34+ cell dose (all P > 0.05).
Engraftment and GVHD
All patients achieved neutrophil engraftment. The median time to neutrophil recovery was significantly shorter in the PTCy+FTATG group than in the PTCy+PTATG group (12 days, range 9–20 vs 13 days, range 11–19; P < 0.001). Platelet engraftment was achieved in all patients in the PTCy+FTATG group. In comparison, two patients in the PTCy+PTATG group died before platelet recovery, one due to intracranial toxoplasmosis at 5.4 months, and one due to extensive chronic GVHD at 9.4 months. Median time to platelet engraftment was also significantly shorter in the PTCy+FTATG group than that in the PTCy+PTATG group (13 days, range 10–42 vs 18 days, range 13–66; P < 0.001). Complete donor chimerism on day +28 after transplantation was observed in 99.1% of patients (113/114), with only one case of mixed chimerism in the PTCy+PTATG group.
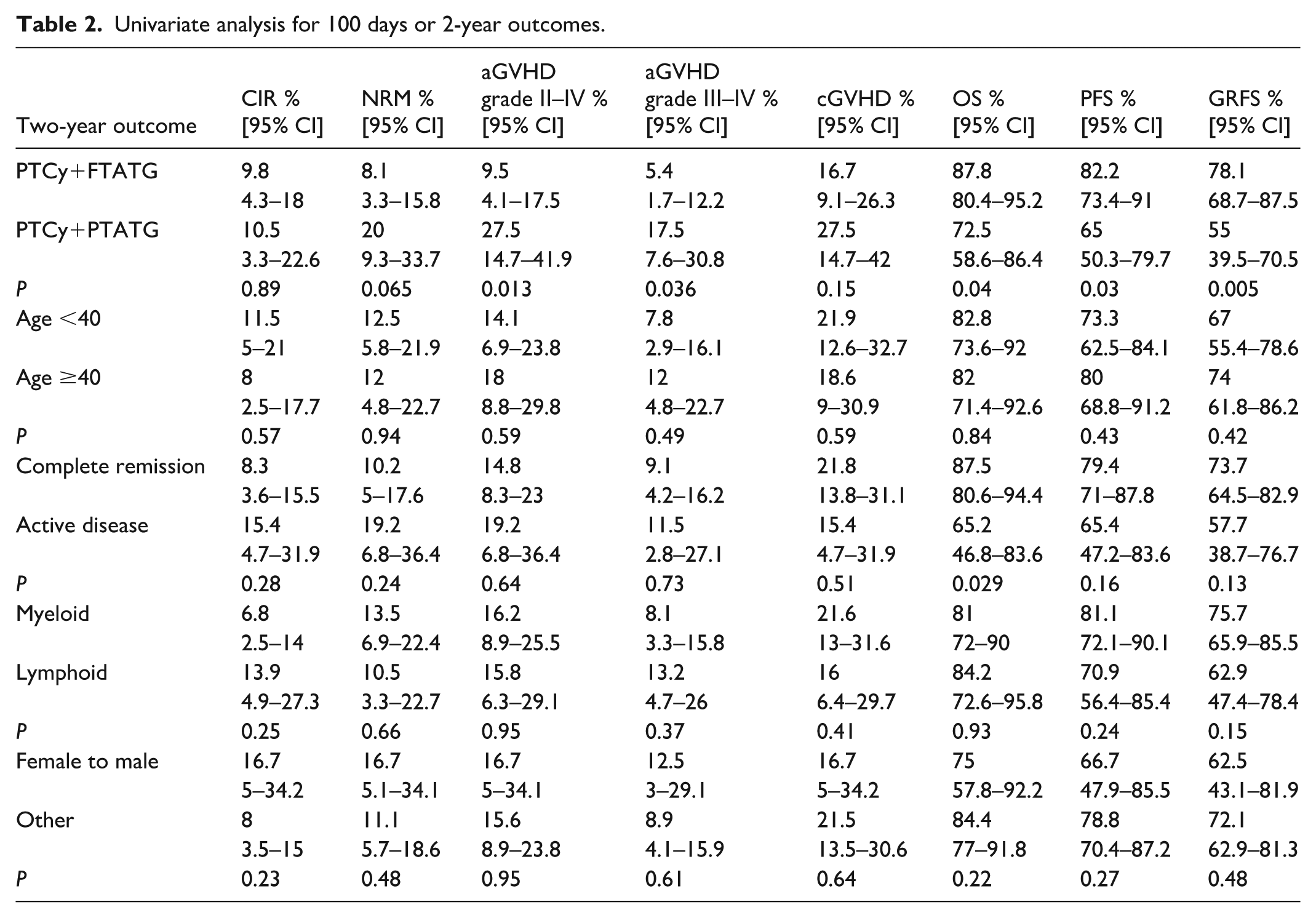
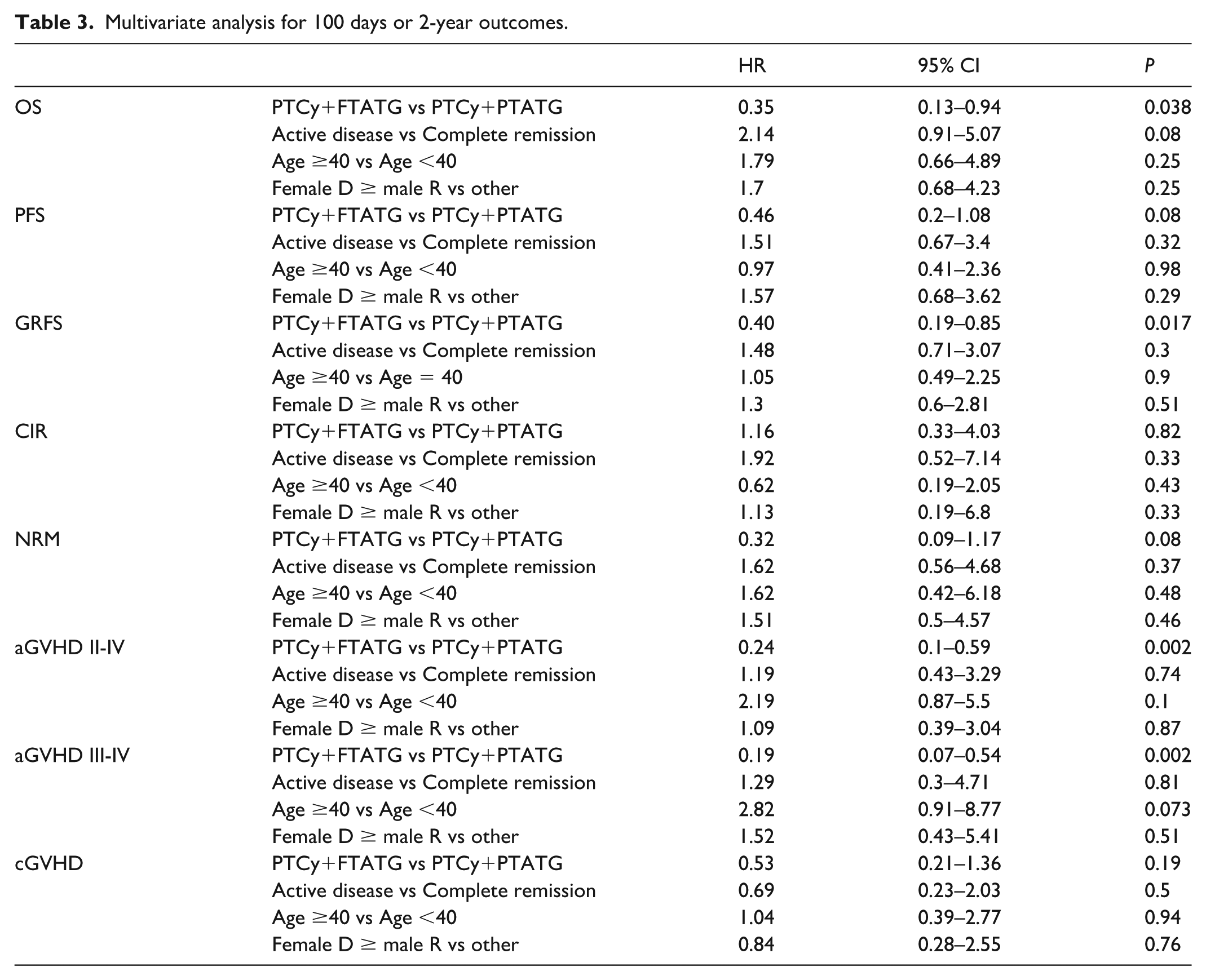
Within 100 days after transplantation, the cumulative incidence of grade II–IV aGVHD was significantly lower in the PTCy+FTATG group than that in the PTCy+PTATG group (9.5% [95% CI: 4.1–17.5] vs 27.5% [95% CI: 14.7–41.9]; P = 0.013). Similarly, the cumulative incidence of grade III–IV aGVHD was significantly lower in the PTCy+FTATG group (5.4% [95% CI: 1.7–12.2] vs 17.5% [95% CI: 7.6–30.8]; P = 0.036). Multivariate analysis confirmed that the PTCy+FTATG regimen was associated with a significantly reduced risk of both grade II–IV aGVHD (HR 0.24; 95% CI: 0.10–0.59; P = 0.002) and grade III–IV aGVHD (HR 0.19; 95% CI: 0.07–0.54; P = 0.002).
