
Abstract
The aim of this article is to identify whether bioactive glass (BG) is a valid substitute for autogenic bone grafting in maxillofacial reconstruction. PubMed, Scopus, Web of Science, and Cochrane Library databases were searched. Meta-analyses with fixed- and random-effects models were performed by using standardized mean differences (SMDs) with 95% confidence intervals (CIs). Heterogeneity was assessed by using the I² statistic. The significance of results was evaluated at P < 0.05. The BG leads to greater total bone volume retention 6 months after surgery compared with autografts (SMD = 0.796, 95% CI = 0.445–1.147, P = 8.74 × 10⁻⁶, I² = 0%). The resorption rate of BG grafts (SMD = −0.768, 95% CI = −1.360 to −0.176, P = 0.011, I² = 3.82%) was less common, while the retention of the biomaterial (SMD = 1.165, 95% CI = 0.540–1.790, P = 0.00026, I² = 0%) was higher in the experimental group. Both BG and autogenic grafts result in the formation of new bone to a similar extent. However, BG is able to provide long-term stability by maintaining the graft volume, reducing resorption, and preserving the graft scaffold, representing an effective alternative to autogenous bone grafting for a durable maxillofacial reconstruction.
Keywords
Introduction
Maxillofacial surgery faces substantial hurdles during reconstruction efforts which demand biomaterials capable of returning functional and aesthetic outcomes after traumatic injuries or congenital and pathological conditions 1 . Through meta-analysis this comparative evaluation investigates the performance of these materials across multiple outcome measures in maxillofacial reconstruction2,3.
Autogenic bone grafts derived from the patient’s own body represent the highest standard for maxillofacial reconstruction because they possess osteogenic, osteoconductive, and osteoinductive properties combined in a unique way 4 . The grafts maintain active osteoblasts that directly produce new bone while possessing essential growth factors that initiate mesenchymal cell differentiation into osteoprogenitor cells 5 . The natural scaffold structure of autografts facilitates bone cell migration and attachment, thereby creating an optimal environment for osseointegration 6 . The iliac crest, mandibular ramus, symphysis, and calvarial bone are the primary donor sites because each location provides unique benefits related to volume, accessibility, and cortical-to-cancellous ratio for various reconstructive applications 7 . Autografts provide biological benefits but face multiple limitations which involve donor site morbidity and extended operation duration along with restricted availability and variable resorption rates that pose risks to long-term success 2 .
Larry L. Hench created Bioactive glass (BG) to overcome host rejection of inert metal and plastic graft materials and this substance bonds to hard and soft tissues while precipitating hydroxyapatite in water solutions which transforms medical and dental tissue regeneration practices8,9. BG, particularly Bioglass® 45S5 and its derivatives, has been extensively studied for use in oral and maxillofacial surgery because of its superior osteogenic potential compared with calcium phosphate-based materials 10 . Commercial formulations, such as Biogran®, PerioGlas®, and NovaBone® are widely used for maxillofacial defect repair, with NovaBone® forming a putty when mixed with blood for site filling 9 . Larger defects, including mandibular advancement and orbital floor fractures, are treated with BonAlive® (S53P4), whereas StronBone®, an SrO-containing BAG, reduces bone resorption 11 . Mixing granular BAG with autogenous bone significantly enhances bone healing while minimizing donor-site morbidity 12 .
BG promotes bone regeneration by releasing biologically active ions such as silicon, calcium, sodium, and phosphorus upon dissolution in physiological environments, thereby creating an osteogenic microenvironment that stimulates osteoprogenitor and osteoblast proliferation and differentiation13,14. BG enhances bone formation by upregulating osteogenic genes like RUNX2 and OSTERIX, promoting alkaline phosphatase activity, and increasing collagen synthesis, all of which are essential for osteoblast maturation 15 . Additionally, BG influences the molecular pathway of Mitogen-Activated Protein Kinase, further accelerating cellular growth and differentiation 16 . A key feature of BG is its ability to form a hydroxyapatite-rich layer at the tissue interface, facilitating integration with the host bone, and serving as a scaffold for new tissue growth 17 . Importantly, BG particle size plays a crucial role in its bioactivity as smaller particles (<150 µm) dissolve rapidly, boosting ion release and bone formation but resorb quickly, while larger particles dissolve slower, offering longer-lasting structural support, thereby making optimal particle sizing essential for balancing regenerative efficacy and graft longevity9,18.
Despite the growing clinical adoption of BG in maxillofacial reconstruction, comprehensive, evidence-based comparisons with autogenic bone grafts remain limited. While autografts are valued for their inherent osteogenic properties, their drawbacks necessitate the exploration of alternative biomaterials, such as BG, which offers bioactivity, antimicrobial benefits, and enhanced bone regeneration. To date, no comprehensive clinical meta-analysis has specifically evaluated the efficacy of BG for maxillofacial reconstruction. This study aimed to systematically assess the efficacy of BAG against autogenic bone grafts through a meta-analysis, evaluating key outcomes, such as bone regeneration, osseointegration, complication rates, and overall clinical success. By elucidating the comparative advantages and limitations of both materials, this study seeks to provide critical insights for optimizing biomaterial selection in maxillofacial surgery, ultimately advancing patient care and surgical outcomes.
Methodology
The study followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines 19 for conducting systematic reviews and meta-analyses. Compliance with the principles of the Declaration of Helsinki strengthened the ethical foundation of this review. The study was registered on the International Platform of Registered Systematic Review and Meta-analysis Protocols (INPLASY) under registration number 202540089.
