
Abstract
Despite recent developments in the treatments for ischemic stroke, such as tissue plasminogen activator (t-PA) and thrombectomy, effective therapies for intracerebral hemorrhage (ICH) remain scarce. Stem cell therapies have attracted considerable attention owing to their potential neuro-regenerative ability; preclinical and clinical studies have been conducted to explore strategies for achieving functional recovery following ICH. In this review, we summarize the findings of preclinical studies on stem cell therapies of ICH, with a focus on different animal models, stem cell sources, transplantation methods, and their potential mechanisms of action. We also provide an overview of data from clinical trials to discuss the current status and future perspectives. Understanding the effectiveness and limitations of stem cell therapy and the future prospects could expand the applications of this novel therapeutic approach for ICH.
Introduction
Stroke, which suddenly occurs when blood vessels clog (ischemic stroke) or burst (hemorrhagic stroke), subsequently causing considerable brain damage, is the second most common cause of deaths globally and the most common cause of disability 1 . While ischemic stroke accounts for the largest portion of stroke (75%) compared with hemorrhagic stroke (10%), the fatality and disability rates are considerably higher with hemorrhagic stroke 2 . Although tissue plasminogen activator (t-PA) and thrombectomy have substantially improved the prognosis of ischemic stroke 3 , there is a lack of effective treatment for hemorrhagic stroke, especially intracerebral hemorrhage (ICH). Even with the advances in medical technology, the rate of ICH-related mortality has not decreased over the past decades4,5. While hematoma evacuation is often applied in the treatment of acute ICH, the precise role of surgery in improving the mortality rate and post-stroke mobility remains unclear. The International Surgical Trials in Intracerebral Hemorrhage, STICH and STICH II, were the two largest randomized trials performed to elucidate the efficacy of surgical interventions for ICH; however, the outcomes of these trials could not demonstrate any significant advantages of surgery for supratentorial hematoma6,7. Based on the data from these trials, the American Heart Association and the American Stroke Association recommend supratentorial hematoma evacuation as a “life-saving” treatment in patients with severe ICH 8 , suggesting that surgical therapies may reduce mortality but not contribute to the amelioration of neurological sequelae. Patients with ICH often undergo rehabilitation for neurological recovery following acute phase and recover within the initial months and soon reach plateau 9 . Owing to the lack of other effective treatments, especially following subacute phase, ICH has led to approximately 64.5 million disability-adjusted life years 2 , which has resulted in severe socioeconomic problems to both patients and society. Therefore, innovative treatment strategies to minimize or reverse the neurological sequelae are highly warranted.
During recent years, cell-based therapies have attracted attention for the treatment of neurological disorders including ischemic stroke, spinal cord injury, and traumatic brain injury10,11. Previous clinical trials have shown promising results wherein patients receiving cell therapy showed better neurological recovery than the controls12,13. Nevertheless, there is limited basic and clinical research on stem cell therapies for ICH. The reason remains unclear, but presumably, ischemic stroke is often preceded because of the high proportion of patients. Although several review articles have discussed stem cell therapies for ischemic stroke, review articles describing stem cell therapy for ICH are limited.
Therefore, in this review, we summarize the preclinical and clinical data on the efficacy of stem cell therapies for ICH, focusing on the advances in this field and providing insights into future development of therapies for ICH.
Preclinical Studies
We thoroughly reviewed original articles on the efficacy of stem cell implantation in animal models of ICH. A literature search on PubMed (https://www.ncbi.nlm.nih.gov/pubmed) was performed to identify basic research articles on stem cell therapy for ICH. We used the keywords “stem cell” and “hemorrhagic stroke” for the initial search. The search was restricted to articles written in English and to articles on mesenchymal stem cells (MSCs). We included articles from 2006 to 2020. However, articles related to subarachnoid hemorrhage and intraventricular hemorrhage were excluded. Hemorrhage in these diseases occurs outside the brain parenchyma, resulting in different brain damage mechanisms. We further reviewed some articles cited within the papers selected from our preliminary search. Article selection and data collection were performed by one of the authors (S.T.). Finally, we selected 39 studies that aligned with the aims of this review, and they have been listed in Table 1.
Preclinical Studies of Stem Cell Therapy in ICH Models.

ICH: intracerebral hemorrhage; BM: bone marrow; MNC: mononuclear cell; MSC: mesenchymal stem cell; IV: intravenous; NSS: neurological severity score; ND: not described; IA: intra-arterial; ICV: intracerebral ventricle; IC: intracerebral; MLPT: modified limb placing test; AD: adipose derived; MT: mannitol; UC: umbilical cord derived; mNSS: modified neurological severity score; HGF: hepatocyte growth factor; GDNF: glial cell–derived neurotrophic factor; PRP: platelet-rich plasma; IN: intranasal; WJ: Wharton’s Jelly-derived; Hx: hematoma; CM: conditioned medium; ERK: extracellular signal-related kinase; PI3K: phosphatidylinositol-3 kinase; PD: placenta derived.