The 2-year cumulative incidence of cGVHD was 16.7% (95% CI: 9.1–26.3) in the PTCy+FTATG group and 27.5% (95% CI: 14.7–42.0) in the PTCy+PTATG group, with no statistically significant difference between groups (P = 0.15). No cases of extensive cGVHD occurred in the PTCy+FTATG group, whereas two cases, including one fatal event, were reported in the PTCy+PTATG group. Detailed GVHD outcomes are presented in Table 2.
Univariate analysis for 100 days or 2-year outcomes.
Survival
Univariate and multivariate analyses showed no significant differences in NRM or CIR according to the GVHD prophylaxis regimen (PTCy+FTATG vs PTCy+PTATG), recipient age, disease type, disease status, or donor–recipient sex combination. The 2-year NRM was 8.1% (95% CI: 3.3–15.8) in the PTCy+FTATG group and 20.0% (95% CI: 9.3–33.7) in the PTCy+PTATG group (P = 0.065; multivariate HR 0.32; 95% CI: 0.09–1.17; P = 0.08). The corresponding 2-year CIR rates were 9.8% (95% CI: 4.3–18.0) and 10.5% (95% CI: 3.3–22.6), respectively (P = 0.89; multivariate HR 1.16; 95% CI: 0.33–4.03; P = 0.82).
Infection was the most common cause of NRM, accounting for 57.1% of cases. At 2 years after transplantation, the PTCy+FTATG group demonstrated significantly better outcomes than the PTCy+PTATG group in terms of OS (87.8% vs 72.5%, P = 0.04), PFS (82.2% vs 65.0%, P = 0.03), and GRFS (78.1% vs 55.0%, P = 0.005).
Multivariate analysis identified the PTCy+FTATG regimen as an independent protective factor for both OS (HR 0.35; P = 0.038) and GRFS (HR 0.40; P = 0.017). Detailed survival outcomes and causes of death are presented in Tables 2 and 3, Supplemental Table 1, and Figures 1 and 2.
Multivariate analysis for 100 days or 2-year outcomes.
