
Abstract
The hematopoietic comorbidity risk index (HCT-CI) is a pre-transplant risk assessment tool used to prognosticate morbidity and mortality of patients undergoing allogeneic hematopoietic stem cell transplantation. Recently, the HCT-CI was updated to include an age component (HCT-CI-age). Although other studies have validated this tool in allogeneic stem cell transplant recipients, it has never been studied in an autologous transplant patient population. We retrospectively reviewed 181 patients who underwent their first autologous hematopoietic stem cell transplant. We aimed (1) to assess whether an HCT-CI score of 3 or greater is associated with greater mean transplant hospital days, greater total hospital days, or greater risk of intensive care unit (ICU) utilization and (2) whether age influences any of these responses independent of HCT-CI. There were 136 patients with an HCT-CI score of 3 or higher and 45 with a score less than 3. The length of initial transplant hospitalization in days was not statistically significant (15.6 v 16.4 days, P = 0.38). Utilizing spline modeling prediction curves, transplant hospital days were estimated to increase from a mean of 15.5 days for a patient with 4 comorbidities to a mean of 22.7 days for a patient with 8 comorbidities. Age made no significant impact on any of the outcomes. The HCT-CI, with or without age, in an autologous stem cell transplantation did not predict length of hospitalization or utilization of the ICU. Patients with higher-HCT-CI scores at baseline may incrementally utilize more resources, and this should be explored in a larger cohort population.
Introduction
Hematopoietic stem cell transplantation (HCT) is a frequently utilized treatment option for hematologic malignancies 1 . Although HCT often improves survival for the index disease, it is associated with major toxicities that affect post-transplant morbidity and mortality 2 . Previous research aimed to stratify patients at risk for these unfavorable outcomes, which led to the adoption of the Charlson Comorbidity Index (CCI) for patients undergoing allogeneic HCT 3 . The utility of the CCI has been validated in allogeneic HCT; however, its lack of specificity necessitated a new tool to identify high-risk transplant patients4,5.
In 2005, Sorror and colleagues at the University of Washington developed the HCTcomorbidity risk index (HCT-CI) to overcome the shortcomings of its predecessor 6 . In its landmark trial, patients with scores ≥3 had significantly higher non-relapse mortality and worse overall survival. Several studies have reproduced these findings, while some have not leading to the use of other risk scores7–15. Regardless, experts conclude the HCT-CI is useful, and the Center of International Blood and Marrow Transplant Registry (CIBMTR) mandates its use via the Pre-Transplant Essential Data collection14,16,17. Other risk assessment tools work in conjunction with the HCT-CI giving hematologists even more insight into potential clinical courses for their patients18–20.
Though the original HCT-CI has been incorporated into pre-transplant evaluation for years 6 , the creators of the tool aimed to further stratify patients by amending the HCT-CI to include an age component (HCT-CI-Age) 21 . Their findings concluded that age > 40 has implications for survival, and should be routinely incorporated into patients’ clinical assessments. To date, two studies have validated the HCT-CI-age’s ability to predict overall survival and non-relapse survival in a retrospective allogeneic cohorts, but no literature in the autologous setting exists22,23.
Despite the robust data in favor of the HCT-CI in allogeneic stem cell transplant populations, the benefit in autologous transplant recipients is less clear. Although it has been established that comorbidities impact outcomes in these patients, few studies have validated the use of the HCT-CI in this population. Despite this, the HCT-CI is still used to inform transplant eligibility determinations24–27. Although data exist in allogeneic populations, there is no literature evaluating other clinically meaningful outcomes such as time to engraftment, transfer to intensive care unit (ICU), or resource utilization in autologous HCT patients based on HCT-CI-Age. HCT is costly, and current data outline the association of HCT-CI with resource utilization in an allogeneic group 28 . As healthcare margins continue to narrow, it is imperative to evaluate resource-utilization in the autologous arena.
In this retrospective study, our team aimed to evaluate outcomes of adult patients receiving autologous HCT based on their pre-transplant HCT-CI score, while also assessing if age influences these outcomes. These data could generate hypotheses on whether age should be an added component to the HCT-CI score for adult patients considered for autologous transplant.
Methods
We retrospectively reviewed 181 patients who underwent autologous hematopoietic stem cell transplantation (ASCT) at the University of Kentucky Markey Cancer Center in Lexington, Kentucky between January 1, 2015 and December 31, 2017. The study was approved by the institutional review board.