Search strategy
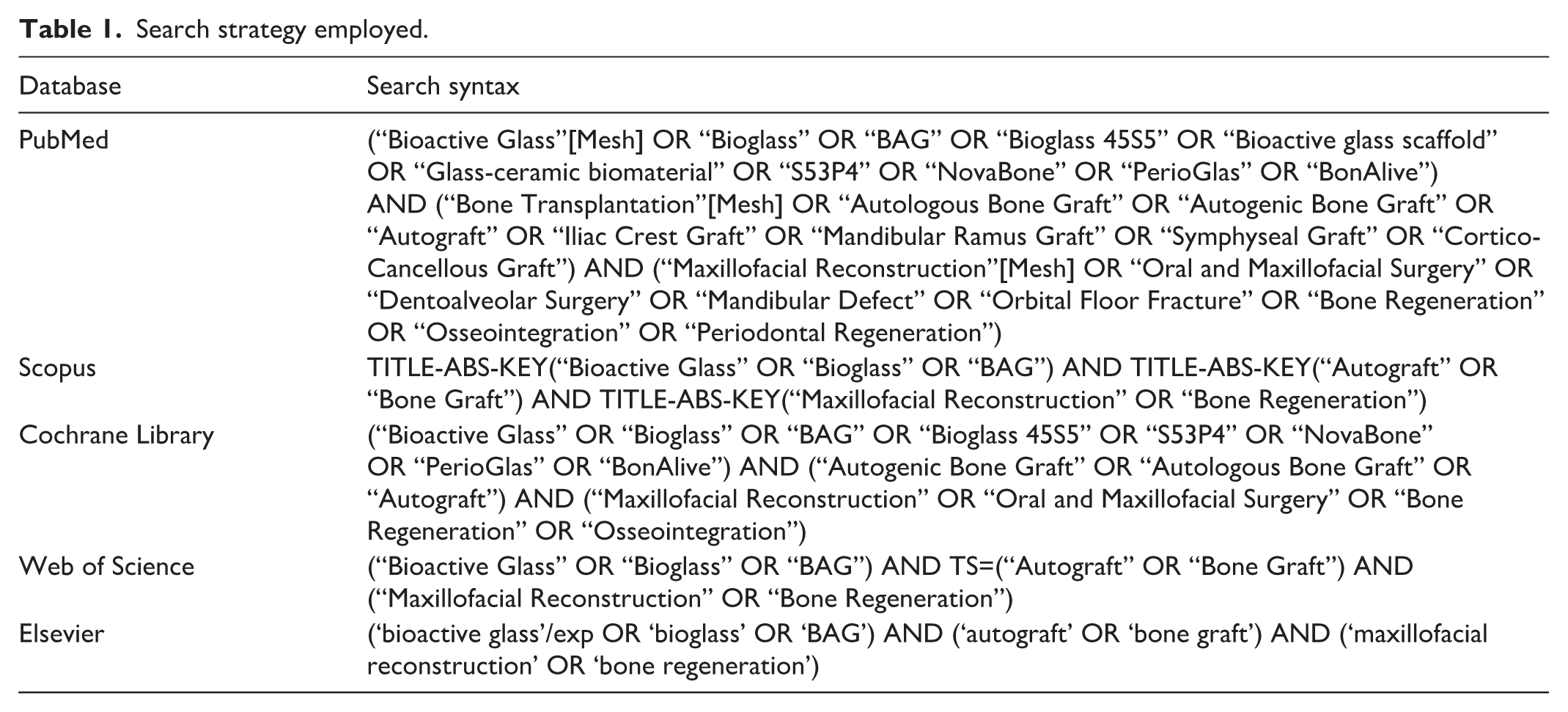
Two authors developed a search strategy based on specified criteria. The team performed independent comprehensive searches of PubMed, Cochrane Library, Scopus, Web of Science, and Elsevier databases to identify studies published until March 2025. A third author reached a consensus decision to resolve any discrepancies. This review targeted randomized controlled trials (RCTs) and cohort studies that investigated BG application. Table 1 presents a description of the search strategy used to identify the articles.
Search strategy employed.
Study selection
Study selection was performed using the PICOS (Participants, Intervention, Comparisons, Outcomes, and Study Design) framework to define inclusion and exclusion criteria. The inclusion criteria encompassed studies that met the following PICO elements: (P) Population: Patients undergoing maxillofacial reconstruction procedures requiring bone augmentation; (I) Intervention: Use of BG as a bone graft substitute in maxillofacial reconstruction; (C) Comparison: Autogenic bone graft or other conventional grafting materials; (O) Outcome: Total bone volume measurement and overall bone healing efficacy, with follow-up assessments at predefined intervals (e.g. 3, 6, or 12 months). Eligible studies included randomized controlled trials (RCTs), cohort studies, and case-control studies published in peer-reviewed journals. Only studies using BG in particulate or granular form were included, as other forms such as 3D scaffolds or injectable pastes were either not reported or not consistently represented across eligible studies. This restriction was applied to maintain consistency and reduce heterogeneity in the pooled analysis.
Studies that did not align with the PICO framework were excluded. Specifically, studies were excluded if they involved (P) populations with systemic conditions affecting bone healing (e.g. osteoporosis, uncontrolled diabetes) or animal models; (I) interventions utilizing composite grafts in which BG was mixed with other materials, making it difficult to isolate its effect; (C) comparisons lacking a standard grafting material or historical controls without direct comparators; and (O) outcomes that did not assess the total bone volume or lacked quantitative bone healing assessments. In addition, studies with insufficient data, abstracts without full-text availability, and non-English publications were excluded.
The study selection process was conducted in two stages. Study selection began with title and abstract screening before moving to a full-text review. Two reviewers independently evaluated the studies for inclusion and resolved any differences by discussing them together or consulting with a third reviewer. The strict selection procedure enabled researchers to gather top-notch evidence to evaluate the effectiveness of BG in maxillofacial reconstruction. The research excluded animal studies, in vitro research, case reports, and narrative reviews because of their lack of methodological clarity. The analysis included RCTs, cohort studies, and comparative interventional studies to ensure a robust evaluation of BG performance in maxillofacial reconstruction.