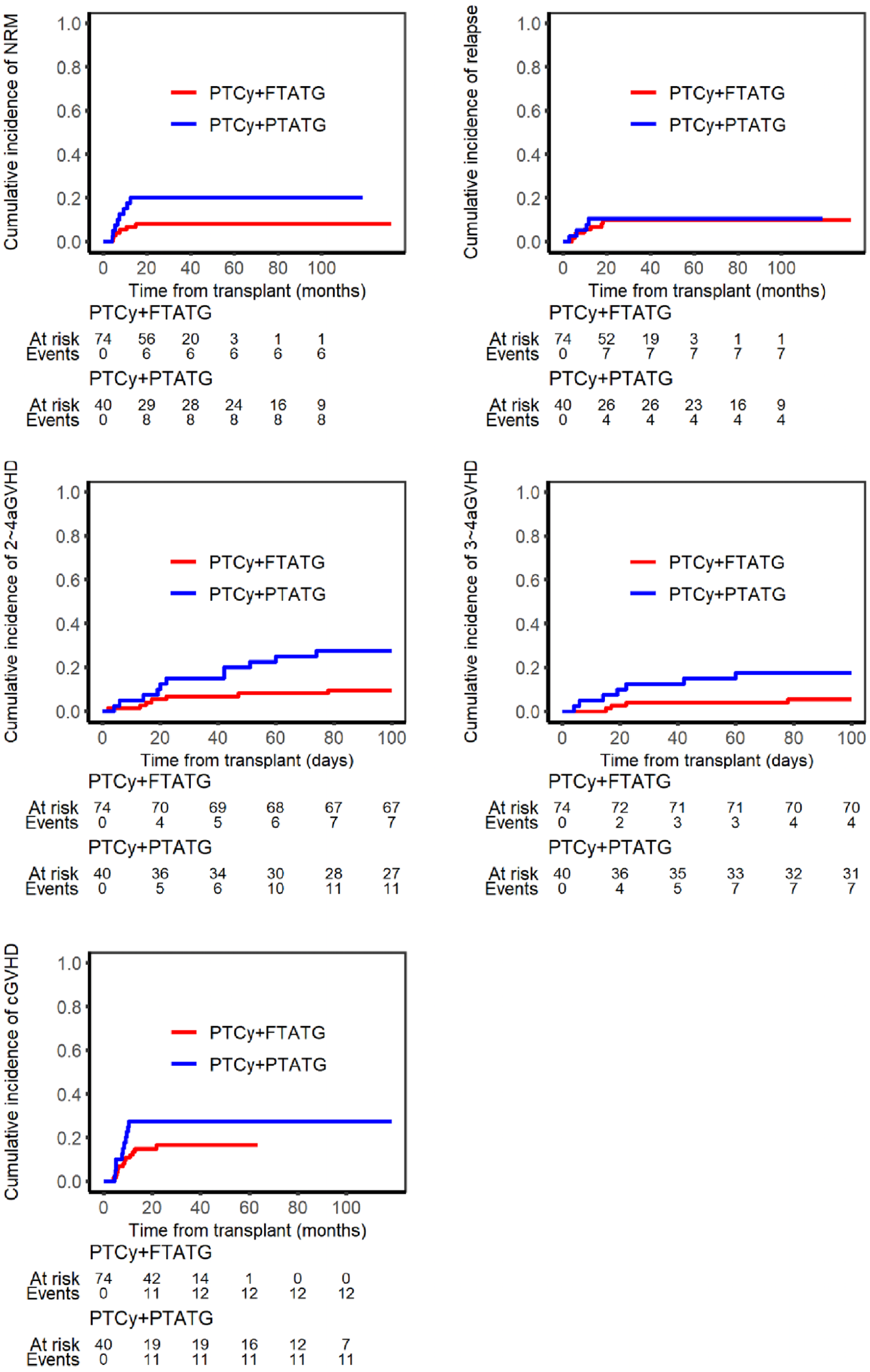
Cumulative incidence of NRM, relapse, and GVHD after transplantation in the PTCy+FTATG and PTCy+PTATG groups.
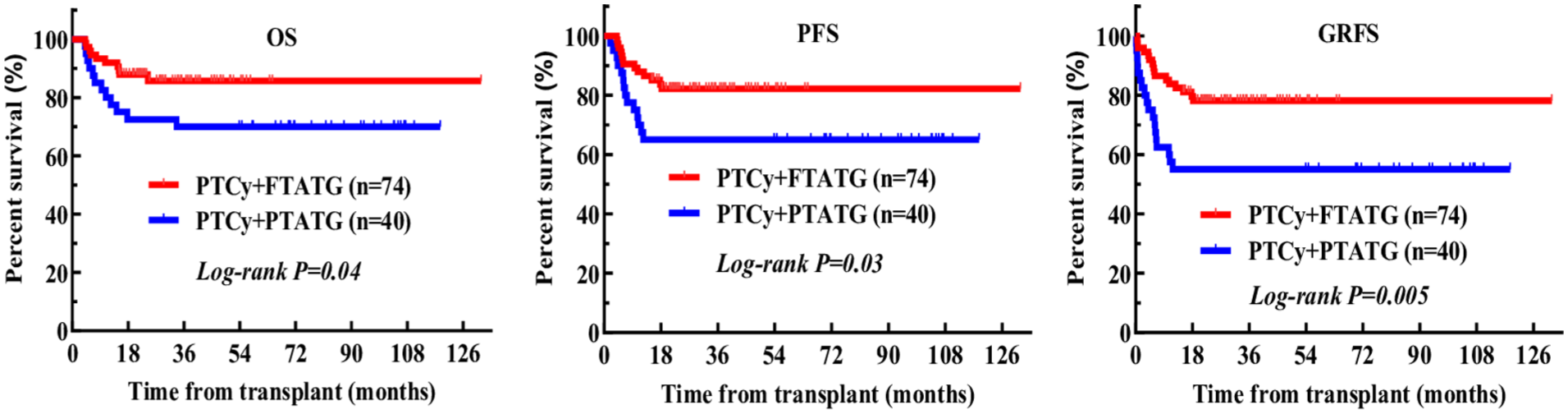
Survival outcomes in the PTCy+FTATG and PTCy+PTATG groups.