Based on collected data, the heterogeneity of the experimental methods is illustrated in Fig. 1, which included different animals, methods of hemorrhagic procedure, cell sources, transplantation routes, and transplantation timings. Understanding the different methodologies is important, as the mode of action of stem cells is different among these methods, which may influence the results of the clinical trials.

Charts outlining the parameters used in animal studies on stem cell therapy against ICH. The animal species (A), hemorrhagic methods (B), implanted cell sources (C), implanting routes (D), and implant timings (E) are summarized. ICH: intracerebral hemorrhage.
Animal Models
Thirty-four (87.2%) of the 39 studies used rat models of ICH, 4 used mice, and 1 used monkeys (Macaca fascicularis) (Fig. 1A). Male animals were used as the ICH model in 31 studies, whereas females were used in 5 studies. While the age of animals was not accurately described in most studies, based on their body weights, most animals could be adjudged as young. Suda et al. 36 described the efficacy of bone marrow mononuclear cells (BM-MNCs) in elderly rats but did not specify the precise age. Cell therapy guidelines for stroke recommend the use of animals of both sexes and different ages to match the situation envisioned for clinical use53,54.
Basal ganglia were the most frequently used targets of ICH although some articles also described striatum or caudate nucleus as the targets. Bacterial collagenase injection was the most commonly (29/39 studies; 74.4%) used method for the induction of ICH, followed by whole blood injection (9/39 studies; 23.1%) and hemoglobin injection (1 study; 2.6%) (Fig. 1B). The bacterial collagenases used for ICH models were subdivided into types IV, VII, I, and animal origin free A (AFA); of these, collagenase types IV (0.1–1 U titer) and VII (0.075–0.5 U titer) were used most frequently. In general, for any given type of collagenase, the higher the titer, the larger the hematoma produced. Mello et al. 51 showed that administering 0.1 U of collagenase IV led to the development of moderate ICH, whereas 0.25 U caused severe ICH in animal models. In addition, type VII collagenase is considered stronger than type IV collagenase. An autologous blood-induced ICH model has also been reported, in which 50–100 µl of blood was injected into rats and 1.5 ml into monkeys. Although both collagenase and autologous blood models are frequently used in preclinical experiments, it is difficult to accurately mimic ICH in humans using these models. In the collagenase model, ICH is caused by the bleeding of cerebral vessels disrupted by collagenase, and it mimics the pathophysiology of human ICH. However, collagenase also disrupts other circumambient structures, and as such, the tissue damage can be greater than that in human ICH. In addition, it is difficult to control the hematoma volume in the collagenase model because the cerebral vessels are unselectively injured. Meanwhile, in the autologous blood model, the hematoma size is relatively easy to control, facilitating the generation of more uniform models. However, in human physiological conditions, hematoma is caused by the external environment as opposed to originating in cerebral arteries. Furthermore, autologous blood may, at times, contain added anticoagulants. Irrespective of the added anticoagulants, the coagulation cascade is activated before further injections. These conditions do not accurately reflect the pathophysiology of human ICH. Moreover, unlike its pathogenesis in humans, ICH is not associated with hypertension in animal models. We found only two studies that used spontaneously hypertensive rats for generating the ICH model to mimic human conditions. Thus, reproducing the exact pathophysiology of human ICH seems extremely difficult.
Stem Cell Sources
Of the 39 studies reviewed, 22 (56.4%) used xenogenic, 16 (41.0%) used allogeneic, and 1 study used autologous stem cells. Among the studies on xenogenic stem cells, 11 did not use immunosuppressants, and it was unknown whether they were adopted in the remaining studies. Furthermore, there was no mention of the utilization of immunosuppressants in 15 of the 16 studies involving allogeneic stem cells. Nevertheless, 10 xenogenic cell studies and 12 allogeneic cell studies reported that the implanted cells differentiated into neural cells around the injured brain. This may be attributed to the low immunogenicity of the MSCs 55 .
Bone marrow (BM)-derived MSCs (BM-MSC) were the most frequently used source of stem cells (24/39 studies; 61.5%), followed by birth-associated tissue [such as umbilical cord (UC), placenta, Warton jerry, and amnion membrane]-derived MSCs (10/39 studies; 25.6%), and adipose tissue–derived MSCs (AD-MSCs) (Fig. 1C). While BM-MSCs and AD-MSCs obtained from patients can be used as autologous grafts, allograft is also frequently examined. Birth-associated tissue-derived MSCs can be obtained from healthy volunteers non-invasively, and these cells show greater cell proliferation and lower immunogenicity than the adult tissue-derived MSCs56–58. Further comprehensive examination is required to elucidate the most appropriate source of cells for the treatment of ICH.
