
Abstract
A descriptive qualitative study was conducted to explore risk perception, self-management challenges, and coping strategies among Chinese hematopoietic stem cell transplantation (HSCT) patients, using the Health Action Process Approach (HAPA) as the guiding framework. Purposive sampling, based on the principle of information power, was employed to recruit 20 HSCT patients from a hospital in south-central China between May and August 2024. The HAPA model informed the development of semi-structured interview questions, and the data were analyzed using a combination of thematic analysis and framework analysis. The findings indicate that both risk perception and self-efficacy play a critical role in motivating patient engagement in self-management. Main barriers to self-management included difficulties in symptom control, lifestyle modification, psychological adjustment, and healthcare-related financial burdens. Effective coping strategies reported by participants involved the use of digital tools, seeking professional medical advice, maintaining self-management journals, and drawing on family and social support networks. In clinical practice, healthcare professionals may capitalize on the heightened risk perception and self-efficacy during the peri-transplant period to promote the transition from risk perception to actionable self-management behaviors. In contrast, during the early post-discharge phase, when both risk perception and self-efficacy tend to decline, tailored support systems and resource allocation are helpful for maintaining the transition from risk perception to self-management action.

Keywords
Introduction
Hematopoietic stem cell transplantation (HSCT) is well-established treatment for malignant hematological diseases, aplastic anemia, genetic blood disorders, and other conditions 1 . In China, 39,918 HSCT procedures were reported over the past 2 years 2 . Among patients with malignant hematological diseases undergoing matched sibling donor allogeneic HSCT (MSD allo-HSCT), the 1-year overall survival rate is 74.1% 3 , with a 3-year survival rate for grade II–IV graft-versus-host disease (GVHD) of approximately 45% 4 . Despite these outcomes, HSCT entails a prolonged recovery period characterized by significant challenges, including immunosuppression, increased infection risk, adverse reactions to immunosuppressive drugs, disease relapse, and transplant-related complications5–7. These factors impair patients’ quality of life, complicate prognosis, increase healthcare costs, and pose life-threatening risks 8 .
The success of HSCT depends on a multifaceted effort that includes advances in medical technology, high-quality supportive care, and active patient self-management. Self-management refers to the day-to-day activities and decisions patients use to manage chronic conditions 9 . In this study, self-management encompasses managing symptoms, adhering to complex treatment regimens, addressing both physiological and psychosocial consequences of the disease, monitoring changes in health status, and communicating effectively with healthcare providers. Effective post-HSCT self-management is a major determinant of outcomes, including control of GVHD, prevention of infection, medication adherence, and quality of life.
HSCT patients often experience prolonged recovery periods and face complex self-management tasks. Approximately 60%–90% of allogeneic HSCT patients develop long-term complications, such as GVHD, infections, neurocognitive deficits, and hypogonadism. These complications necessitate ongoing follow-up to monitor for recurrence and prevent further progression10,11. Effective self-management involves the use of self-regulation strategies, including goal setting, self-monitoring, and problem-solving, to manage both the disease and its associated risk factors 12 . However, patients frequently encounter barriers such as inadequate medical information, psychological distress, financial constraints, and geographic disparities in healthcare access, all of which complicate effective self-management13–15.
Current research on post-discharge self-management among HSCT patients has largely relied on quantitative designs and focused primarily on biomedical interventions. These approaches have yielded valuable estimates of symptom prevalence and self-reported behaviors but provide limited insight into the subjective experiences, contextual influences, and dynamic decision-making that underlie self-management16,17. This gap underscores the need for qualitative inquiry to elucidate how such behaviors are perceived, adopted, and sustained.
Risk perception, defined as an individual’s subjective judgment of disease susceptibility, is an important predictor of health behaviors and self-management 18 . Among people with type 2 diabetes, Li et al. 19 discovered that higher perceived risk was associated with greater self-management, suggesting that risk perception may precede behavior change. In a UK-based study, reflective-deliberative risk perception negatively predicted intention, whereas affective-experiential risk perception positively predicted intention 20 . This heterogeneity underscores the need to examine how different forms of perceived risk are constructed and enacted in everyday self-management.