T lymphocyte reconstitution, infection, and hemorrhagic cystitis
Post-transplant T-lymphocyte subset recovery was monitored by flow cytometry (Figure 3, Supplemental Table 2). Baseline T-cell subset levels were comparable between the two groups. Both groups showed rapid recovery of CD3+ and CD8+ T-cell counts, which returned to the normal range within 6 months, with similar recovery kinetics in both cohorts.
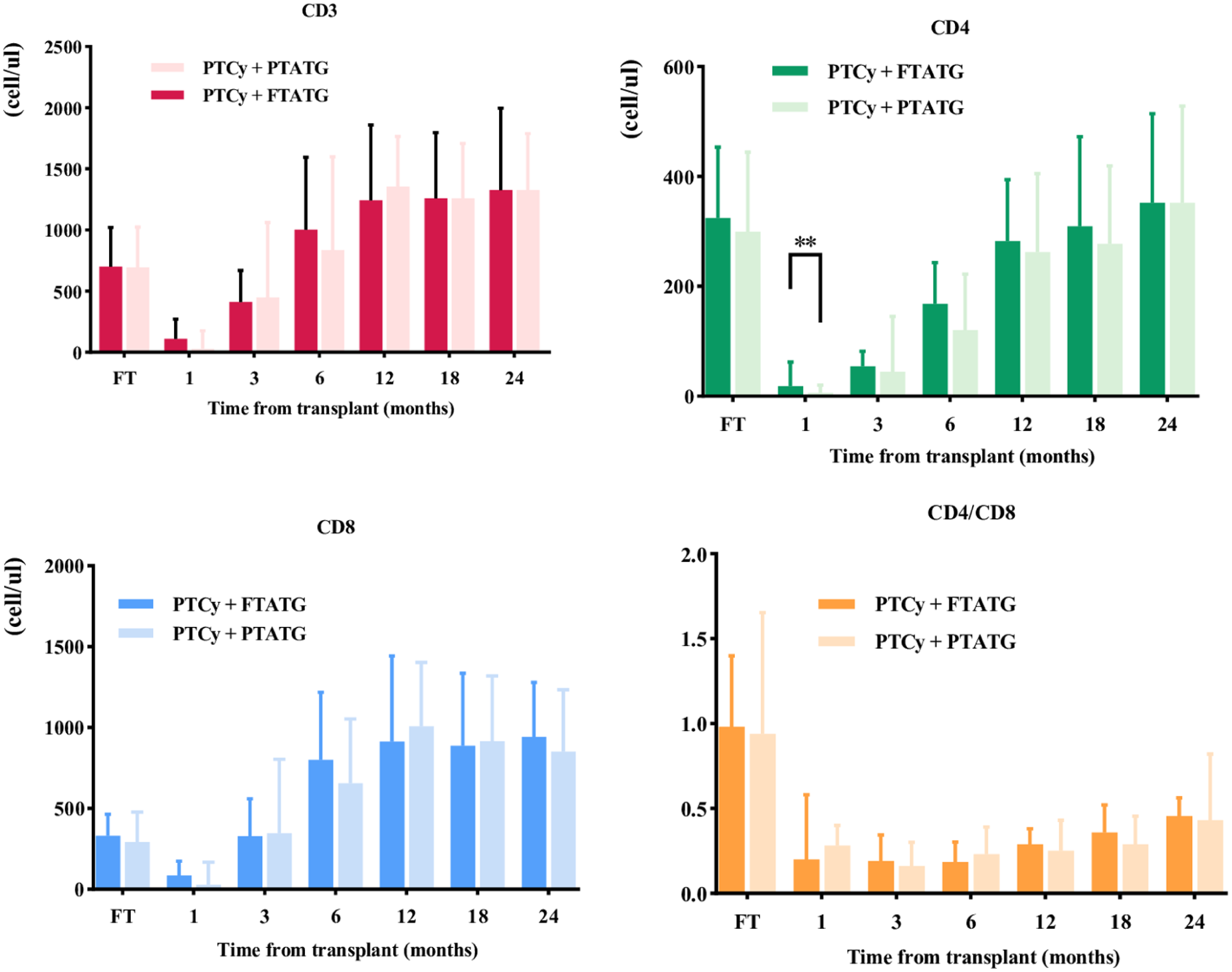
Recovery of T lymphocyte subsets after transplantation in the PTCy+FTATG and PTCy+PTATG groups.
CD4+ T-cell recovery was slower in both groups and remained below the normal reference threshold (385 cells/μL) even at 2 years. However, the PTCy+FTATG group had significantly higher CD4+ counts at 1 month after transplantation (median 18 vs 6 cells/μL, P = 0.008). Thereafter, recovery