Transplantation Routes, Dosages, and Timings
Intravenous (19/39 studies; 48.7%) and intracerebral routes (17/39 studies; 43.6%) are the most commonly used routes of transplantation, followed by intracerebral ventricle (5/39 studies; 12.8%), intra-arterial (2/39 studies; 5.1%), and intranasal (one study; 2.6%) routes (Fig. 1D). Studies on the comparison of cell transplantation routes are seldom reported. Zhang et al. 15 reported intravenous, intra-arterial, and intracerebral ventricle cell transplantations in the acute phase after hemorrhagic insult. They transplanted the same amount of cells (2 × 106 BM-MSCs) four times (days 1, 3, 5, and 7) through different routes. The results showed that intracerebral ventricle transplantation achieved the best functional recovery, followed by intra-arterial transplantation, whereas the recovery in the intravenous transplantation group was identical to that in the sham-treated group. The authors also found that the transplanted cells were engrafted in the ipsilateral brain through intracerebral ventricle and intra-arterial methods but not via the intravenous method. The cells were mostly distributed in the ipsilateral cortex, bleeding foci, and hippocampus and showed neuronal or glial transformation. Xie et al. 40 have reported that intracerebral and intravenous transplantations of human umbilical cord–derived stem cells are effective when these are transplanted 1 day after hemorrhage. Although it is not clear which route can achieve the best recovery of the neurological function, Hess and Borlongan 59 have proposed that intravenous transplantation may be beneficial in the acute phase of stroke owing to its immunomodulatory effect, whereas intracerebral transplantation is favorable in the chronic phase wherein inflammation is mostly settled.
The dose of implanted cells administered varies depending on the route of implantation; the median doses of the cells were 2.5 (0.5–8) million for the intravenous, 0.5 (0.1–5) million for intracerebral, 0.5 (0.2–2) million for intracerebral ventricular, 1.5 (1–2) million for intra-arterial, and 1 million for the intranasal routes. Especially, the cell doses administered through the intravenous and intracerebral routes were significantly different (P < 0.01, Wilcoxon rank-sum test), and this difference may be associated with the difficulty in the migration of intravenously implanted cells into the injured brain lesions. Thus, it is important to adjust the dose of cells administered depending on the route of implantation to ensure functional improvement. In three of the six studies that included a group with unfavorable functional outcomes15,19,23,32,48,51, the cell doses administered were less than the median value mentioned above.
The cells were administrated within 1 day after ICH onset in most of the studies (25 of the 39 studies; 64.1%) (Fig. 1E). Although the dose of cells administered influences the speed of functional recovery, the timing proved even more important; the sooner the cells were administrated after the onset of ICH, the faster was the improvement in the functional outcomes. There was a weak correlation between the time of implantation and the time required for functional recovery (ρ = 0.64, Spearman’s rank correlation coefficient).
Factors Enhancing the Effect of Stem Cell Therapy
Previous studies have shown that combination therapy involving stem cell implantation or stem cell modifications, such as gene transduction, with preconditioning may be more efficacious than stem cell therapy alone in the treatment of ICH.
Seyfried et al. 19 have reported the beneficial effects of mannitol injection followed by intra-arterial infusion of MSCs. Compared to treatment with MSCs alone, the combination therapy with MSCs and mannitol led to an increased number of newly generated neuronal cells around the lesion and better functional recovery. This finding may be attributed to the ability of mannitol to increase vascular endothelial permeability by opening the blood–brain barrier (BBB). Furthermore, Zhang et al. 39 have shown the efficacy of hematoma aspiration before the intracerebral administration of MSCs. Hematoma aspiration along with MSC administration leads to a reduced expression of p53, which promotes apoptosis, and consequently leads to better outcomes than MSC treatment alone. Vaquero et al. 32 demonstrated that treatment using MSCs with a platelet-rich plasma-derived scaffold, containing platelet-derived trophic factors that enhance endogenous neurogenesis, may have better long-term outcomes than the treatment with MSC alone.
Regarding gene transduction, hepatocyte growth factor (HGF) 21 , glial cell line–derived neurotrophic factor (GDNF)26,47, and microRNA-126a-3p (miR-126) have also been reported 52 . While HGF-transduced MSCs improve the neurological function in ICH by nerve fiber remyelination and axonal regeneration, the GDNF-transduced MSCs improve the neurological recovery by preventing apoptosis, promoting neuronal replacement, and enhancing other neurotrophic factors. Furthermore, miR-126-modified MSCs improved angiogenesis and ameliorated functional outcomes of ICH by repairing the BBB and damaged nerves.