Data collection and quality evaluation
Two reviewers independently performed data collection and quality evaluation using EndNote 20.2.1 to screen study titles and abstracts according to the inclusion criteria. A blinded third author made the final decision to resolve any disagreements during the full-text review of the potentially eligible studies. Studies without explicit reports on both BG and efficacy of maxillofacial reconstruction often lead to disagreements. Data extraction was performed using a pre-tested Microsoft Excel spreadsheet to maintain consistency while recording essential study information, including authorship details, publication year, study design characteristics, diagnostic criteria, sample group sizes, intervention strategies, and outcome measurements.
Documentation of methodological rigor and potential biases occurred to maintain the systematic data collection and analysis procedures. The Cochrane Risk of Bias 2 (RoB2) tool served as the assessment method for RCTs while the Cochrane Risk of Bias in Non-randomized Studies–of Interventions (ROBINS-I) tool evaluated observational or cohort studies20,21. The Risk-of-Bias Visualization tool (Robvis) based in Bristol, AC, UK, displays results using traffic light plots and summary bar charts 22 . The research team applied rigorous inclusion criteria, together with consistent data extraction and sensitivity analyses, to reduce potential biases.
To further ensure the reliability of the findings, the overall certainty of the evidence was assessed using the Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) framework 23 . The GRADE approach was applied to evaluate confidence in the effect estimates, considering factors such as risk of bias, inconsistency, indirectness, imprecision, and publication bias. The quality of evidence was categorized as high, moderate, or low to present the key outcomes.
Statistical analysis
Statistical analysis was conducted using Comprehensive Meta-Analysis software version 3.7, and the meta-analysis was carried out using a detailed method for the synthesis of data in the form of serious studies. Fixed-effects models were applied for outcomes with non-significant heterogeneity (I² < 25%), accounting for variability across populations and methodologies, whereas random-effects models were used when heterogeneity was high (I² > 75%). The standardized mean difference (SMD) and event rate with 95% confidence interval (CI) were used to pool individual study results, and heterogeneity was assessed using the I² statistic, with P values < 0.05, indicating significant heterogeneity. A Z-test determined the statistical significance of the pooled outcomes, with P < 0.05 considered significant. In addition, the inclusion of more recent studies with improved methodological consistency allows for a more robust quantitative synthesis. In forest plots, different symbols represent key statistical elements. Individual study effect sizes were represented by squares, with the size of each square proportional to the weight assigned to the study in the meta-analysis. The horizontal lines extending from the squares indicate the corresponding CIs. The pooled effect size is depicted as a diamond, with its center representing the overall effect estimate and its width indicating the 95% CI. A narrower diamond reflects higher precision in the pooled estimate, whereas a wider diamond indicates greater variability across the studies.
Data from studies evaluating remission rates, response rates, and symptom improvement outcomes for autogenic grafts and BG were included. Outcomes of BG versus autogenic graft use were assessed for publication bias using Begg’s and Egger’s tests, depicted through the generation of funnel plots for visual inspection of potential publication bias.
Results
Study characteristics
Fig. 1 shows the PRISMA flow diagram, which illustrates the study selection procedure for our systematic review. A total of 7494 records were initially identified through searches across five databases: The initial search across five databases generated records from PubMed (n = 47), Scopus (n = 1534), Cochrane Library (n = 4), Web of Science (n = 142), and Elsevier (n = 5767). Prior to screening, 5726 records were removed, comprising 3551 duplicate records and 2175 records deemed ineligible by the automation tools. This resulted in 1768 records available for screening. Following the screening process, no records were excluded, and all 1768 reports were retrieved. None of these reports were unavailable, allowing for a full eligibility assessment. During this stage, 1753 records were excluded based on predefined criteria: studies not related to digital twin applications in lean supply chain management (n = 1535), non-peer-reviewed literature (n = 215), and studies with unclear methodology or insufficient data (n = 3). Ultimately, 1524–38 studies were included in the systematic review after qualitative synthesis. The characteristics of the included studies are shown in Table 1, and no studies were excluded due to overlapping population reporting. The final selection process ensured a comprehensive and high-quality evidence base for evaluating the role of digital twins in optimizing lean supply chains. Following rigorous evaluation of the study design, risk of bias, heterogeneity, and methodological consistency, 10 of these 15 studies met the inclusion criteria for the meta-analysis. The exclusion of five studies from the meta-analysis was based on a high risk of bias, lack of quantitative data for effect estimation, or substantial methodological heterogeneity. The final selection process ensured the robustness and reliability of the synthesized evidence, providing a comprehensive understanding of the efficacy of interventions for scar reduction.

PRISMA flowchart.
The collective evidence from these 15 clinical studies, as described in Table 2, underscores the growing interest in bioactive materials, particularly BG, as viable alternatives or adjuncts to traditional graft materials across diverse dental and maxillofacial applications. The studies encompassed a wide range of designs, including randomized controlled trials, prospective clinical trials, split-mouth and pilot studies, and comparative analyses, with sample sizes ranging from three to 62 participants. Populations varied from pediatric patients requiring restorative dental procedures to adults requiring bone augmentation for implant placement or orbital floor reconstruction. Most interventions involve the use of BG, either alone or in combination with autogenous bone grafts. These combinations are primarily employed in sinus floor augmentation, maxillary ridge reconstruction, and bone defect repair. Across studies, BG was evaluated for its impact on parameters such as new bone formation, bone resorption rates, histological and immunohistochemical changes, implant integration, marginal bone loss, and postoperative complications. The follow-up duration ranged from 3 to 52 months. Key findings have consistently highlighted the safety, biocompatibility, and efficacy of BG. It demonstrated comparable or superior performance to hydroxyapatite, β-tricalcium phosphate (β-TCP), and autogenous bone, particularly when used at a 1:1 ratio with autografts. While some studies, such as that by Yilmaz et al., noted limitations in alveolar bone preservation using BG cones alone, most reported favorable outcomes in terms of osteoconduction and graft integration. Overall, these studies support the use of BG in both restorative and regenerative contexts, emphasizing its potential to reduce reliance on autogenous grafts and enhance clinical outcomes in dental and craniofacial reconstructive procedures.
Characteristics of the included studies.