According to the Health Action Process Approach (HAPA) model, risk perception is a core factor in initiating behavior change during the intention-to-change stage. In the context HSCT, the persistent risks of disease recurrence and GVHD highlight the need for a deep understanding of how risk perception influences self-management behaviors, such as dietary control, medication adherence, and symptom monitoring. However, there is a lack of in-depth exploration of how risk perception drives these behaviors, especially considering the influence of psychobehavioral stages and cultural contexts. Using qualitative methods 21 , this study aims to apply the HAPA framework to examine the self-management process among Chinese HSCT patients, from the intention to take action, through action, and into maintenance22,23. By integrating patients lived experiences with a theoretical framework, this study will provide a comprehensive understanding of how risk perception, motivation, and coping strategies influence self-management behaviors.
Methods
Design
The study employed a qualitative descriptive design and conducted semi-structured interviews with post-HSCT patients. The thematic analysis24,25 was used to analyze the interview data. Descriptive qualitative research, rooted in the philosophy of naturalistic inquiry, aims to produce straightforward descriptions of phenomena as they occur in their natural state, minimizing interpretive inference 26 .
The interviews were conducted by H.Y., a specialist nurse in stem cell transplantation with a postgraduate degree and substantial experience in qualitative research and interviewing techniques. Her in-depth understanding of the treatment and recovery processes of the study participants contributed to the reliability and richness of the data collected. Conducted from May to August 2024, this study received approval from the Institutional Ethics Committee of the Second Xiangya Hospital of Central South University (No.2024-0275). In addition, the study adhered to the Consolidated Criteria for Reporting Qualitative Studies (COREQ) checklist 27 .
Sampling and participants
The participants were selected using a purposive sampling approach combined with maximum variation in terms of age, gender, financial status, self-health status, disease type, HSCT types, and duration after HSCT. Post-HSCT patients, treated and reviewed at a tertiary teaching hospital in Hunan Province, were recruited by the nurse in charge of a specialized outpatient clinic. The researcher (H.Y.) approached eligible patients, obtained informed consent, conducted all interviews, and oversaw standardized data collection. Sample size was guided by the information power framework, considering the study’s narrow aim, high sample specificity, strong interview dialogue, and a case-focused analytic strategy 28 .
Inclusion criteria were (1) post-HSCT patients who had been discharged and had at least 2 months of independent home-based self-management, (2) at least 18 years old, (3) ability to understand and speak Chinese, and (4) willingness to discuss their experiences with HSCT self-management. Exclusion criteria were (1) current psychiatric disease, (2) cognitive impairment, and (3) language barriers.
Data collection
Between May and August 2024, we screened 35 patients from the HSCT outpatient clinic of the Hematology Department by using electronic medical records. Of these, 22 met all inclusion criteria. Exclusions included 8 patients with ineligible transplant types, 3 who refused participation, 2 with language barriers. Of the 22 eligible participants, 20 completed interviews (1 declined due to discomfort, and 1 withdrew due to scheduling conflicts). Data collection was stopped once information saturation was reached, which was confirmed through repeated coding: no new themes emerged in the last three consecutive interviews. The final sample size (n = 20) is consistent with the principles of purposive sampling and information saturation in qualitative research.
Included patients had three types of hematological malignancies: acute leukemia, lymphoma, and myelodysplastic syndrome. All participants underwent allogeneic hematopoietic stem cell transplantation (allo-HSCT), which was classified into three subtypes based on HLA matching: haploidentical HSCT, HLA-identical HSCT, and 10/10 matched unrelated donor (MUD) HSCT. Patients’ self-reported health status was categorized into three levels: (1) Good: no physical discomfort, normal daily activities, and no need for regular medical intervention; (2) Moderate: mild occasional discomfort with minimal impact on daily activities; (3) Poor: persistent or significant discomfort impairing daily activities and potentially requiring regular medical care. Financial status was assessed based on monthly family income (RMB), with three categories: <5000, 5000–10,000, and >10,000.
Data were collected through face-to-face semi-structured interviews conducted in Chinese. Before each interview, we explained the study aims, procedures, and interview topics to participants and established rapport. All participants provided written informed consent, including consent for audio recording and note-taking. Interviews were conducted one-on-one in a private office, with only the participant and the interviewer (H.Y.) present.
Each participant was interviewed for 20–40 min. During the interviews, participants described their experiences and needs regarding post-discharge self-management. The interview guide was developed on the basis of the HAPA framework and a review of literature. Following two pilot interviews with post-HSCT patients, the guide was refined and finalized (see Table 1).
Semi-structured interview guide.