patterns were similar, with median CD4+ counts exceeding 200 cells/μL by 1 year in both groups. The CD4+/CD8+ ratio remained inverted (<0.5) throughout the 2-year follow-up period, with no significant difference between groups.
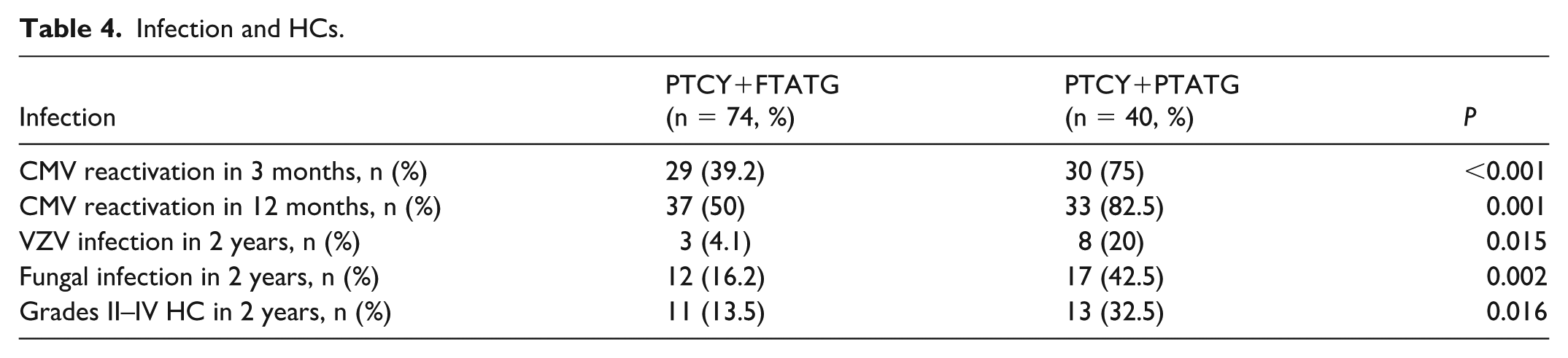
Infectious complications are summarized in Table 4. The PTCy+FTATG group had significantly lower cytomegalovirus (CMV) reactivation rates than the PTCy+PTATG group at both 3 months and 12 months (39.2% vs 75.0%, P < 0.001; and 50.0% vs 82.5%, P = 0.001, respectively). Similarly, the PTCy+FTATG group showed significantly lower 2-year incidences of varicella-zoster virus (VZV) infection (4.1% vs 20.0%, P = 0.015), breakthrough fungal infection (16.2% vs 42.5%, P = 0.002), and grade II–IV hemorrhagic cystitis (HC; 13.5% vs 32.5%, P = 0.016).