Risk of bias
Randomized studies
The analysis of bias risk in the included randomized controlled trials (RCTs) shown in Fig. 2 demonstrates a moderate risk level throughout the studies. Deepika et al. 24 and Stavropoulos et al. 34 found minimal bias risk throughout all evaluation domains which demonstrated appropriate handling of the randomization process together with intervention adherence, outcome measurement procedures, and selective reporting practices. However, Han et al., 26 , Menezes et al., 29 and Pereira et al. 31 exhibit some concerns, leading to a moderate risk of bias. Han et al. 26 showed some concerns in the randomization process (D1), which might indicate insufficient details on allocation concealment or an imbalanced distribution of participants. Menezes et al. 29 and Pereira et al. 31 had concerns related to missing outcome data (D3) and measurement of the outcome (D4). This suggests potential issues, such as incomplete follow-up, lack of intention-to-treat analysis, and subjectivity in outcome assessment. Overall, while most studies had a relatively low risk of bias, limitations in the randomization process, missing data, and outcome measurements in some trials may have impacted the reliability of the findings, necessitating cautious interpretation in meta-analyses.

Traffic light plots on the risk of bias assessment on included RCTs.
Non-randomized studies
Fig. 3 illustrates the variability in methodological quality for non-randomized studies in the risk of bias assessment, where certain studies showed a high risk of bias and others presented moderate concerns. Additionally, Galindo-Moreno et al., 25 Sándor et al., 33 Turunen et al., 37 and Yilmaz et al. 38 study had a serious risk of bias, predominantly due to confounding bias (D1) and participant selection bias (D2). These problems point to insufficient management of baseline characteristics, together with improper matching and retrospective study designs that amplify the risk of bias. Sándor et al. 33 showed serious bias because of deviations from the planned interventions, which suggests possible inconsistencies in how treatments were given or followed. Several studies including those by Kinnunen et al., 27 , and Menezes et al. 28 , and Pereira et al. 32 and Tadjoedin et al. demonstrated a moderate risk of bias in the selection of participants (D2), along with missing data issues (D5) and outcome measurement problems (D6). Potential selection bias exists along with issues with incomplete follow-up and assessments that were not blinded. Although non-randomized studies can demonstrate a low risk of bias in specific domains, their findings must be interpreted.
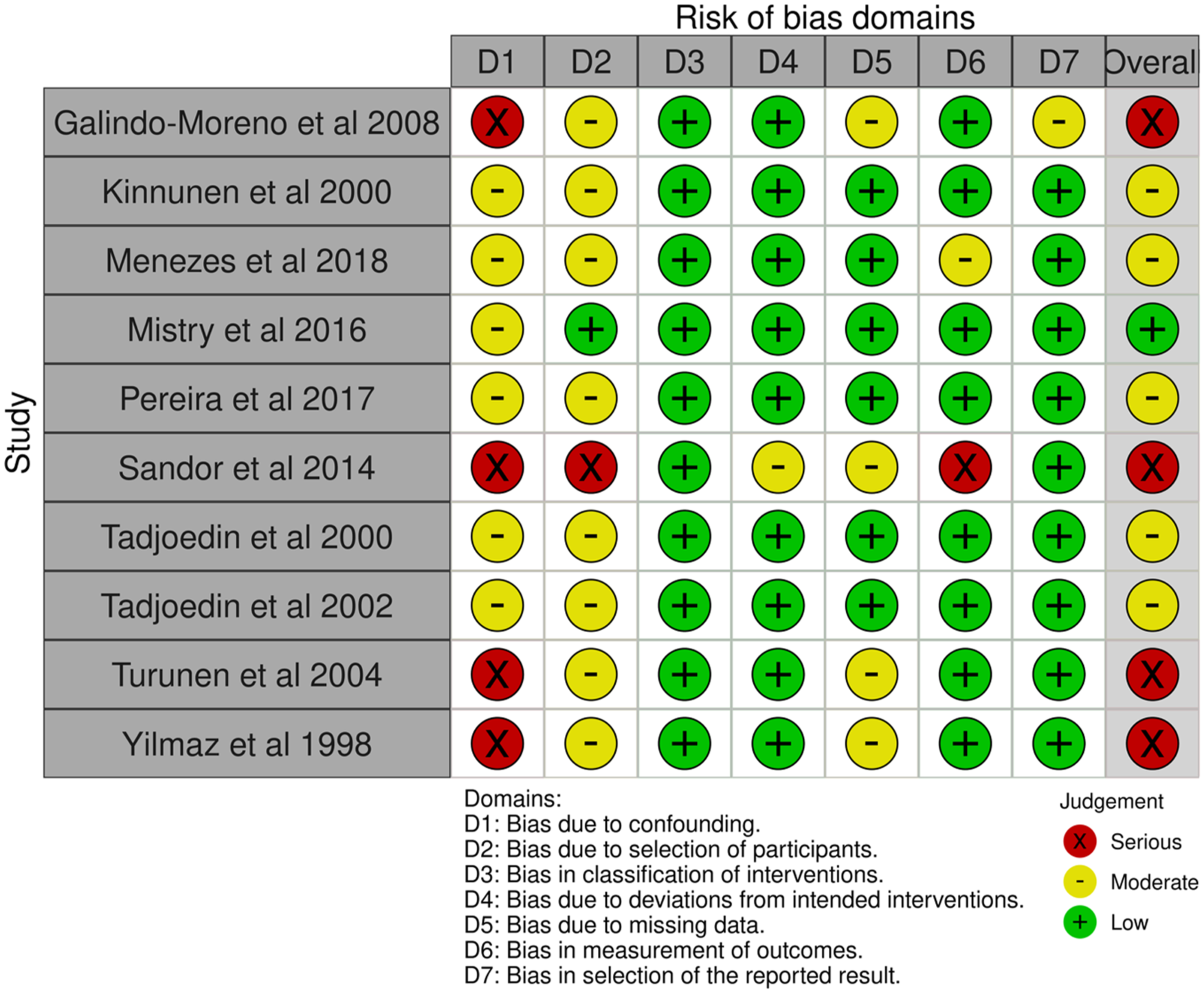
Traffic light plots of the risk of bias assessment for the included non-randomized control studies.