The interviews began with an open-ended question about patients’ perceptions and feelings about their condition after HSCT. The researcher recorded the interviews both audibly and through note-taking. By observing the interviewees’ non-verbal cues, the researcher followed up with appropriate questions while avoiding leading questions. Before concluding, participants were invited to add or clarify any additional information. The interviews were transcribed verbatim within 24 h, and participants were assigned codes (e.g. P1 = Participant 1) to ensure anonymity. The transcripts were uploaded to NVivo12 (QSR International) for qualitative analysis.
Data analysis
Thematic analysis 29 and HAPA framework analysis 30 were applied to identify emerging themes and assign them to pre-selected theoretically driven domains, thus facilitating the identification of psychological and behavioral changes in the self-management process.
Step 1: Familiarization. Two researchers, Z.X. and H.Y., extracted the audio data from the recording device and transcribed it into text. They then proofread, summarized, and organized the data into interview transcripts. Step 2: Generating Codes. The interview transcripts were thoroughly read, and key words, phrases, or sentences were identified and assigned preliminary codes. Step 3: Constructing Themes. Preliminary codes were compared and grouped based on similarity, and major categories were created using a thematic map. These themes were then mapped deductively to the HAPA framework. Step 4: Revising Themes. Themes were reviewed against the dataset, with similar or related themes grouped together for revision. Step 5: Defining Themes. The naming and descriptions of the themes clarified their content and scope. Step 6: Producing the Report. A report was written based on the identified themes, incorporating relevant literature to explain and justify them. Anonymized quotes were used to illustrate the core meaning of the themes.
Three researchers (X.L., H.Y., and X.Y.) independently coded the data. H.Y. and X.Y. both nursing professors with extensive experience in nursing management and hematology care, work at a hospital and a university, respectively. This collaborative approach ensured that the final report would be comprehensive and credible.
Results
Participant characteristics
This study employed the HAPA framework to conduct semi-structured interviews with 20 post-HSCT patients. Participants’ ages ranged from 18 to 61 years, with a mean age of 37.8 years. Among these 20 participants, 16 were diagnosed with acute leukemia, 2 with lymphoma, and 2 with myelodysplastic syndromes. Time post-HSCT ranged from 3 to 41 months, with a mean of 16.6 months. Detailed characteristics of the study participants are presented in Table 2.
Characteristics of HSCT patients (n = 20).

The analysis of the interview data revealed 7 themes and 12 subthemes across two phases: motivational phase (risk perception, outcome expectations, action self-efficacy) and volitional phase (action planning, coping strategies, maintenance self-efficacy, recovery self-efficacy).
The results showed that HSCT patients’ risk perception followed a phased pattern. During the peri-transplant period, patients exhibited heightened awareness of life-threatening risks, which coincided with increased action self-efficacy, thereby fostering strong adherence to medical instructions. However, as risk perception decreased upon discharge, self-management behaviors declined. When complications such as GVHD emerged, risk perception increased again, leading to the restoration and maintenance of self-management behaviors. Main barriers to self-management included difficulties in symptom control, lifestyle modification, psychological adjustment, and healthcare-related financial burdens. Effective coping strategies reported by participants involved the use of digital tools, seeking professional medical advice, maintaining self-management journals, and drawing on family and social support networks (see Graph 1, Table 3).