Patients
All adult patients who received their first autologous hematopoietic stem cell transplant for a malignant indication during the specified time points were included. The electronic health record was utilized to collect demographic and clinical data. Pre-transplant clinical data included patient-specific comorbidities that are included on the original HCT-CI comorbidity index 6 .
Independent Variables
HCT-CI was dichotomized into groups with fewer than three comorbidities and three or more comorbidities. Aims were (1) assess whether an HCT-CI score of 3 or greater is associated with greater mean transplant hospital days, greater total hospital days, or greater risk of ICU utilization, after adjustment for patient age, sex, ethnicity, and indication for treatment (multiple myeloma or lymphoma/other, and CD34+ cell count); and (2) assess whether age influences any of these responses independent of HCT-CI score. For the multivariable modeling, indication for transplant was dichotomized into multiple myeloma and non-multiple myeloma.
Outcomes
Transplant hospital days were defined as number of days from transplant (day stem cells infused) to discharge. Hospital days prior to transplant were not included due to patients having differing conditioning regimens. Total hospital days were defined as number of days in the year post-transplant. ICU utilization was defined as at least 1 day in the ICU in the year post-transplant. Patients were hospitalized until neutrophil engraftment, defined as 3 consecutive days of an absolute neutrophil count >500 x 103/uL.
Statistical Analysis
A descriptive analysis of patient and treatment characteristics was conducted. Continuous measures were compared by t test or Mann-Whitney U test for independent samples. Categorical variables were compared by Pearson’s chi-square test, or by Fisher’s Exact test if any cell count was less than 5. P values and effect sizes were reported for each comparison. Effect size measures were Cohen’s d (Cramer 1992) or Vargha-Delany A for continuous variables (Vargha and Delaney 2000), and Cramer’s V for categorical variables 29 .
For multivariable modeling of the association of HCT-CI group with transplant hospital days and total hospital days, Poisson and negative binomial regression were considered. Overdispersion of the response variable was assessed via likelihood ratio test. For ICU utilization, logistic regression was used, with Firth’s bias adjustment applied due to the small overall sample size and the small number of patients who required ICU services. All multivariable models were adjusted for patient age, sex (with female as referent), ethnicity (with non-white as referent), indication for treatment (with non-multiple myeloma as referent), and CD34+ cell count. Age and CD34+ cell count were treated as continuous variables. They were initially entered into the multivariate models as natural cubic splines, to allow for the possibility of a nonlinear relationship with the outcomes (total hospital days, transplant hospital days, and risk of ICU admission). Spline models were compared via likelihood ratio test with reduced models, in which a simple linear relationship was assumed. If the reduced model (without spline) provided no worse fit than the full model (with spline), then the relationship term was entered into the final model as a normal, linear term.
Continuous HCT-CI Analysis
As a secondary analysis for total hospital days and transplant hospital days, we fit the same models as described, but with HCT-CI treated as a continuous variable, and its relationship with hospital days modeled by a natural cubic spline. All outcomes and covariates were otherwise the same as in the primary models, in which HCT-CI dichotomized at 3. Full regression results for all models are reported in the supplemental materials.
Results
Description of Study Sample
Between January 1, 2015 and December 31, 2017 there were 181 patients who underwent their first ASCT at the University of Kentucky. HCT-CI scores pre-transplant ranged from 0 to 8. There were 136 patients with a score of 3 or higher, and 45 with a score less than 3. The mean HCT-CI score was 3.5, the median was 3 (Fig. 1). Baseline patient and treatment characteristics by HCT-CI group can be found in Table 1. Most patients (93%) were Caucasian, 64% were male, and more than three-quarters were at least 50 years of age. Over half the patients transplanted were being treated for multiple myeloma, while a third were being treated for non-Hodgkin lymphoma. The most common pre-transplant comorbidities were pulmonary dysfunction, diabetes, and psychiatric disturbance. Fourteen patients had a prior history of a different malignancy.

Distribution of HCT-CI scores in the sample. HCT-CI: hematopoietic cell transplantation comorbidity index.
Comparison of Patient and Treatment Characteristics Between HCT-CI Groups.

ASCT: autologous hematopoietic stem cell transplantation; HCT-CI: hematopoietic cell transplantation comorbidity index.