Various studies have reported the efficacy of preconditioned MSCs. For instance, Lee et al. 35 have shown that MSCs primed with fasudil, a Rho-kinase inhibitor, significantly improved the functional outcomes compared with the non-primed MSCs through the upregulation of GDNF. Sun et al. 37 used hypoxia-preconditioned MSCs to enhance neurotrophic factors and neurogenesis, whereas Min et al. 46 used apocynin, a nicotinamide adenine dinucleotide phosphate oxidase inhibitor, for MSC preconditioning. The apocynin-preconditioning enhanced the therapeutic efficacy of the MSCs by enhancing the cerebrovascular integrity and neuroprotective effects. Collectively, these reports suggest that stem cell therapy for hemorrhagic stroke can be improved using appropriate enhancers.
Takamiya et al. 60 recently reported that MSCs compounded with a biodegradable scaffold (CellSaic) resulted in better functional recovery than MSCs alone in a chronic ICH model. CellSaic released higher amounts of trophic factors such as BDNF, HGF, vascular endothelial growth factor (VEGF), and GDNF; extracellular vesicles (exosome) were also released in CellSaic. Takamiya et al. found better cell engraftment with immunohistochemistry and neuronal integrity with animal single-photon emission computed tomography (SPECT). These results indicate that combined cell product can upregulate the function of MSCs.
Mechanisms Underlying Stem Cell Therapy for Hemorrhagic Stroke
Based on previous studies, the mechanisms underlying the effects of stem cell therapy in hemorrhagic stroke can be classified as follows: neurogenesis, angiogenesis, anti-brain edema, anti-inflammation, and neuroprotection (summarized in Table 2).
Potential Therapeutic Mechanisms of Stem Cells in Preclinical ICH Models.
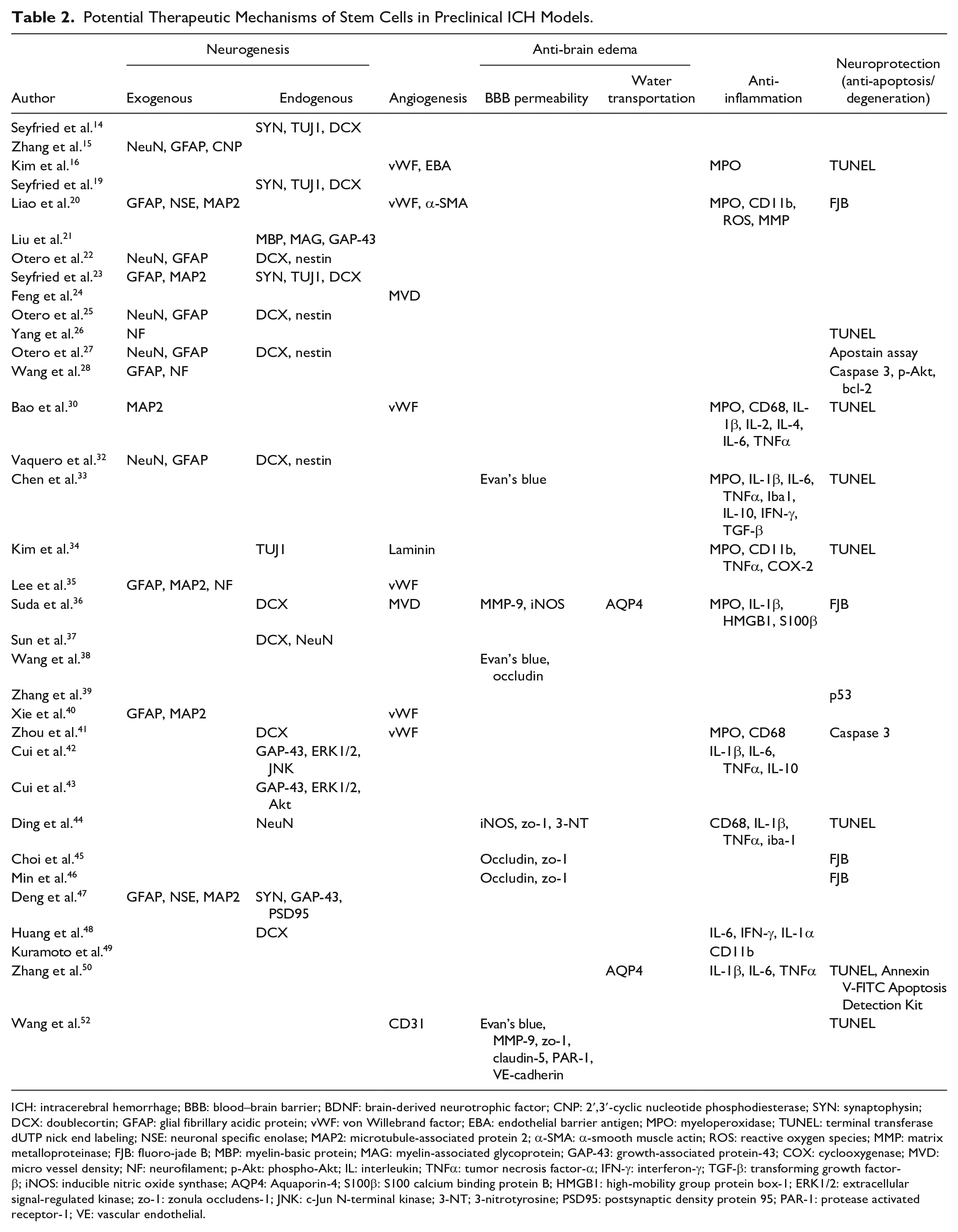
ICH: intracerebral hemorrhage; BBB: blood–brain barrier; BDNF: brain-derived neurotrophic factor; CNP: 2′,3′-cyclic nucleotide phosphodiesterase; SYN: synaptophysin; DCX: doublecortin; GFAP: glial fibrillary acidic protein; vWF: von Willebrand factor; EBA: endothelial barrier antigen; MPO: myeloperoxidase; TUNEL: terminal transferase dUTP nick end labeling; NSE: neuronal specific enolase; MAP2: microtubule-associated protein 2; α-SMA: α-smooth muscle actin; ROS: reactive oxygen species; MMP: matrix metalloproteinase; FJB: fluoro-jade B; MBP: myelin-basic protein; MAG: myelin-associated glycoprotein; GAP-43: growth-associated protein-43; COX: cyclooxygenase; MVD: micro vessel density; NF: neurofilament; p-Akt: phospho-Akt; IL: interleukin; TNFα: tumor necrosis factor-α; IFN-γ: interferon-γ; TGF-β: transforming growth factor-β; iNOS: inducible nitric oxide synthase; AQP4: Aquaporin-4; S100β: S100 calcium binding protein B; HMGB1: high-mobility group protein box-1; ERK1/2: extracellular signal-regulated kinase; zo-1: zonula occludens-1; JNK: c-Jun N-terminal kinase; 3-NT; 3-nitrotyrosine; PSD95: postsynaptic density protein 95; PAR-1: protease activated receptor-1; VE: vascular endothelial.