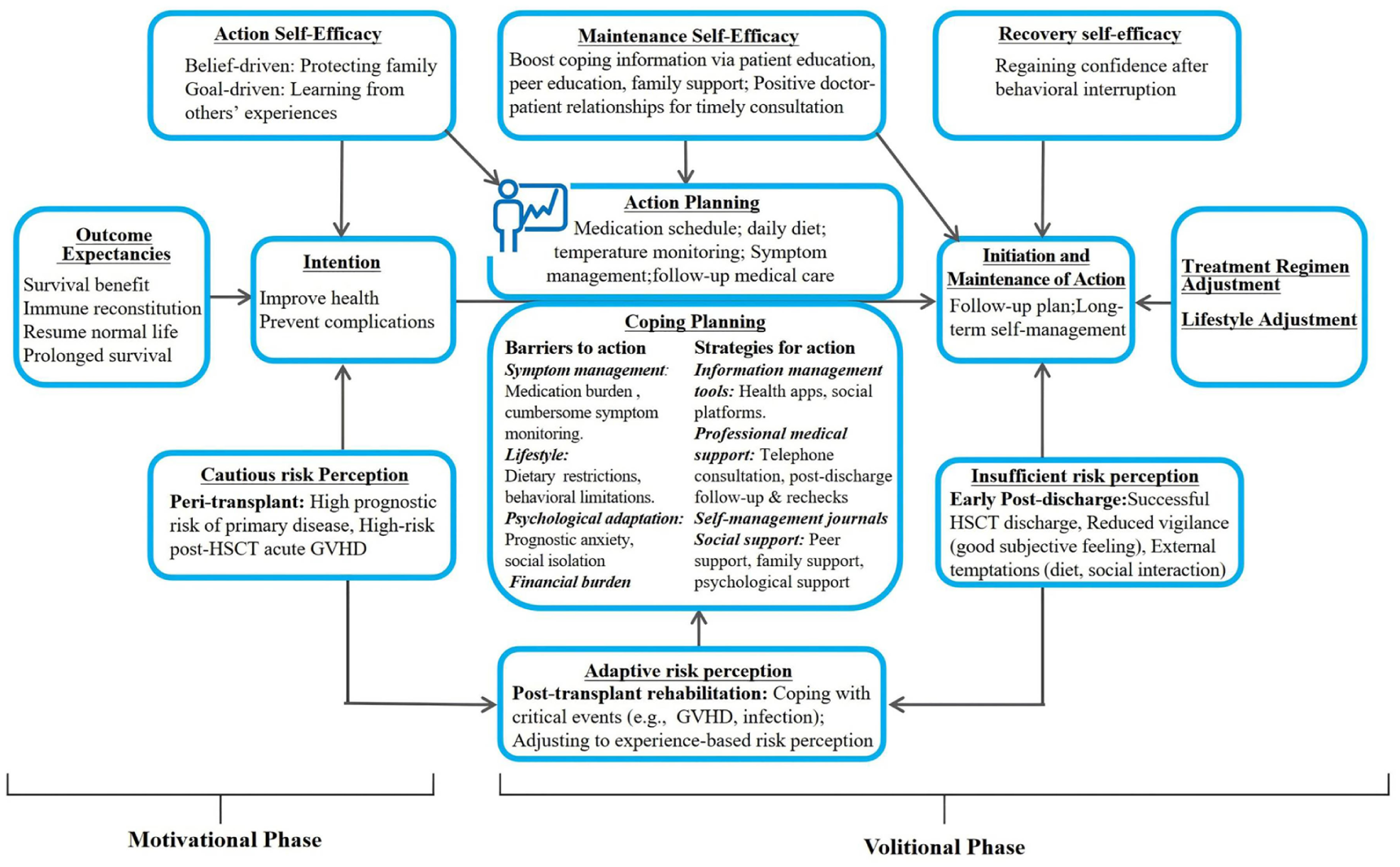
HAPA-guided conceptual model of self-management for HSCT patients.
Summary of themes and sub-themes.

Risk perception
The analysis of the interview data identified three primary types of risk perception among post-HSCT patients: cautious, insufficient, and adaptive. This typology was based on participants’ detailed accounts of their experiences.
Cautious risk perception
During the peri-transplant period (from hospital admission to pre-discharge), patients are exposed to several HSCT-specific high-risk factors, including ultra-high-dose chemotherapy preparation, transplant failure, and GVHD. As a result, their perceived risks were heightened. Patients subjectively assessed their disease susceptibility and severity as extremely high, leading to increased alertness, anxiety, and fear.
“The pre-transplant discussion was jarring. They said if the transplant failed, complications could even be fatal. I went into it with a gambler’s resolve—if it worked, it’d be a win.” (P9) “Once in the transplant isolation ward, I was stuck there all day, I began to feel vulnerable and had no choice but to follow the doctors’ and nurses’ orders.” (P3)
Insufficient risk perception
Some participants’ overdependence on clinicians and their prior experiences mpaired their ability to accurately perceive risks. “Since contracting this disease was uncontrollable, I left it to fate. Regardless of the risks, doctors would handle everything, so I just needed to follow their instructions” (P19).
Adaptive risk perception
Post-transplant risk perception followed a phased pattern, initially decreasing and then gradually increasing. “I was fully cooperative throughout the transplant process. However, after the transplant, I couldn’t resist meeting friends, causing flu-triggered GVHD. Now I’ll strictly follow medical rules” (P17).
Outcome expectancies
Outcome expectations refer to a patient’s evaluation of the potential outcomes and effects of specific behaviors.
