
Abstract
Cardiovascular diseases are the leading cause of mortality and morbidity worldwide and account for more than 17.9 million deaths (World Health Organization report). Hypertension and aging are two major risk factors for the development of cardiac structural and functional abnormalities. Hypertension, or elevated blood pressure, if left untreated can result in myocardial hypertrophy leading to heart failure (HF). Left ventricular hypertrophy consequent to pressure overload is recognized as the most important predictor of congestive HF and sudden death. The pathological changes occurring during hypertensive heart disease are very complex and involve many cellular and molecular alterations. In contrast, the cardiac changes that occur with aging are a slow but life-long process and involve all of the structural components in the heart and vasculature. However, these structural changes in the cardiovascular system lead to alterations in overall cardiac physiology and function. The pace at which these pathophysiological changes occur varies between individuals owing to many genetic and environmental risk factors. This review highlights the molecular mechanisms of cardiac structural and functional alterations associated with hypertension and aging.
Introduction
Cardiovascular diseases (CVDs), affecting the heart and circulation, are the leading cause of mortality and morbidity. World Health Organization (WHO) reports that an estimated 1.13 billion people worldwide have hypertension, and between 2015 and 2050, the proportion of the world’s population over 60 years will nearly double from 12% to 22%. High blood pressure and aging are two independent and critical risk factors for CVDs. Uncontrolled/unattended hypertension leads to myocardial hypertrophy, subsequently progressing to cardiac failure 1 . The cardiac changes during aging go unnoticed until they require medical attention. Depending upon the duration and nature of the stimulus, hypertensive heart disease (HHD) can either lead to concentric or eccentric hypertrophy with either a preserved or a reduced left ventricular (LV) ejection fraction (LVEF) ultimately resulting in malfunctioning of the heart. The progression of hypertrophy during hypertension occurs initially as a compensatory mechanism to maintain the cardiac output due to increased wall stress. The adaptive remodeling in course of time advances to maladaptive remodeling, pushing the heart to a decompensated stage. The transition from compensatory phase of left ventricular hypertrophy (LVH) to decompensatory phase remains enigmatic and still eludes an answer. Many physiological, cellular, and molecular mechanisms have been proposed to explain the transition from hypertrophy to failure. The pathological changes of the heart in patients with LVH include an increase in the size of the cardiomyocyte, alterations in the extracellular matrix (ECM) with accumulation of collagen and fibrosis, and abnormalities of the intramyocardial coronary vasculature 2 –4 . The neurohormones, growth factors, and cytokines also influence the progression of hypertrophy. LVH is a significant intermediate phenotype in the progression of HHD 5 and is associated with adverse outcomes 6 . LVH remains a powerful pathological factor for driving cardiac failure, and hence finding a potential cause for the transition will pave the way for better treatment strategies.
Hypertensive Heart Disease
Hypertension is a key risk factor for LVH and in the development of clinical heart failure (HF). Unattended high blood pressure is considered to be the major risk factor for coronary artery diseases and HF. Hypertension accounts for about one quarter of HF cases as reported by the Framingham study, which are considered the leading cause of mortality by WHO. Arterial blood pressure is influenced by cardiac output and peripheral vascular resistance. Stroke volume and heart rate that controls cardiac output are dependent on the myocardial contractility and size of the vascular compartment. The function and structure of blood vessels affect the vascular resistance. Prolonged, untreated hypertension can lead to maladaptive remodeling in the myocardial structure and coronary vasculature, thus resulting in coronary artery disease. Consequent to pressure overload, the heart muscles thicken to counterbalance the increased stress and thus maintain the ejection fraction (EF). This initial hypertrophic response of increased myocyte size in the heart occurs as a compensatory mechanism. On progression, the adaptive remodeling becomes maladaptive, leading to cardiac failure 1 . Various hemodynamic, structural, neuroendocrine, cellular, and molecular factors play integral roles in the development of hypertension and associated abnormalities. Abnormalities in the renin–angiotensin–aldosterone system and sympathetic nervous system, endothelial dysfunction, and vascular inflammation can independently contribute to hypertension 3,4,7,8 . Also oxidative stress that develops in the early stages of hypertension results in further release of reactive oxygen species (ROS), contributing to hypertension-induced irregularities 9 . The complications of HHD include LVH, HF, coronary artery diseases, ischemic heart disease, arrhythmia, sudden cardiac death, and stroke. β-Blockers, calcium channel blockers, angiotensin converting enzyme inhibitors, angiotensin receptor blockers, and renin inhibitors are the commonly prescribed antihypertensive agents. Hypertension plays a key role in the evolution of cardiac failure. In an attempt to compensate for the increased peripheral resistance noted in hypertension, the myocardium enlarges, leading to myocyte hypertrophy and fibrosis. Eventually, LV failure occurs when the hypertrophied and/or fibrotic myocardium is no longer able to maintain normal cardiac output. HHD progresses with initial LVH leading to diastolic dysfunction followed by systolic dysfunction.