MSCs May Promote Reorganization of the Neural Circuits
Neurogenesis is the most common mechanism that can be subdivided into exogenous and endogenous neurogenesis. Exogenous neurogenesis is the direct differentiation of the implanted stem cells, whereas endogenous neurogenesis involves the generation of self-neuronal cells produced by the stimulation of the implanted stem cells.
The transplanted cells pre-labeled with various methods, such as using green fluorescence protein (GFP), might be considered to show exogenous neurogenesis when they also present a positive signal for neural marker antibodies such as anti-NeuN, anti-neurofilament, and anti-microtubule-associated protein 2. Although the mechanisms underlying cell migration to injured lesions remain unclear, Xie et al. 40 suggested that the mechanisms might be associated with stromal cell-derived factor-1 (SDF-1)/CXCR4 system. SDF-1 is expressed in reactive astrocytes and attracts MSCs that express CXCR4 in cerebral infarction61–63. In addition, sphingosine-1-phosphate (S1P), which is expressed in injured cellular membrane, has been reported to help multilineage-differentiating stress-enduring cells migrate through the specific receptor (S1PR) 64 . Thus, some factors derived from damaged tissues may influence the effectiveness of stem cell therapy.
However, researchers have argued that endogenous neurogenesis is more prominent than exogenous neurogenesis as the detectable implanted cells are substantially smaller than those initially implanted14,22,23,25,27,32. Growth-associated glycoprotein-43 (GAP-43) is reported to play an important role in neurogenesis21,42,43. GAP-43 is a protein associated with the development and regeneration of neurons and is expressed following the phosphorylation of extracellular signal-regulated kinase 1/2 (ERK1/2). Cui et al. 43 reported that BM-MSC implantation increases phosphorylated ERK1/2 and GAP-43 levels in the perihematomal brain tissue.
Furthermore, Liang et al. 31 suggested that MSCs cause the reconstruction of neural networks. The authors showed that, while the ipsilateral caudal forelimb area (CFA, primary motor area) was not restored by stem cell implantation despite the functional improvements, the ipsilateral rostral frontal area (supplementary motor area) and contralateral CFA were enhanced by the administration of MSCs. These effects may be attributed to the reorganization of the neural circuits.