Positive outcome expectancies
I held to one hope: if I strictly adhered to the doctors’ instructions—disinfecting, isolating, resisting cravings—I would regain a normal life. (P2)
Negative outcome expectancies
I anticipated constant vomiting from immunosuppressants, but mild nausea actually increased my confidence in taking them on time. (P7)
Action self-efficacy
Patients in the peri-transplant period demonstrated high action self-efficacy, driven by survival imperatives, though some expressed doubts about their ability to manage their health in the long term.
High action self-efficacy
“In the ward, one thought kept me going: my son was waiting for me, and I was determined to overcome the disease.” (P1) “Every morning, I would say, Welcome, stem cells, into my body. Let’s work together to complete the treatment.” (P20)
Low action self-efficacy
I’m not sure if I can stick to the diet long-term. It’s just too hard. (P18)
Action planning
Formulating specific action plans serves as a premise for translating health behavior goals into practice. However, some patients challenge due to inertia, forgetfulness, and competing demands. “I posted my medication schedule on the fridge and set three phone alarms. When they ring, I take the pills immediately. This method helped me avoid missing any doses for half a year” (P5).
Coping planning
Barriers to action
Although post-HSCT patients initiate self-management behaviors, they continue to face a series of barriers to action, which become more pronounced as the post-discharge period extends. (1) Managing disease- and transplant-related symptoms: a significant medication burden, persistent symptoms that interfere with daily life, and avoidance of invasive follow-up examinations. (2) Adapting to necessary lifestyle changes, including strict dietary restrictions, proves extremely difficult, with non-adherence potentially increasing the risk of severe GVHD. (3) Psychological adjustment: patients frequently experience anxiety about prognosis, concerns about body image, feelings of social isolation, and helplessness stemming from self-management failures. (4) Financial burden: although basic health insurance mitigates part of the financial strain, the financial burden of post-HSCT rehabilitation remains considerable.
These interconnected obstacles collectively impede patients’ self-management capacity.
Barriers to symptom management
“There are too many medications. Keeping track of them feels burdensome. Since the transplant, I have experienced persistent nausea and vomiting, making it difficult to eat without discomfort.” (P14) “After the transplant, I was most afraid of the bone marrow aspiration follow-up check. I put it off as long as possible, so I haven’t had this check-up in the past six months.” (P11)
Barriers to lifestyle modification
Post-transplant diets are stringent. One particular meal was so unappetizing that I indulged in two bites of a scallion pancake. I did not anticipate the subsequent gastrointestinal GVHD, which I now deeply regret. (P9)
Barriers to psychological adjustment
After the transplant, I stayed alone for an extended period, and it seemed that the care from others gradually diminished. I felt excluded by both friends and society, which was deeply distressing. (P10)
Barriers to financial burden
Since the transplantation, my family has exhausted our resources. (P15)
Strategies for action
The interviews indicate that information tools are frequently used to track key milestones and gather health information; however, concerns regarding the reliability of such information often induce anxiety. Patients place significant value on professional medical resources, particularly in medication guidance, symptom monitoring, and adjustments to treatment plans. They indicate that clear communication and peer support play a significant role in improving adherence and confidence. When facing emotional and daily life challenges, patients proactively seek family and social support. Furthermore, using daily life management tools, such as self-management diaries and dietary tracking apps, effectively reduces the risk of complications and strengthens confidence in daily self-management. These strategies facilitate a transition from an intention to engage in self-management to the sustained practice of “I can adhere.”
Use of information tools
“To monitor the number of days post-HSCT, I used a countdown application on my phone.” (P2) “I searched for dietary recommendations post-HSCT on platforms such as TikTok and Little Red Book.” (P5) “When looking up how to take a medication online, I noted conflicting information, which only confused me more.” (P12)
Support from professional medical resources
“A video consultation with healthcare professionals to discuss each medication in detail could improve adherence and ensure proper use.” (P12) “Patient education sessions are particularly helpful, as they introduce us to transplant-related knowledge. Last time, a fellow patient’s sharing made me realized that I need to keep up with self-management.” (P6)
Support from family and social resources
During a period of severe emotional distress, I contacted the psychological crisis hotline. (P16)
Use of tools for daily life management
“I record my daily meals, marking problematic foods in red to avoid eating them later, which has been helpful in preventing the recurrence of diarrhea.” (P3). “I use a video-sharing platform to record my routines. This practice improves my daily management.” (P13).