Cardiac Hypertrophy
Heart responds to various environmental stressors by either enlargement or atrophy. The reactions will depend particularly on the type, duration, and strength of the stimuli 9 . In addition to cardiomyocytes, heart also harbors smooth muscle cells, endothelial cells, fibroblasts, mast cells, and resident cardiac stem cells. Cell-to-cell communication in the heart directs integrated biological responses to the altered environment with the help of various transcription factors (TFs) and other signaling molecules. The autocrine and paracrine factors released by cells act on various target cell types to perform the desired cellular function. Congestive HF is a common end point of many abnormal cardiac conditions, including hypertrophy. When compensatory mechanisms that become activated during cardiac hypertrophy fail, congestive HF is manifested and is associated with an unfavorable prognosis. HF subsequent to cardiac hypertrophy remains a major clinical problem, and the mechanisms for the transition still remain elusive.
Pathological Cardiac Hypertrophy
Pathological hypertrophy occurs in response to chronic pressure or volume overload. It is often confused with physiological hypertrophy, a reversible cardiac condition observed mainly in athletes and pregnant women. It is mostly seen consequent to diseases like hypertension, valvular disease, myocardial infarction, ischemia, inherited genetic mutations, or diabetes. It is considered to be an intermediate stage in the transition to HF. It is also associated with increase in cardiomyocyte size and cardiac mass. In the initial phase of hypertrophy, in response to hypertensive stress, cardiac efficiency is maintained and is termed as the “adaptive phase” or “compensatory phase.” Here the myocytes increase in thickness in order to cope up with the increased pressure on the ventricular wall and to preserve the cardiac output. Prolonged hypertension-induced hypertrophy can result in the transition from adaptive to maladaptive remodeling which is characterized by reduced EF and LV dilatation. Advanced stage of hypertrophy is associated with severe cardiomyocyte loss and fibrotic remodeling and is characterized by systolic and diastolic dysfunction which predisposes to development of cardiac failure or even sudden death 10 . Cardiomyocyte loss is mediated by apoptosis or necrosis due to either excessive ROS, inflammatory response, or mitochondrial damage, and is often replaced by collagen, thus leading to cardiac fibrosis. The accumulation of collagen results in the stiffening of the ventricular wall leading to the impairment of contraction and relaxation of the left ventricle. The electrical conduction is disturbed due to the presence of extensive fibrotic tissue, leading to arrhythmias 11 . Angiogenesis is compromised in pathological hypertrophy, therefore reduced capillary density increases oxygen diffusion distances leading to myocardial ischemia 12 .
Normal heart relies on fatty acid oxidation for the production of Adenosine Tri Phosphate (ATP) needed for the proper functioning whereas glucose and lactate oxidation accounts for only 30% of energy production. The heart is able to switch between fuel consumption depending on the demand and is considered as an adaptive response. However, in pathological hypertrophy, there is reduced fatty acid oxidation and increased dependence on glucose for ATP production. This is because the oxygen supply is limited and the transport of fatty acid is impaired in pathological hypertrophy. In advanced state of hypertrophy, glucose metabolism decreases the overall ability of the heart to generate ATP 13,14 .
Cellular and Molecular Mechanisms in Pathological Hypertrophy
Reactivation of fetal gene program is observed in pathological cardiac hypertrophy 15 . Fetal recapitulation occurs with molecular changes similar to that observed during fetal cardiac development and includes stimulation of atrial natriuretic peptide, B-type natriuretic peptide, and genes for fetal isoforms of contractile proteins. It is accompanied by downregulation of myocardial genes, such as β-myosin heavy chain (MHC) and upregulation of α- MHC 16 . The various TFs mediating the reactivation of fetal gene program are Nuclear Factor of Activated T cells (NFAT), Nuclear factor kappa-light-chain-enhancer of activated B cells (NF-kB), Myocyte Enhancer Factor-2 (MEF2), Transcription Factor GATA4 (GATA4), and Serum Response Factor (SRF). These TFs are implicated to play a prominent role in embryonic development 16 –18 . The re-expression of fetal genes is used as a marker of pathological cardiac remodeling. The aberrant expression of genes involved in fetal contractile proteins and cardiac metabolism leads to progressive myocardial dysfunction and pathogenesis. One of the critical signaling pathways associated with cardiac hypertrophy includes insulin-like growth factor receptor 1 (IGF1)–phosphoinositidine-3-kinase–protein kinase B pathway 19 . Studies have shown that the activation of Insulin Like Growth Factor 2 Receptor (IGFIIR) is critical for the development of angiotensin-induced cardiac hypertrophy 20 . The other pathways that are significantly modulated in hypertrophied heart are mitogen-activated protein kinases (MAPKs; e.g., Extracellular Signal-Regulated Kinases (ERKs), c-Jun NH(2)-terminal kinase (JNKs), and p38) 21 , dual-specificity MAPK phosphatases 22 , and protein kinase C isoforms 23 .