MSCs Improve Angiogenesis After ICH
Angiogenesis is an important mechanism underlying the effects of stem cell therapy as the brain tissue around the hematoma is usually susceptible to ischemia. Angiogenesis is promoted by certain trophic factors, including VEGF. Zhou et al. 41 showed that MSC implantation increased the number of von Willebrand factor–positive cells and the level of VEGF in the perihematomal area. Furthermore, Wang et al. 52 reported that MSC administration increases CD31 (endothelial marker), and its effect was enhanced when miR-126-modified MSCs were used, presumably because miR-126 regulated the response of endothelial cells to VEGF. Thus, angiogenesis owing to the trophic factor secreted from MSCs will take on the role of neurological recovery after ICH.
MSCs Ameliorate BBB Permeability
The exacerbation of neurological symptoms by perifocal edema after hemorrhagic stroke is known as secondary injury; thus, reduction of cerebral edema is an important strategy to prevent further disease progression. The reports have shown that MSCs decrease the level of inducible nitric oxide synthase, 3-nitrotyrosine (hallmark of ONOO−), and matrix metalloproteinase-9 that may disrupt the BBB33,65,66 and increase the levels of tight junction markers such as zonula occludens-1 and claudin-5. Thus, MSCs ameliorate BBB permeability. In addition, Suda et al. 36 and Zhang et al. 50 have suggested that the anti-brain edema mechanism not only prevents the disruption of BBB but also modulates the expression of aquaporin-4 (AQP-4), a major water channel of the central nervous system associated with the pathogenesis of brain edema. The authors showed that AQP-4 expression is downregulated by MSC administration.
MSCs Reduce Neutrophil Infiltration and Inflammatory Macrophages
Inflammation can lead to secondary injuries in ICH. Therefore, controlling inflammation is essential to prevent neurological deterioration in ICH. Several reports have suggested the following anti-inflammatory mechanisms: decreased levels of pro-inflammatory cytokines including interleukin (IL)-1α, IL-1β, IL-2, IL-4, IL-6, tumor necrotic factor α (TNFα), and interferon γ; increasing levels of anti-inflammatory cytokines such as IL-10; and modulating inflammatory cells including neutrophil, microglia, and macrophage16,20,30,33,34,36,41,42,44,48,49,50,67,68. Chen et al. have suggested that TNFα stimulates gene/protein-6 (TSG-6), an upstream factor of inflammation, and reduces the infiltration of neutrophils and the production of inflammatory macrophages 69 . The authors showed that MSC implantation increased the expression of TSG-6.
MSCs Exert Neuroprotective Effects Related to Anti-Apoptotic Pathways
Approximately half of the preclinical studies suggested that MSCs have some neuroprotective effects, including anti-apoptotic or anti-degenerating functions, based on the results of apoptosis detection assay or Fluoro-Jade staining; some studies have reported detailed pathways. For example, Wang et al. 28 have demonstrated that the expression of phosphorylated Akt and B-cell lymphoma-2 (bcl-2), which are associated with the anti-apoptotic pathway and reduce cytochrome C from mitochondria, is upregulated and the level of caspase 3 is reduced upon MSC implantation. Zhang et al. 50 targeted p38 and Jun N-terminal kinase (JNK), which are also components of an apoptotic pathway, and found that MSCs downregulate phosphorylated p38 and JNK expression.