Maintenance self-efficacy
Maintenance self-efficacy was identified as one of the factors influencing their long-term adherence to care plans and ability to overcome challenges. Some participants expressed confidence in self-management of post-HSCT. “I am not used to receiving care from others; instead, I fear that it might increase the risk of infection. Making a daily checklist for myself and following it makes me feel more at ease” (P4).
Recovery self-efficacy
Patients reported actively adjusting their coping strategies in the face of health fluctuations and reestablished confidence to restart and maintain self-management behaviors.
I felt safe six months after discharge. But last month, sudden gum bleeding and weakness made me stop taking my temperature. My daughter urged me to the hospital, and that’s when I realized I couldn’t let my guard slip. After adjusting my meds, I’m now taking my temperature and tracking my diet more carefully—this illness needs careful care. (P8)
Discussion
This research employed the HAPA framework to explore the risk perception, self-management challenges, and coping strategies among HSCT patients. In line with the HAPA model, both risk perception and action self-efficacy were found to play pivotal roles in shaping behavioral intentions31,32. The volitional phase revealed substantial barriers to action planning and coping implementation, particularly in the areas of symptom management and lifestyle modification. Sustaining self-management behaviors was further hindered by challenges related to symptom control, lifestyle adjustment, psychological adaptation, and financial burden.
Stage characteristics of risk perception and self-management behavior in HSCT patients
According to the HAPA model, health behavior change begins with a motivational phase, during which risk perception and action self-efficacy jointly contribute to the formation of behavioral intentions 33 . In this study, post-discharge HSCT patients demonstrated a dynamic pattern of risk perception, characterized by an initial decline followed by a gradual increase over time.
During the perioperative period, patients exhibited both heightened risk perception and strong behavioral intentions. This phenomenon may be explained by their acute awareness of life-threatening health conditions, a strong desire to survive, and a high level of trust in medical care. These factors appeared to facilitate their transition into the volitional phase, during which they actively formulated specific action plans, such as strict adherence to treatment protocols and proactive engagement in acquiring self-management skills.
In the early post-discharge period, risk perception and self-management behaviors showed a noticeable decline. Patients frequently exhibited inconsistent or poorly structured self-management plans and behaviors. Notably, individuals facing financial hardship often delayed or avoided follow-up visits, despite recognizing their clinical significance. This phenomenon can be attributed to two factors. On one hand, patients transitioning from hospital to home may develop a false sense of security, believing that the most critical stage of recovery has passed. This optimism bias may result in overconfidence in their recovery trajectory and an underestimation of potential risks, such as GVHD. On the other hand, the shift from a highly structured hospital environment to the comparatively unmonitored home setting introduces multiple barriers to effective self-management. These include physical fatigue, insufficient health-related information, and financial strain 34 . Such contextual challenges substantially impair patients’ capacity for daily self-care, leading to reduced adherence to recommended self-management practices. Similarly, Yu et al. 35 also reported a decline in self-management adherence during the early recovery phase following hospital discharge in HSCT patients.
When complications such as GVHD arise, patients’ risk perception typically increases, and self-management behaviors strengthen. Several studies have shown that the early post-discharge period following HSCT is often characterized by a high incidence of complications, including acute GVHD and infections5,6,35. However, insufficient self-management during this phase may hinder patients’ ability to effectively monitor and respond to their condition. Participants reported that access to medical resources and family support enables more effective disease coping and self-management. This finding aligns with research on self-management in ischemic stroke patients, which suggests that individuals who overestimate the risk of recurrence tend to experience greater fear of disease progression and exhibit better health behaviors at 1-month post-discharge. In contrast, those who underestimate the risk often demonstrate poorer health behaviors 36 . Furthermore, qualitative data reveal that although psychological distress can temporarily hinder self-management execution in GVHD patients, active coping strategies are key to facilitating recovery and maintaining long-term adherence to self-care practices 37 . During recovery, HSCT patients report an increased risk perception compared with the lower levels observed immediately post-discharge. However, this heightened perception remains lower than during the peri-transplant period and stabilizes at a moderate level. This suggests that HSCT patients may enter an adaptive phase of “living with the disease.”