Quality assessment of studies
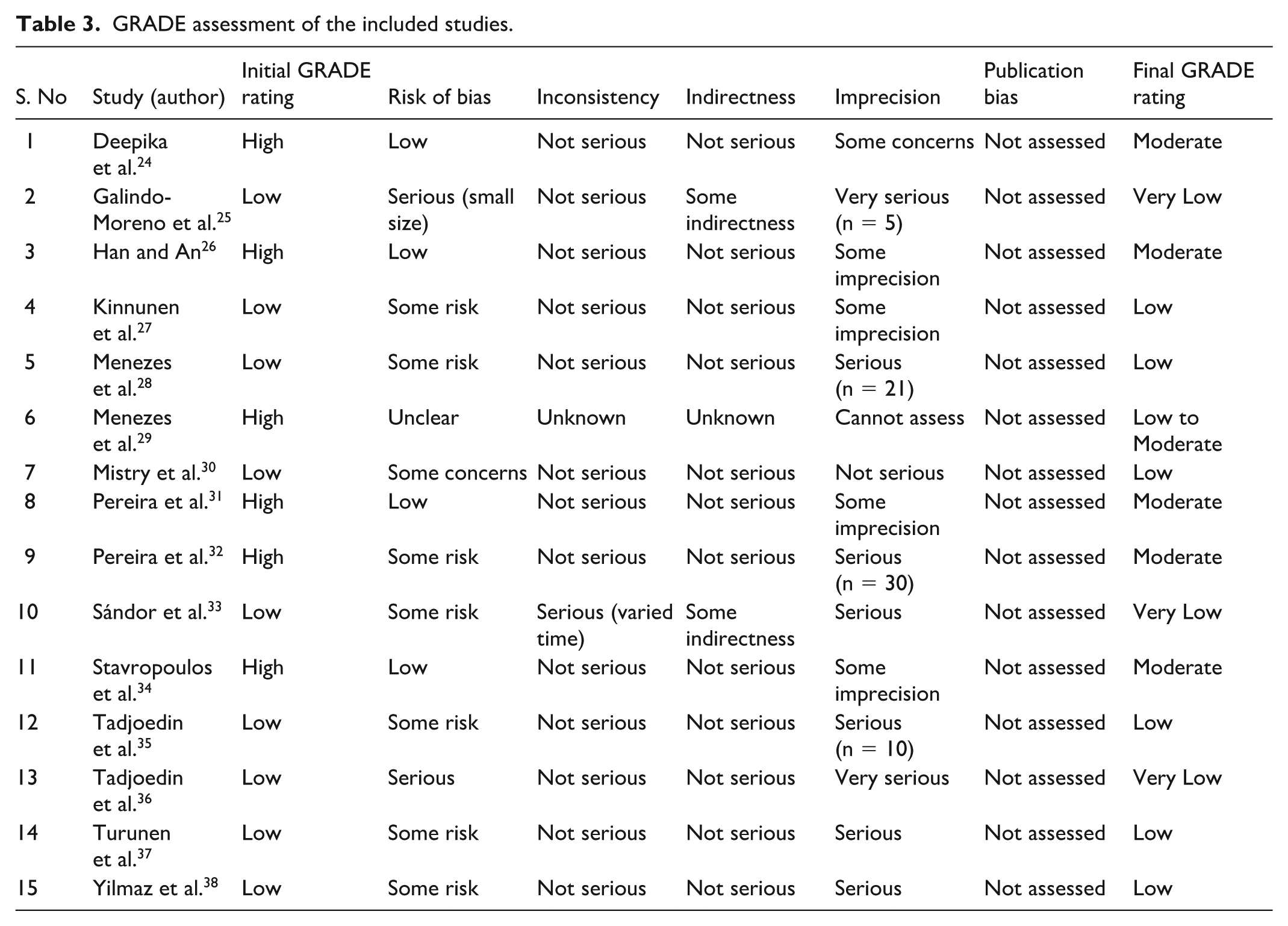
The GRADE approach was employed to assess the quality of evidence across the included studies (Table 3). Among the 15 studies assessed, the risk of bias varied, with some studies demonstrating serious concerns owing to small sample sizes or methodological limitations. Inconsistency was generally not a major concern, except in one study in which varied follow-up times contributed to heterogeneity. Indirectness was noted in two studies due to differences in patient populations or interventions. Imprecision is a common issue, with multiple studies showing concerns owing to small sample sizes or wide CIs. Publication bias was not formally assessed because of the limited number of studies.
GRADE assessment of the included studies.
After thorough scrutiny of the methodological quality and risk factors associated with each study, only 10 studies met the inclusion criteria for the meta-analysis. The excluded studies had significant limitations, including a serious risk of bias, imprecision, or methodological inconsistencies, which could have compromised the robustness of the pooled estimates. The final selection ensured higher quality evidence synthesis, thereby enhancing the reliability of the meta-analysis findings.
Total bone volume
The forest plot in Fig. 4 evaluates the total bone volume at 6 months post-procedure, comparing BG with autogenic bone grafts. The SMD was 0.796 (95% CI = 0.445–1.147), indicating that BG results in moderately higher bone volume retention than autogenic grafts. The statistically significant P value (8.74 × 10⁻⁶) confirms a strong association, and I² = 0% suggests no detectable heterogeneity among the studies, reinforcing the reliability of findings.