The effect size quantifies the magnitude of the difference between the groups. For continuous measures we used Cohen’s d (small effect: 0.2, moderate effect: 0.5, large effect: 0.8) or Vargha-Delany A (0.5 means no effect). For categorical variables, we used Cramer’s V (for binary independent variables, small effect: 0.1, moderate effect: 0.3, large effect: 0.5; for independent variables with four levels: small effect: 0.06, moderate effect: 0.17, large effect: 0.29).
Non-myeloma = Diffuse large B-cell lymphoma (DLBCL) (n = 24), Mantle cell (n = 11), primary central nervous system lymphoma (PCNSL) (n = 6), Hodgkin lymphoma (n = 18), and other (n = 3).
BEAM = carmustine, etoposide, cytarabine, and melphalan.
R-TBC = rituximab, thiotepa, busulfan, and cyclophosphamide.
Total Hospital Days
Total days in hospital within 1 year of transplant had a large range (11–53 days) that varied considerably based on HCT-CI score (Fig. 2). In univariable analysis, patients with HCT-CI scores ≥3 spent 5% more days in the hospital within 1 year of transplant than patients with HCT-CI scores <3 (mean 17.4 days versus 16.5 days). The difference was not statistically significant (IRR = 1.05; 95% CI = [0.93–1.19], P = 0.41).

Number of days in hospital during the first year post-transplant. HCT-CI: hematopoietic cell transplantation comorbidity index.
In multivariable analysis, there was little change after adjusting for patient age, sex, race, indication, and CD34+ cell quantity (IRR = 1.06, 95% CI = [0.94–1.20], P = 0.33) (Table 2). Only the quantity of CD34+ cells infused was associated with total hospital days. For each increase of 106cells/kginfused, total hospital days decreased by 4.4% (IRR = 0.96, 95% = [0.93–0.98], P = 0.002). There was no evidence that total hospital days varied with age (IRR = 1.00, 95% CI = [0.99–1.01], P = 0.33). Full regression estimates for total hospital days are reported in the supplement (Table S1).
Adjusted Estimates of Association Between HCT-CI and Transplant Hospital Days, Total Hospital Days, and ICU Admission.

HCT-CI: hematopoietic cell transplantation comorbidity index; ICU: intensive care unit.
Adjusted for patient age, sex, race, indication and CD34+ cell count.
95% confidence interval.
Transplant Hospital Days
When considering only the initial transplant hospitalization, patients with HCT-CI scores ≥3 again stayed in the hospital 5% longer than patients with HCT-CI scores < 3 (16.4 days versus 15.6 days) on univariate analysis, This difference was also not statistically significant (IRR = 1.05; 95% CI = [0.94–1.17], P = 0.38).
Similarly, in multivariate analysis, there was little change after adjusting for patient age, sex, race, indication, and CD34+ cell quantity (IRR = 1.05, 95% CI = [0.94–1.16], P = 0.39) (Table 2). The quantity of CD34+ cells infused was associated with transplant hospital days; for each increase of 106 cells/kg infused, length of stay decreased by 3.8% (IRR = 0.96, 95% CI = [0.94–0.99], P < 0.01). Patient age was also associated with transplant hospital days; for each 10-year increase in age, length of stay increased by 5.4% (IRR = 1.05, 95% CI = [1.00–1.01], P = 0.01). Full regression estimates for transplant hospital days are reported in the supplement (Table S2).
ICU Treatment
Of the 181 patients included in the analysis, 13 (7%) spent at least 1 day in the ICU during their transplant hospitalization. In the group with higher comorbidity risk indices, 11 patients out of 136 (8.1%) required an ICU stay, compared to 2 patients out of 45 (4.4%) in the lower comorbidity group. In univariate analysis, a non-statistically significant increase in odds of ICU transfer was detected for patients with HCT-CI ≥3 (odds ratio [OR] = 1.59, 95% CI = [0.48–8.5], P = 0.50). This trend increased in multivariate analysis (OR = 1.89, 95% CI = [0.5–10.1]).
Lymphoma patients were more prevalent in the lower comorbidity group (33% versus 19%), possibly due to being of younger age (mean 53.1 vs. 59.5 years for myeloma patients). Lymphoma patients were also more likely to require ICU care (8 out of 79 patients compared to 5 out of 102 multiple myeloma patients). When this imbalance in the composition of the HCT-CI groups was accounted for in the multivariate analysis, the estimated odds of ICU utilization increased.
The other covariates (age, sex, race, CD34+ cell count) were not significantly associated with odds of ICU utilization. Full regression estimates for transplant hospital days are reported in the supplement (Table CT 20-03)S3).