Clinical Trials
The number of clinical trials on the efficacy of stem cell therapy for hemorrhagic stroke is limited, and a summary of the published trials is shown in Table 370–77.
Summary of Clinical Trials Using Stem Cells for Patients With Intracerebral Hemorrhage..
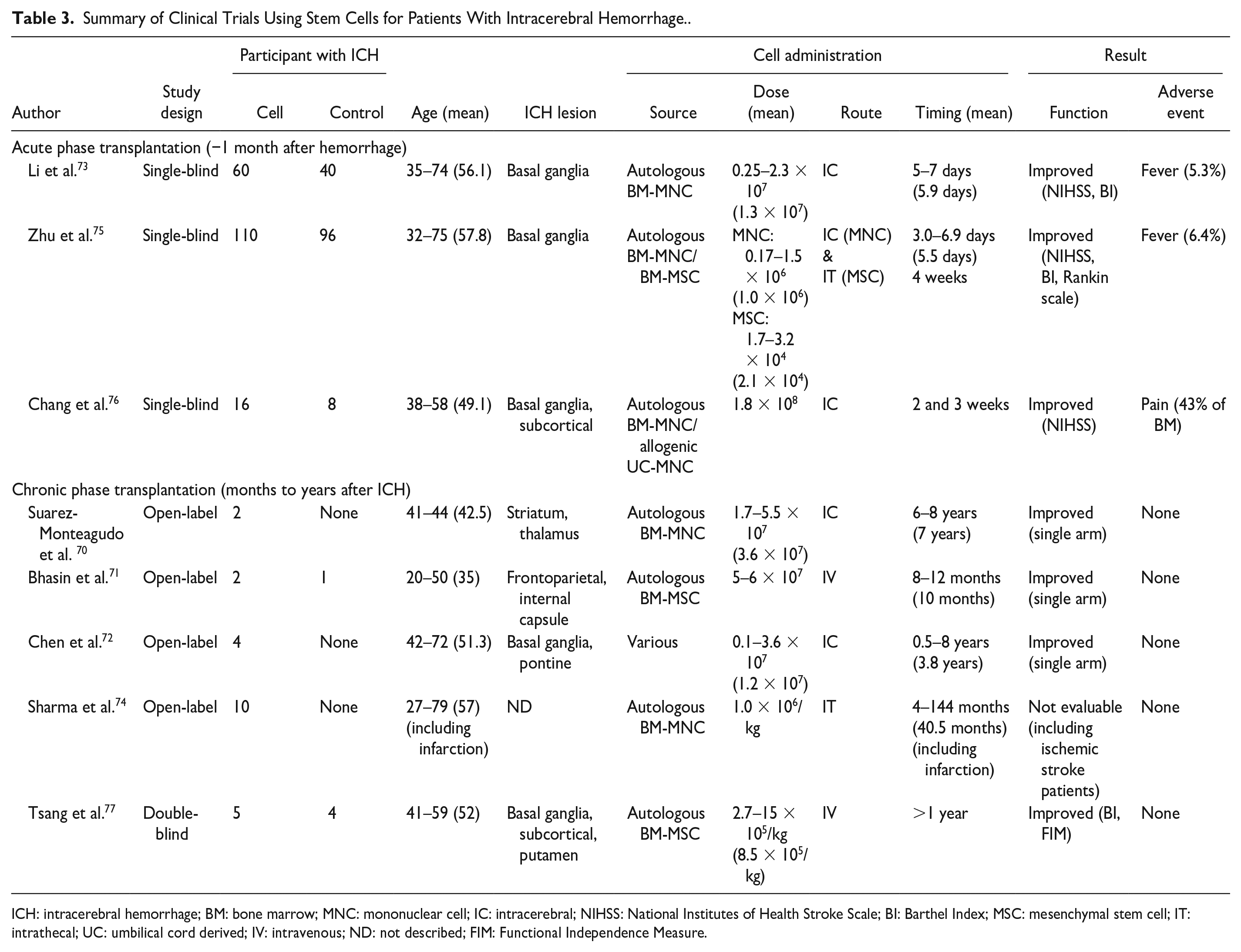
ICH: intracerebral hemorrhage; BM: bone marrow; MNC: mononuclear cell; IC: intracerebral; NIHSS: National Institutes of Health Stroke Scale; BI: Barthel Index; MSC: mesenchymal stem cell; IT: intrathecal; UC: umbilical cord derived; IV: intravenous; ND: not described; FIM: Functional Independence Measure.
Overview of the Trials
In the eight trials, 209 of 358 patients with ICH received MSCs or mononuclear cells (MNCs), which were mostly derived from autologous BM. The mean age of participants in each trial ranged from 35 to 57.8 years, and the integrated mean age of participants in all trials, calculated with the number of participants and individual mean age, was 56.2 (range: 20–79) years. Compared with those in the preclinical studies, participants in clinical trials were considerably old. Meanwhile, almost all hematomas were in the basal ganglia, similar to those observed in basic research.
Safety of Stem Cell Transplantation for Patients With ICH
Safety is a major concern when applying new treatment options. There has been no report of tumorigenesis of the transplanted stem cells in patients with ICH; however, tumorigenesis of human fetal neural stem cells has been reported in patients with ataxia telangiectasia 78 . Therefore, extra caution must be exerted, as it is difficult to remove cells once they are engrafted into the host brain. The transplantation procedure itself is associated with the risk of complications. Intracerebral transplantation is associated with the risk of de novo ICH caused by the injection needle, and the infection may be more frequent, as patients with ICH often experience multiple skin incisions during hematoma evacuation and decompression surgery. Intravenous or arterial transplantation is associated with the risk of thromboembolic complications such as pulmonary embolism and ischemic stroke; systemic delivery of cells can exacerbate the innate immune response, which may induce a fever or graft versus host disease. Intrathecal transplantation can cause hydrocephalus due to cell clogging in the cerebrospinal fluid drainage system. However, there are no reports of serious adverse events associated with cell therapy in patients with ICH. Suárez-Monteagudo et al. 70 reported intracerebral transplantation of autologous BM-MSCs in two patients with chronic striatum and thalamic hemorrhage and encountered no surgical complications, such as infection and bleeding. Furthermore, Li et al. 73 treated 60 patients via intracerebral transplantation and reported no de novo ICH. Bhasin et al. 71 reported one case of intravenous transplantation of autologous bone-derived MSCs for frontoparietal hemorrhage, with no early or late adverse reactions, while Chen et al. 72 adopted intrathecal transplantation for four patients and observed no major complications.