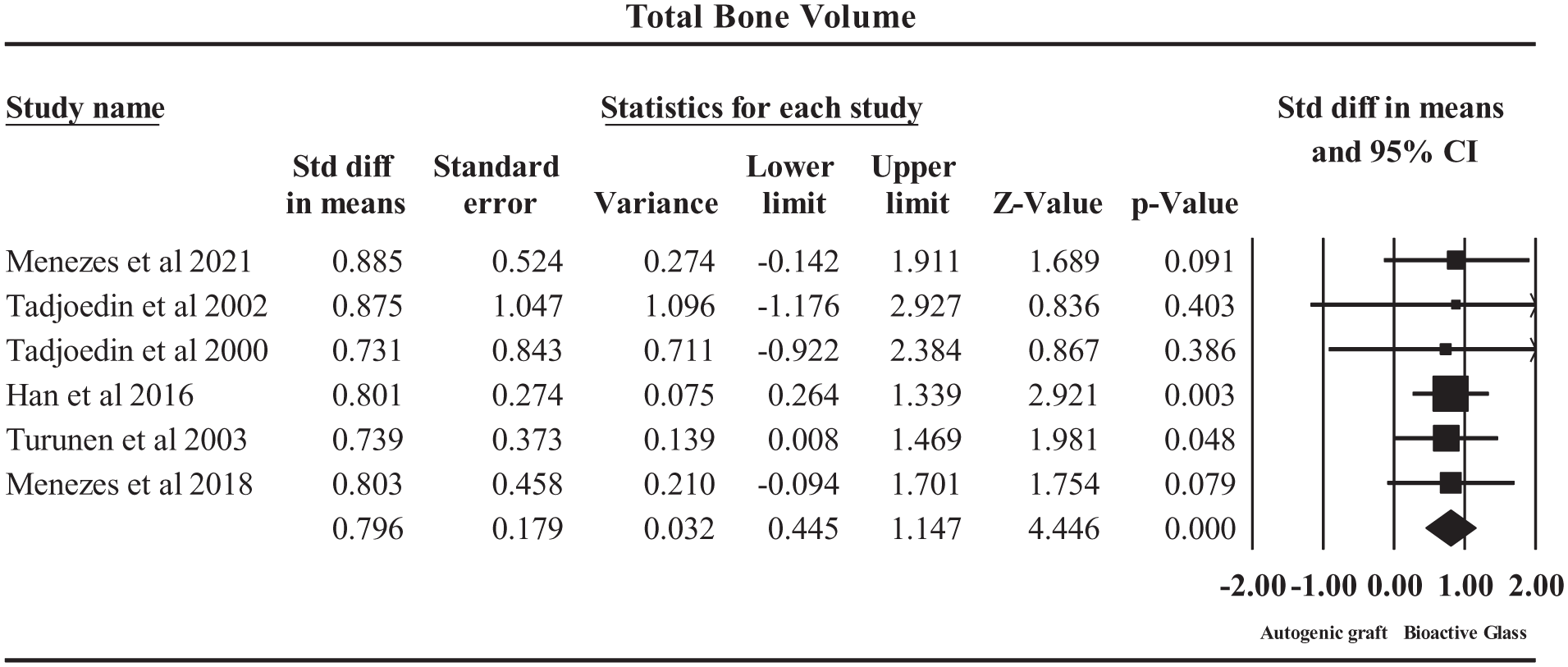
Forrest plot on the outcome total bone volume.
Among the included studies, the Han et al. 26 (SMD = 0.80, P = 0.003) significantly contributed to the effect size, supporting the superior performance of BG. Turunen et al. 37 (SMD = 0.74, P = 0.047) and Menezes et al. 28 (SMD = 0.80, P = 0.079) also demonstrated a positive trend, reinforcing the overall conclusion. However, Tadjoedin et al.35,36 reported lower and less significant effect sizes, indicating some variability in the outcomes across studies.
New bone formation
This meta-analysis, as depicted in the forest plot in Fig. 5, evaluated new bone formation following maxillofacial reconstruction using BG versus autogenic bone grafts. The SMD was −0.304 (95% CI = −0.805 to 0.197, P = 0.235) under both fixed- and random-effects models. This suggests that there is no significant difference in new bone formation between BG and autogenic grafts. Heterogeneity was zero (I² = 0%), indicating consistency across the studies.

Forest plot on the outcome new bone formation post interventions.
Among the studies included, Pereira et al. 32 (SMD = −0.40, P = 0.38), and Pereira et al. 31 (SMD = −0.30, P = 0.55) contributed to moderate negative effect sizes, suggesting slightly lower new bone formation in BG grafts than in autogenic bone. Menezes et al. 28 (SMD = −0.25, P = 0.58), and Stavropoulos et al. 34 (SMD = −0.21, P = 0.81) reported even smaller differences, further supporting the lack of a significant effect.
These findings indicate that BG and autogenic grafts result in comparable new bone formation in maxillofacial reconstruction. While autogenic grafts have inherent osteogenic capacity, they also pose challenges, such as donor-site morbidity and resorption. On the contrary, BG acts as an osteoconductive scaffold, promoting bone regeneration through cell adhesion and mineralization.
From a clinical perspective, the results support the use of BG as a viable alternative to autogenic bone grafts, especially in cases where autograft harvesting is not feasible or carries a high risk. Given the non-significant difference in new bone formation, the choice of material may depend on factors such as graft stability, ease of application, and patient-specific considerations. Further long-term studies assessing functional outcomes, bone density, and integration could help refine clinical decision making.
Resorption rate
The forest plot in Fig. 6 assesses the resorption rate at follow-up in maxillofacial reconstruction by comparing BG with autogenic bone grafts. The SMD was −0.768 (95% CI = −1.360 to −0.176, P = 0.011) in the fixed-effects model, indicating a significantly lower resorption rate for BG than for autogenic grafts. The random-effects model (SMD = −0.772, P = 0.013) yielded a similar conclusion, reinforcing the robustness of the results. Heterogeneity was low (I² = 3.82%), suggesting that the study variations did not significantly impact the overall effect.

Forest plot on the outcome resorption rate post interventions.