The changes of the myocardium occurring during pathological hypertrophy not only affect the parenchyma but also the stroma, which forms the ECM. The ECM is composed of fibroblasts which secrete collagen along with smaller amounts of elastin, laminin, and fibronectin. The fibrillar collagen provides structural integrity to adjoining myocytes and aids in myocyte contraction that translates into efficient cardiac contraction 24 . Pathological hypertrophy is associated with increased interstitial and perivascular fibrosis 4 . Myocyte loss due to apoptosis and necrosis is replaced by collagen deposition. However, disproportionate accumulation of collagen increases ventricular stiffness and altered microcirculation resulting in impaired cardiac function and adverse cardiovascular events 25 . The augmented fibrosis coupled with reduced capillary density increases the risk for oxygen deprivation resulting in myocardial ischemia 26 .
Variants of Hypertrophy
Depending on the initiating stimuli, cardiac hypertrophy has classically been subdivided as concentric or eccentric 27 . Concentric hypertrophy is observed in response to pressure overload pathological stimuli such as hypertension and aortic stenosis. An increase in relative wall thickness and cardiac mass, with a small reduction in chamber volume, is observed in concentric hypertrophy. In contrast, eccentric hypertrophy leads to increase in cardiac mass due to increased chamber volume. Pathological conditions which induce volume overload such as aortic regurgitation and arteriovenous fistula cause diastolic wall stress leading to eccentric cardiac hypertrophy 28 . Concentric hypertrophy is characterized by parallel addition of sarcomeres leading to an increase in width of individual myocytes. In eccentric hypertrophy, sarcomere units are added in series resulting in relatively increased length of the myocytes. Clinical studies suggest that eccentric cardiac hypertrophy poses greater risk than concentric cardiac hypertrophy since it progresses to ventricular dilation and systolic failure 29 .
Changes in Cardiac Function with Pathological Hypertrophy
According to Framingham Heart Study, each increase in LV mass of 50 g/m of height was associated with 1.5-fold increase in CVDs 30 . Cardiac electrical abnormalities are evident in most of the experimental models of hypertrophy exhibited as prolonged action potential and conduction and repolarization abnormalities 31,32 . The parameters like QT interval (QTc), ST height, R amplitude, P amplitude, and PR interval are significantly decreased in hypertrophic mice. This analysis also established a method to distinguish between wild-type and hypertrophic phenotype using echocardiographic features. The hypertrophic mice had enlarged LV, interventricular septa, right ventricles, and atria, typical of concentric hypertrophy compared to wild type. Also the Electrocardiography (ECG) of hypertrophic mice was characterized by increased voltage as evident by higher P- and R- amplitudes, wider QRS complex, prolonged QTc interval, and LV strain. In isoproterenol-induced cardiac hypertrophy, the T-wave inversion observed is due to changes in action potential 33 . LV mass directly affects the ST-segment and T-wave abnormalities whereas the total heart weight affected the QTc interval. In patients with hypertrophic cardiomyopathy, abnormalities in ST-segment and T-waves have been reported 34 .
Transition from Hypertrophy to Failure
HHD commonly results in concentric hypertrophy, a nondilated thick-walled left ventricle typically associated with a normal LVEF, and is the common precursor to LV failure 26 . The transition from concentric LV hypertrophy to failure has been demonstrated in animal models including the spontaneously hypertensive rats (SHRs) 35 , in surgical aortic banding model, in transgenic rodent models, and in humans with aortic stenosis or familial hypertrophic cardiomyopathy 36 .