Infection and HCs.
Discussion
Although the combination of PTCy and ATG has been investigated in haploidentical transplantation, the optimal timing of ATG administration remains uncertain, particularly in the setting of MAC using PBSCs. Therefore, this study directly compared pre-transplant (FT) versus post-transplant (PT) ATG when combined with PTCy for GVHD prophylaxis in patients undergoing MAC haplo-PBSCT. In contemporary haploidentical transplantation, PTCy reduces GVHD primarily by selectively eliminating alloreactive T cells and promoting the recovery of regulatory T cells (Tregs). In comparison, ATG exerts immunosuppressive effects mainly by depleting T cells and modulating dendritic cells16–20. However, in MAC PBSC transplantation, the use of either high-dose PTCy or ATG alone is still associated with considerable rates of grade II–IV aGVHD and cGVHD4,6. High-dose PTCy has also been linked to delayed engraftment, cardiotoxicity, HC, and increased infection risk21–23, while high-dose ATG may delay immune reconstitution and increase infectious complications24,25. Therefore, combining PTCy with ATG may provide complementary or synergistic protection against GVHD, and lowering the dose of each agent may help reduce treatment-related toxicity. A recent meta-analysis showed that, compared with ATG or PTCy alone, the combination of PTCy plus ATG significantly reduced aGVHD incidence and improved survival after haploidentical transplantation without increasing relapse 26 . The principal finding of this study is that half-dose PTCy (25 mg/kg/day on days +3 and +4) combined with pre-transplant low-dose ATG (total 5 mg/kg on days −3 to −1) (PTCy+FTATG) was superior to high-dose PTCy (50 mg/kg/day on days +3 and +4) plus post-transplant low-dose ATG (2.5 mg/kg on day +8) (PTCy+PTATG). The PTCy+FTATG regimen significantly reduced the incidence of grade II–IV aGVHD (9.5% vs 27.5% [HR 0.24; 95% CI: 0.10–0.59; P = 0.002]) and grade III–IV aGVHD (5.4% vs 17.5% [HR 0.19; 95% CI: 0.07–0.54; P = 0.002]), while improving OS (87.8% vs 72.5% [HR 0.35; 95% CI: 0.13–0.94; P = 0.038]) and GRFS (78.1% vs 55.0% [HR 0.46; 95% CI: 0.20–1.08; P = 0.08]). Furthermore, neutrophil and platelet engraftment occurred more rapidly in the PTCy+FTATG group. This regimen also significantly reduced major infectious complications, including CMV reactivation at 3 and 12 months after transplantation (39.2% vs 75.0%, P < 0.001; 50.0% vs 82.5%, P = 0.001, respectively), breakthrough fungal infection (16.2% vs 42.5%, P = 0.002), VZV reactivation (4.1% vs 20.0%, P = 0.015), and grade II–IV HC (13.5% vs 32.5%, P = 0.016). Although the overall CMV reactivation rate remained high, this likely reflects established risk factors such as haploidentical transplantation, ATG exposure, and intensive surveillance with biweekly CMV-DNA monitoring; however, no CMV end-organ disease was observed27–31. Within the PTCy+FTATG subgroup, letermovir prophylaxis appeared capable of reducing CMV reactivation to 31.9% (15/47).
These favorable outcomes may be explained by mechanistic synergy between PTCy and ATG, together with optimized timing and dosing. Early administration of ATG may more effectively deplete alloreactive T cells, while reducing the PTCy dose to 25 mg/kg/day, within a reported effective range for GVHD prevention with lower toxicity 17 , likely lessening myelosuppression, delayed immune recovery, and HC associated with the conventional 50 mg/kg/day regimen. At the same time, using a lower total ATG dose (5 mg/kg) before transplantation may have facilitated faster immune reconstitution and reduced the risk of opportunistic infections. The PTCy+FTATG regimen did not increase NRM or cumulative relapse incidence compared with either the PTCy+PTATG cohort or previously reported studies of PTCy-ATG combinations8–12. Despite the older median age in the PTCy+FTATG group (46 vs 26 years), outcomes remained favorable, with superior OS and GRFS. A similar positive trend was also seen for PFS (82.2% vs 65.0% [HR 0.46; 95% CI: 0.20–1.08; P = 0.08]). The aGVHD rate in the PTCy+FTATG group was lower than that in most reported PTCy plus ATG regimens in both the MAC and RIC haplo-HCT groups, while its cGVHD incidence (16.7% [95% CI: 6.1–28.5]) was also favorable 8–12. The neutrophil and platelet engraftment times in the PTCy+FTATG group were shorter than those reported in other studies using PTCy, ATG, or PTCy+ATG 9,18,19,32.