Self-management strategies for HSCT patients based on the HAPA model
Based on this study, self-management interventions for HSCT patients should leverage the heightened risk perception and self-efficacy observed during the peri-transplant period to support the shift from risk awareness to concrete health behaviors. To this end, healthcare professionals can implement patient-centered discharge education programs38,39 that emphasize the message: “discharge does not equate to recovery.” Such programs should incorporate patient narratives, visual aids, and other educational tools to clearly communicate the risks of post-discharge complications, such as GVHD, and underscore the potentially serious consequences of dietary non-adherence 40 .
Priority should be given to supporting patients with limited perception and poor self-management behaviors during the early stages post-discharge rehabilitation. Proactive follow-up care can facilitate continuous communication through transitional support mechanisms such as dedicated nurse hotlines, online consultation platforms, and peer support programs, thereby empowering patients in their self-management efforts 41 . Digital interventions should be promoted to help patients maintain self-management efficacy and behaviors 42 . Participants reported that digital goal-setting tools, including mobile applications for symptom monitoring, medication reminders, and features, in supporting daily self-management. However, dietary management remains a significant challenge, particularly due to negative sensory experiences and low acceptance of sterile dietary regimens. These difficulties often conflict with the widespread preference for spicy foods and culturally rooted beliefs in “food as medicine” observed in certain regions 35 . Therefore, we recommend integrating sterile dietary principles with local food cultures to develop modified recipes for HSCT patients.
Complication events may serve as valuable catalysts for enhancing self-management efficacy among HSCT patients. First, when complications arise, patients require adequate support to cope effectively, including family support, peer educational guidance, and medical care as identified herein. Second, complications should be regarded not only as clinical challenges but also as key opportunities for reinforcing health education and facilitating behavioral adaptation. Such events can re-engage patients’ risk awareness and strengthen self-efficacy, thereby promoting more sustainable self-management behaviors. To support this process, wearable devices and mobile health platforms can be leveraged to provide real-time feedback on physiological parameters, allowing patients to make timely and adaptive modifications to their self-management routines 43 . However, differ in their clinical trajectories and psychological responses, which may result in fluctuating levels of risk perception and self-efficacy. Therefore, interventions should be integrated with dynamic assessment to support patients in maintaining optimal levels of risk perception and self-management efficacy throughout the recovery process44,45.
Study limitations
First, the sample was drawn from a single hospital in south-central China, which may limit the generalizability and representativeness of the findings. Regional variations in healthcare policies and access to services may influence self-management behaviors, and as a result, the experiences of patients in other regions may differ. Second, recall bias is a potential limitation, particularly among patients with a longer post-transplant recovery period, who may find it difficult to accurately recall their symptom experiences and self-management behaviors. Third, the relatively short duration of this study may not provide a comprehensive view of how patients’ self-management evolves over time or the challenges they may encounter.
Conclusion
The qualitative study applied the HAPA framework to explore the risk perception, self-management challenges, and coping strategies among HSCT patients. The findings indicate that high risk perception and self-efficacy promote engagement in self-management during the peri-transplant period. However, the volitional phase presents challenges, including symptom management and psychological distress. To support clinical practice, healthcare providers can harness patients’ elevated risk perception and self-efficacy during the peri-transplant period to encourage the adoption of effective self-management behaviors. To address the decline in risk perception and self-efficacy in the early post-discharge phase, tailored interventions and resources should be provided to sustain patients’ motivation and ability to maintain self-management practices.
Footnotes
Acknowledgements
We thank all the HSCT patients for participating and sharing their experiences.
Ethical Considerations
The study was approved by the ethics committee of The Second Xiangya Hospital of Central South University (No. 2024-0275) and was conducted in accordance with the Declaration of Helsinki.
Consent to Participate
Written informed consent was obtained from each participant.
Author Contributions
X.Y. drafted the manuscript. H.Y. and X.Y. contributed to the conception and design of the study. H.Y., Z.X., and X.L. contributed to data acquisition, analysis, and interpretation. H.Y. provided research supervision. X.Y. critically revised the manuscript. All authors have full access to all study data and are responsible for ensuring data integrity and accuracy of the analysis.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Natural Science Foundation of Hunan Province (Grant No. 2024JJ9227), Joint Funding Project of Hunan Provincial Natural Science Foundation and Hunan Xiangya Boai Rehabilitation Hospital Co Ltd. (Grant No. 2025JJ90296) and Science Popularization Foundation of Hunan Province (Grant No. 2023ZK4105).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated or analyzed during this study are included in this published article.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
There are no human subjects in this article and informed consent is not applicable.
Clinical Trial Number
Not applicable.