Treating HCT-CI as continuous variable
To account for the possibility that HCT-CI is associated with the outcomes of interest, but not in the way that is assumed by dichotomizing HCT-CI at 3, we refit the multivariate models with number of comorbidities treated as a continuous variable. HCT-CI was entered into the models as a natural cubic spline. The advantage of this approach is that it makes no assumptions about the nature of the relationship between relationship between HCT-CI and days in hospital. All outcomes and covariates were otherwise the same as in the primary models, in which HCT-CI dichotomized at 3.
Total Hospital Days
There was no significant difference in fit between the full model—with the relationship between HCT-CI and total hospital days modeled by a natural cubic spline with 3 degrees of freedom—and a reduced model in which it was treated as linear a linear term (χ2 = 3.5, df = 2, P = 0.17). In the final model, a statistically significant, linear association between HCT-CI and total hospital days was not indicated (βHCT-CI = 0.026 [-0.003–0.054]). Full regression estimates are reported in the supplement (Table S4).
Transplant Hospital Days
There was a significant difference in fit between the full model—with the relationship between HCT-CI and transplant hospital days modeled by a natural cubic spline with 3 degrees of freedom—and a reduced model in which it was treated as linear (χ2 = 6.6, df = 2, P = 0.037). In the final model, a statistically significant, nonlinear association between HCT-CI and transplant hospital days was found (P < 0.001). Full regression estimates are reported in the supplement (Table S5). The estimated relationship between continuous HCT-CI and transplant hospital days for myeloma and non-myeloma patients is visualized in Fig. 3 and Fig. 4.

Estimated mean transplant hospital days for myeloma patients by HCT-CI score.
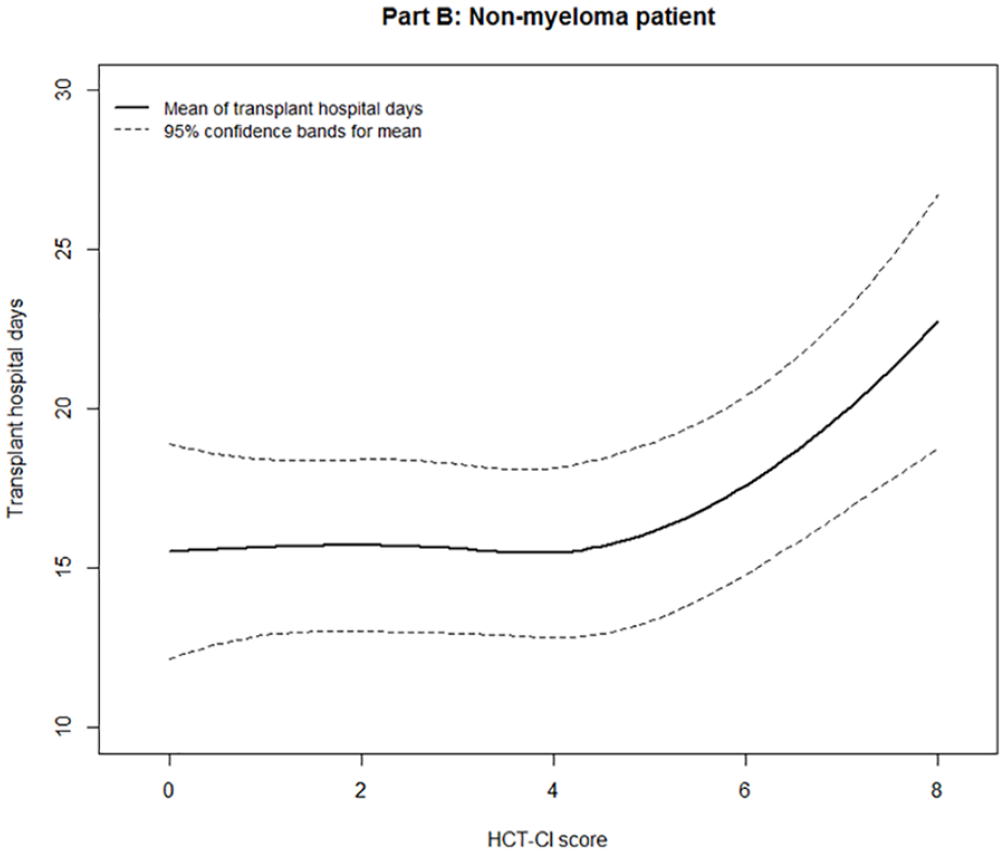
Estimated mean transplant hospital days for non-myeloma patients by HCT-CI score.