Several limitations should be acknowledged. First, the retrospective single-center design introduces the possibility of selection bias. Second, heterogeneity in conditioning regimens may have confounded the results. However, the consistent differences observed in major clinical outcomes between the two prophylactic strategies support the reliability of the main findings. Larger prospective multicenter studies, together with mechanistic investigations, are needed to validate these results and determine their broader applicability.
Conclusion
In summary, half-dose PTCy combined with pre-transplant low-dose ATG (PTCy+FTATG) appears to effectively address key challenges in GVHD prophylaxis for MAC haplo-PBSCT. Through complementary immunologic mechanisms and optimized timing/dosing, this strategy significantly reduces aGVHD and selected infectious complications, accelerates hematopoietic recovery, and demonstrates encouraging tolerability with favorable survival outcomes, including in older patients. These findings support its potential as a promising prophylactic approach for GVHD prevention.
Supplemental Material
sj-xls-1-cll-10.1177_09636897261454024 – Supplemental material for Comparison of the efficacy of pre-transplant and post-transplant antithymocyte globulin combined with post-transplant cyclophosphamide for graft-versus-host disease prophylaxis in myeloablative haploidentical peripheral blood stem cell transplantation
Supplemental material, sj-xls-1-cll-10.1177_09636897261454024 for Comparison of the efficacy of pre-transplant and post-transplant antithymocyte globulin combined with post-transplant cyclophosphamide for graft-versus-host disease prophylaxis in myeloablative haploidentical peripheral blood stem cell transplantation by Xuelian Jin, Tian Dong, Jie Ji, Zhigang Liu, Pu Kuang, Jian Li, Yu Wu, Juan Xu, Zerong Wang, Jiajia Zeng, Zilin Xiong and Xinchuan Chen in Cell Transplantation
Supplemental Material
sj-xls-2-cll-10.1177_09636897261454024 – Supplemental material for Comparison of the efficacy of pre-transplant and post-transplant antithymocyte globulin combined with post-transplant cyclophosphamide for graft-versus-host disease prophylaxis in myeloablative haploidentical peripheral blood stem cell transplantation
Supplemental material, sj-xls-2-cll-10.1177_09636897261454024 for Comparison of the efficacy of pre-transplant and post-transplant antithymocyte globulin combined with post-transplant cyclophosphamide for graft-versus-host disease prophylaxis in myeloablative haploidentical peripheral blood stem cell transplantation by Xuelian Jin, Tian Dong, Jie Ji, Zhigang Liu, Pu Kuang, Jian Li, Yu Wu, Juan Xu, Zerong Wang, Jiajia Zeng, Zilin Xiong and Xinchuan Chen in Cell Transplantation
Footnotes
Acknowledgements
Ethical considerations
The study protocol was approved by the Ethics Committee on Biomedical Research, West China Hospital of Sichuan University (approval no. 2019-993, approval date 15/11/2019) and was conducted in accordance with the Declaration of Helsinki.
Author contributions
XLJ was responsible for writing the report, extracting and analyzing the data, and interpreting the results. XCC was responsible for designing the study protocol, screening potentially eligible patients, supervising the research, and revising the report. TD, JJ, ZGL, KP, and JL were responsible for designing the protocol and screening potentially eligible patients. ZRW, JJZ, and ZLX contributed to data extraction. YW and JX were responsible for interpreting the results and providing critical feedback on the report.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work was supported in part by the Clinical Research Incubation Project, West China Hospital, Sichuan University (grant no. 2022HXFH031).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statements
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
Statement of human and animal rights
This article does not contain any studies with human or animal subjects.
Statement of informed consent
Written informed consent was obtained from all patients before transplantation.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.