Among the included studies, the study by Menezes et al. 29 had SMD of −1.37 (P = 0.014). Tadjoedin et al. 35 (SMD = −1.50, P = 0.105) strongly contributed to the observed effect, both showing higher resorption in autogenic grafts. Menezes et al. 28 (SMD = −0.42, P = 0.348) and Tadjoedin et al. 36 (SMD = −0.08, P = 0.924) reported smaller effects, suggesting some variability in the resorption rates across studies. These findings highlight the superior long-term stability of BG over autogenic bone grafts. Autogenic grafts, which are the gold standard owing to their osteogenic potential, are susceptible to significant resorption over time, leading to volume loss and structural instability. In contrast, BG, an osteoconductive material, provides a stable scaffold that resists resorption, thereby preserving the graft volume and improving long-term outcomes. Clinically, the results support the consideration of BG as a viable alternative, especially in cases where long-term bone volume maintenance is critical. This is particularly beneficial for patients with large defects or compromised bone healing, where the risk of graft resorption is high. Future studies should explore longer follow-up periods and functional outcomes, such as mechanical stability and patient-reported satisfaction, to validate these findings further.
Biomaterials remaining in maxillofacial reconstruction
The forest plot in Fig. 7 evaluates the outcome of the biomaterial remaining in maxillofacial reconstruction by comparing BG and autogenic bone grafts. The SMD was 1.165 (95% CI = 0.540–1.790), indicating that BG demonstrates a significantly higher retention of biomaterial post-procedure than autogenic grafts. The P value (0.00026) confirmed statistical significance, while heterogeneity (I² = 0%) suggested consistency across the studies.

Forrest plot on the outcome remaining biomaterial.
Among the contributing studies, Galindo-Moreno et al. 25 reported the highest effect size (SMD = 1.24), suggesting greater biomaterial retention at BG-treated sites. Conversely, Pereira et al.31,32 reported slightly lower effect sizes (SMD = 1.14), yet reinforced the trend favoring BG.
Higher biomaterial retention suggests that BG maintains longer structural integrity, potentially aiding bone regeneration by providing prolonged scaffolding for osteointegration. In contrast, autogenic grafts, despite their osteoinductive properties, undergo greater resorption over time, which may require additional grafting procedures. This could reduce surgical morbidity and improve long-term outcomes, particularly in cases of complex maxillofacial defects.
Overall, the findings suggest that BG is a viable alternative to autogenic grafts, particularly in patients in whom autograft availability is limited or donor-site morbidity is a concern. However, further clinical trials with long-term follow-up are needed to assess functional integration and patient-reported outcomes.
Publication bias
The evaluation of publication bias for four outcomes presented in Fig. 8 included Begg and Mazumdar’s rank correlation test alongside Egger’s regression test. Begg’s test results showed no significant publication bias for Total Bone Volume (Kendall’s tau b = 0.13333, P = 0.35356) and the remaining biomaterial (Kendall’s tau b = 0.66667, P = 0.14813) based on the correlation between the treatment effect and standard error. The remaining outcomes demonstrated nonsignificant results, which suggests minimal bias from small studies reporting exaggerated treatment effects. Begg’s test power limitations require careful interpretation of the findings, especially in studies with a small sample size.

Funnel plots on the publication bias. (a) Funnel plot on the outcome bone formation, (b) funnel plot on the outcome resorption rate, (c) funnel plot on the outcome biomaterial remaining in the bone, (d) funnel plot on the outcome of total bone volume.
Egger’s test demonstrated no significant small-study effects while evaluating funnel plot asymmetry through regression analysis. For total bone volume, the intercept (B0) was 0.05413 (95% CI: the statistical P value of 0.34687 indicated that there was no significant evidence of funnel plot asymmetry). The intercepts and their respective P values for the remaining biomaterial and additional outcomes showed no evidence of publication bias. The findings of the meta-analysis remained reliable, because the results of both tests were consistent. Corrective procedures using Duval and Tweedie’s trim-and-fill method were implemented when funnel plots displayed potential signs of publication bias. The method calculates the number of missing studies that might create asymmetry and modifies the effect size to produce a more conservative estimate. The stability of the pooled estimates, even after adjustment, confirms the reliability of the findings and indicates little influence of publication bias on the overall conclusions.
Discussion
Recent reviews highlight the broad clinical applications of BG in dental and craniofacial surgery, including its use in ridge augmentation, sinus floor elevation, and reconstruction of craniofacial bone defects, owing to its excellent osteoconductive and osteostimulative properties12,39,40. Long-term clinical studies confirm the favorable integration and safety profile of BG formulations, such as S53P4, in craniofacial reconstructions, with minimal complications and versatility in various forms 41 . This meta-analysis comprehensively evaluated four critical outcomes: total bone volume, new bone formation, resorption rate, and biomaterial remining-following maxillofacial reconstruction using BG compared with autogenic bone grafts. These findings suggest that BG offers significant clinical advantages in several clinical domains.
Clinically, this meta-analysis highlights the potential of BG as a strong alternative to autogenic bone grafts in maxillofacial reconstruction. Bioactive glass demonstrated significantly greater total bone volume retention at 6 months post-procedure, suggesting that it can better preserve the graft structure over time. This is especially important in maintaining contour and stability during facial reconstruction, thereby reducing the need for secondary interventions. Although new bone formation did not differ significantly between BG and autografts, the comparable performance reinforces the utility of BG in promoting effective osteointegration, particularly in patients with contraindications or impractical harvesting autografts. Bioactive glass’ osteoconductive properties of BG offer a predictable regenerative response without donor-site morbidity. Importantly, the significantly lower resorption rate observed with BG implies an improved long-term graft stability. This is clinically relevant in large or load-bearing defects, where volume maintenance is essential for function and esthetics. Similarly, the higher retention of biomaterials in BG-treated sites suggests that it provides prolonged scaffold support, facilitating gradual and stable bone regeneration over time.
Nkenke et al. 42 comprehensively reviewed clinical outcomes of sinus floor augmentation using various techniques and graft materials. Both simultaneous and staged implant placements were assessed, and no significant differences were observed in implant survival. Healing times varied, yet did not affect implant success. Implant survival rates consistently exceeded 90%, regardless of the graft material or membrane use. Complications such as sinus membrane perforation, sinusitis, and graft loss occurred, but were not linked to specific materials. Donor-site morbidity was noted, particularly with iliac crest harvests. Similarly, our meta-analysis demonstrated high implant survival with BG and autografts, with negligible differences in bone volume outcomes at 6 months. These findings collectively support the clinical viability of various graft materials and techniques for sinus augmentation, reinforcing flexible surgical planning based on patient-specific factors.