Discussion
In our autologous stem cell transplant population, the addition of age to the HCT-CI did not have statistically meaningful impact on length of stay, hospital days post-transplant, or ICU utilization after univariate and multivariate analyses. CD34+ cells infused was the only factor that affected hospital days. Although not found to be statistically significant, from an epidemiological perspective, there was a trend in higher ICU utilization when HCT-CI was examined in both the univariate and multivariate analyses. Our small sample size may be culpable for this non-significance, and further analysis into the relationship between HCT-CI and ICU utilization in autologous patients is warranted.
In our analysis, we initially dichotomized our patients based on HCT-CI of 3, which is comparable to the Sorror group. Importantly, the aforementioned study was examined in an allogeneic transplant population, which has a host of other factors influencing morbidity and mortality. Therefore, utilizing a higher HCT-CI score to determine patient candidacy to receive autologous stem cell transplant may be appropriate. We performed cubic spline modeling to interrogate the relationship between HCT-CI as a continuous variable and our outcomes of interest. In this model, number of transplant days increased linearly with each additional point above HCT-CI. Additionally, this finding was not sensitive to the patient’s malignancy (i.e. myeloma versus non-myeloma). This begs the question of whether HCT-CI should be further examined as a continuous interval to better prognosticate patients’ clinical courses. Although this may seem to be intuitive, there are real-world implications that come with extending a hospital stay from a mean of 15 days (HCT-CI = 4) to 22 days (HCT-CI = 8) with most notable being resource utilization. In a similar study exploring the role of HCT-CI to resource utilization in allogeneic stem cell recipients, DeCook and colleagues found a statistically significant longer length of hospitalization and all hospital days (25 versus 29 days within first 100 days of transplant) when exploring different HCT-CI scores and ages. Our data suggest that this increase in length of transplant hospitalization is not exclusive to allogeneic recipients and should be further explored in larger cohorts to determine incremental cost associated with increasing HCT-CI in ASCT recipients. Furthermore, we posit that clinicians should critically evaluate the expected safety of conducting ASCT in patients with high HCT-CI scores.
There are several limitations to our analysis. With this study being retrospective, selection bias exists as only patients receiving transplants were included. Our group did not have access to patients that were transplant ineligible due to high HCT-CI scores. Furthermore, the majority of disease states included in the HCT-CI are binary and do not describe the severity, or lack thereof, of the disease (i.e. psychiatric disturbance, diabetes, prior solid tumor). However, the authors feel this study design is similar to the real-world as the HCT-CI is scored as such. Other limitations include our dichotomous metric of ICU utilization; however, this is a pragmatic design to determine if higher HCT-CI scores at baseline led to ICU utilization, and thus downstream resource utilization. Our analysis did not include patients’ disease or remission status at transplant which may impact outcomes. Additionally, other baseline characteristics such as receipt of radiation therapy before or after transplant and prior lines of therapy were not recorded, which could alter patients’ outcomes. It is also important to note that our center does not utilize HCT-CI to determine conditioning intensity. This practice may differ from other transplant centers given the different impacts that reduced-intensity and myeloablative conditioning can have on post-transplant outcomes. Finally, our study did not examine why patients’ length of stays were longer than others. The authors find this to be generalizable to all transplant centers as complications after transplant can be heterogeneous, but length of hospital is easily comparable between centers.
In conclusion, the HCT-CI, with or without age, in an autologous stem cell transplantation did not predict length of hospitalization or utilization of the ICU. Consideration of the HCT-CI as a continuous variable should be examined further in larger studies.
Supplemental Material
sj-docx-1-cll-10.1177_09636897221080385 – Supplemental material for Age Adjusted Comorbidity Risk Index Does Not Predict Outcomes in an Autologous Hematopoietic Stem Cell Transplant Population
Supplemental material, sj-docx-1-cll-10.1177_09636897221080385 for Age Adjusted Comorbidity Risk Index Does Not Predict Outcomes in an Autologous Hematopoietic Stem Cell Transplant Population by Dylan Barth, Michael Singleton, Gregory Monohan, Brian McClune and Val Adams in Cell Transplantation
Footnotes
Ethical Approval
This study was approved by the institutional review board at the University of Kentucky, Lexington, Kentucky.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
Informed consent for patient information to be published in this article was not obtained because of the retrospective nature of this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.