Minor complications occur in 5% to 6% of participants receiving cells through the intracerebral or intrathecal routes, wherein the patients developed a low-grade fever73,75 and complained of iliac crest pain due to BM aspiration of autologous BM-MSCs 76 . Further acquisition of clinical data is necessary to elucidate the safety of cell transplantation in larger clinical trials.
Efficacy of Stem Cell Transplantation in Patients With ICH
During the acute phase, in which MSCs are administered within 1 month of ICH, favorable results have been reported73,75,76. For instance, Li et al. 73 reported that intra-cavity transplantation of autologous BM-MNCs 5 days post hematoma evacuation through intracranial drainage tube resulted in better neurological recovery than that in the control group. The authors also reported the recovery of not only the mobility but also the intellectual impairment, including language and mental activities. Zhu et al. 75 transplanted 6.9–12.8 × 107 (mean: 8.5 × 107) MSCs into both hematoma cavity (5 days post evacuation) and subarachnoid space via intrathecal transplantation (4-week post evacuation). The authors compared 110 patients with MSC transplantation and 96 controls and found significant recovery, based on the National Institutes of Health Stroke Scale (NIHSS), Barthel index, and modified Rankin Scale (mRS), in the transplanted group. The difference continued for up to 12 months post transplantation. Chang et al. 76 reported the findings of a 5-year long-term follow-up in patients with stem cell transplantation. The authors retrospectively investigated patients who received autologous BM-MNCs, allogeneic human umbilical cord blood cells, or control, and transplanted the cells twice (2 and 3 weeks post hemorrhage removal surgery), through the drainage tube inserted into the hemorrhagic cavity. The results showed that although the patients had similar backgrounds, the NIHSS was lower in both transplanted groups than in the control, up to 60 months post transplantation. These results suggest that hematoma evacuation with intracavity stem cell transplantation can accelerate the recovery; notably, none of these trials were double-blinded or randomized.
Conversely, during the chronic phase, it is difficult to discuss the effectiveness of MSCs, as most of the trials were open-label studies that included patients with both ischemic and hemorrhagic stroke, with a small proportion of patients with hemorrhage. However, several studies have shown promising results, including motor functional recovery and its mechanisms. Interestingly, Suárez-Monteagudo et al. 70 reported that one patient who received 1.7 × 107 cells into the perilesional area 6 years after hemorrhage showed functional recovery and increased motor area, as examined via transcranial magnetic stimulation, in the contralateral cortex but not in the ipsilateral area. In contrast, Bhasin et al. reported that the laterality index of blood oxygen level-dependent (BOLD) increased in the ipsilateral premotor cortex 71 . Chen et al. transplanted olfactory ensheathing cells, neural progenitor cells, umbilical cord mesenchymal cells, and Schwann cells through selected routes, including intracranial parenchymal implantation, intrathecal implantation, and intravenous administration. Some patients showed increased Barthel Index 1–2 years post transplantation. There has been only one study in which autologous BM-MSCs were intravenously implanted in patients with chronic ICH in a double-blinded manner and the patients showed improved functional results compared with the control group 77 , although the number of patients was small and detailed data were lacking.
Summary of Clinical Trials and Future Perspective
The number of clinical trials of ICH is considerably less than those on ischemic stroke, which hinders the clinical application of stem cell therapy. Further trials to determine the safety, effectivity, and underlying action mechanisms of stem cell therapy are highly warranted.
In contrast to basic studies, most clinical trials have been focused on functional recovery, hence failed to elucidate the molecular mechanisms of the disease. Understanding the modes of action such as changes in glucose metabolism and binding potential of benzodiazepine receptors could facilitate the discovery of effective treatment methods 79 .
Future clinical trials should focus on the following: (1) clarifying the therapeutic mechanisms underlying stem cell therapy using functional imaging including positron emission tomography (PET) and SPECT; (2) designing a combination therapy to enhance the therapeutic effect of MSCs; and (3) conducting trials to better understand different transplantation procedures for different phases of ICH.
Conclusions
The results from studies using animal models suggest the effectiveness of stem cell therapy for ICH; therefore, preclinical studies should be conducted to apply these findings in a clinical setting. Understanding the data obtained from previous preclinical studies will facilitate future research to address knowledge gaps.
Early clinical studies suggest that stem cell therapy is safe and effective against ICH; however, further studies are warranted for clinical application stem cell therapy.
Footnotes
Author Contributions
S.T. and M.K. designed the study; S.T. selected the articles and collected the data; S.T. and M.K. drafted the original manuscript; M.F. advised on study design and critically revised the manuscript; all authors have read and approved the final manuscript.
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
There are no human subjects in this article and informed consent is not applicable.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by AMED under grant number JP17bk0104045h0003.