Regarding new bone formation, the meta-analysis revealed comparable efficacy between BG and autogenic grafts (SMD = −0.304, 95% CI = −0.805 to 0.197, P = 0.235). This nonsignificant difference suggests that despite lacking the intrinsic osteogenic properties of autografts, BG achieves similar outcomes through its osteoconductive properties. Jones 43 corroborated this finding in a systematic review concluding that BG creates an environment conducive to bone formation that ultimately parallels autograft performance. However, these results contradict those of Sculean et al. 44 , who reported superior bone formation with autografts in periodontal applications, highlighting potential variations based on the anatomical site and surgical technique. The consistent findings across studies in the meta-analysis (I² = 0%) strengthen confidence in BG as a viable alternative when considering new bone formation as an outcome measure.
Resorption rate analysis revealed one of the most significant advantages of BG, with substantially lower resorption compared with autogenic grafts (SMD = −0.768, 95% CI = −1.360 to −0.176, P = 0.011). Menezes et al. 29 provided strong evidence for this conclusion (SMD = −1.37, P = 0.014), which is consistent with the findings of Lindfors and Aho 45 , who documented minimal resorption of BG implants over time. The predictable dissolution pattern of BG, as opposed to the more variable resorption of autografts, contributes to its dimensional stability in reconstructive applications. Peltola et al. 11 further validated this advantage, demonstrating that BG undergoes controlled dissolution rather than unpredictable resorption, leading to more reliable outcomes in maxillofacial reconstruction. This stability is particularly valuable in cases that require long-term structural integrity.
Assessment of the remaining biomaterial provided additional evidence favoring BG, with significantly higher retention post-procedure (SMD = 1.165, 95% CI = 0.540–1.790, P = 0.00026). Galindo-Moreno et al. 25 reported the strongest effect (SMD = 1.24), aligning with observations by Tadjoedin et al. 46 that BG particles incorporate into bone matrix while maintaining structural presence. Turunen et al. 37 further explained this phenomenon by noting the prolonged persistence of BG particles serving as scaffolds for new bone growth. This extended presence may enhance the material’s efficacy in challenging reconstruction scenarios by providing sustained support during the regeneration process. The integration of BG into the surrounding tissues, rather than complete resorption, represents a fundamental difference from autogenic grafts, which may contribute to its clinical advantages in certain applications.
Collectively, these outcomes suggest BG as a compelling alternative to autogenic grafts in maxillofacial reconstruction, particularly in scenarios where donor-site morbidity or long-term dimensional stability is critical. Kokubo et al. 47 reached similar conclusions in their comprehensive review, identifying BG as a viable replacement for autografts across various maxillofacial applications. The comparable new bone formation, coupled with superior volume maintenance and reduced resorption, suggests that BG may offer an optimal balance between regenerative capacity and structural integrity.
This research offers significant insights into BG performance against traditional bone grafts for maxillofacial reconstruction while recognizing several limitations that need to be considered. The small sample size used in this study restricts the applicability of the results to wider and more varied patient groups. The strength of the research findings could be improved by future studies involving larger patient groups and trials conducted across multiple centers. The duration of follow-up used in this study was probably too short to properly evaluate the long-term results, including graft stability and integration over multiple years. Extended monitoring periods through longitudinal studies would yield better insights into the long-term effectiveness of BG. Third, patient-specific variables, such as differences in bone metabolism, underlying health conditions, and surgical techniques, could have influenced the outcomes, necessitating more controlled and standardized methodologies in future research. Fourth, while the study primarily focused on clinical efficacy, biomechanical and histological analyses are necessary to further validate the biological integration of BG at a microscopic level. Finally, the included studies varied in surgical indications (e.g. sinus augmentation, orbital reconstruction), types of BG (e.g. 45S5, S53P4, Biogran), and follow-up durations (ranging from 3 to 52 months). While these differences were documented in the data extraction phase and summarized in the characteristics table, subgroup analysis was not feasible because of insufficient sample size within each subgroup. Future research should incorporate advanced imaging and molecular techniques to provide deeper insights into the cellular interactions. Finally, cost-effectiveness and accessibility are key considerations. Bioactive glass, while promising, may be more expensive or less readily available in certain regions than traditional grafting materials. Future studies should assess the economic viability and real-world applicability of BG in various healthcare settings. Addressing these limitations through further research could strengthen the evidence base and facilitate broader clinical adoption of BG in maxillofacial reconstruction.
Conclusion
These findings indicate that BG offers superior long-term stability, as demonstrated by a significantly lower resorption rate and greater biomaterial retention than those of autogenic grafts. In addition, BG exhibits moderately higher bone volume retention at 6 months post-procedure, reinforcing its role in maintaining structural integrity. Although autogenic grafts possess inherent osteogenic properties, BG effectively supports bone regeneration through osteoconduction. Clinically, these results support the use of BG as a viable grafting material, particularly in cases where autograft harvesting is impractical or is associated with high donor-site morbidity. Enhanced graft stability and reduced resorption rates of BG may be particularly beneficial for patients with large defects or compromised healing capacity. However, further long-term studies are warranted to assess mechanical stability, functional integration, and patient-reported outcomes to further refine its clinical application.
Footnotes
Acknowledgements
All the authors are thankful to the King Khalid University, Saudi Arabia for the financial support.
Author contributions
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors extend their appreciation to the Deanship of Research and Graduate Studies at King Khalid University for funding this work through Large Research Project under grant number RGP2/545/46.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and materials
Data supporting the findings of this study are available from the corresponding author upon reasonable request.
Statement of human and animal rights
This article does not contain any studies with human or animal subjects.
Informed consent statement
Not applicable.