A number of factors are identified as mediators for the transition from cardiac hypertrophy to failure. In pressure overload model, PGC-1β deficiency is shown to accelerate the transition to HF. Peroxisome proliferator-activated receptor-gamma coactivator, PGC-1α and PGC-1β regulate mitochondrial biogenesis and genes encoding for enzymes and proteins of mitochondrial metabolism and electron transport chain and are primarily expressed in oxidative tissues 37 . The contribution of PGC-1β to mitochondrial function and gene expression in nonstressed hearts and to maintaining contractile function under pathological increased workload has been identified 38 . PGC-1β and PGC-1α play partially overlapping but distinct roles in maintaining cardiac mitochondrial energetics in the unstressed heart with both pathways regulating the expression of genes involved in oxidative phosphorylation whereas PGC-1α predominantly regulates fatty acid oxidation. However, both isoforms contribute to the maintenance of cardiac function in the context of pressure overload. The modulation of PGC-1β activity represents a promising target for limiting the transition from pressure overload cardiac hypertrophy to HF 39 . This study also underscores the potential role of additional mechanisms such as oxidative stress that is exacerbated by deficiency of the transcriptional coactivators in contributing to the accelerated transition to decompensated HF.
Adverse remodeling of T-tubule in intact hearts is observed during compensated hypertrophy that is tightly associated with the decline of myocardial function. T-tubule is a highly organized ultrastructural substrate for excitation–contraction (EC) coupling in ventricular myocytes. T-tubules are essential for the initiation and synchronous triggering of sarcoplasmic reticulum (SR) Ca2+ release and hence it is an important determinant of myocyte function 40 . A significant loss of T-tubule density with T-tubule disorganization in ventricular myocytes was first identified in a dog model with pacing-induced HF 41 . Several discrepancies regarding T-tubule remodeling were resolved by a study in HF patients which found a pronounced T-tubule loss irrespective of the different cardiac etiologies. T-tubule remodeling is an important event that occurs before the onset of HF and is not a secondary modification after HF 42 . This study using SHRs in HF also showed that T-tubule disorganization led to an increase in orphaned Ryanodine receptors, which led to the loss of local control of Ca2+-induced Ca2+ release resulting in decreased EC coupling efficacy and increased dyssynchrony of SR Ca2+ release. Progressive deterioration of T-tubule structure in ventricular myocytes was observed throughout the disease development. The strong correlation between LV function and T-tubule disorganization makes it a critical factor mediating the transition from compensated hypertrophy to HF.
A study in Dahl salt-sensitive rat myocytes observed that alterations in EC coupling occur in LV myocytes during the transition from compensated hypertrophy to HF 11 . Prolongation of contraction and relaxation may be an early indicator of abnormalities in myocyte mechanical function during the transition. A shift in MHC isoforms from the V1 to the V3 isoform was observed during the development of cardiac hypertrophy or failure in rats 16 . The altered catalytic hydrolysis of ATP by changes in the activity of myosin ATPase will affect maximal rates of energy liberation during the cross-bridge cycle. The isoform shift may affect the time course of the contraction and represents a compensatory mechanism to maintain the contraction amplitude. A decrease in contractility will be observed when the prolongation of contraction time course can no longer preserve the adequate contractile function with disease progression. Apoptosis of cardiac muscle cells (myocytes) is suggested to be one of the determinants of transition from compensated to decompensated hypertrophy leading to heat failure. Oxidative stress, implicated in hypertension and hypertrophy, is known to trigger mitochondrial death pathway43,44 . The organelle mitochondrion is the primary site of action for key apoptotic regulatory factors, including the B-cell lymphoma 2 (Bcl-2) family of proteins. An increase in the ratio of Bcl-2 like protein 4, Bax to Bcl-2 in the outer mitochondrial membrane determines the survival or death of a cell following an apoptotic stimulus 45 . This increase leads to collapse of the mitochondrial membrane potential and translocation of cytochrome-c into the cytoplasm, thereby triggering the caspase cascade and subsequent apoptotic cell death. Activation of caspase cascade and upregulation of Bcl-2 proteins during the transition to pressure overload–induced HF was reported in a sheep model 46 . Activation of apoptotic factors is also reported in guinea pigs during the transition from cardiac hypertrophy to failure 44 .
Increased reactive oxygen species is an important and the main contributing factor for the downstream pathways involved in the development and progression of hypertrophy 47,48 . An increase in free radicals or a relative deficit in the endogenous antioxidant reserve leading to oxidative stress can cause contractile dysfunction 47 and has been suggested as one of the contributing factors in the transition of compensated heart hypertrophy to the decompensated stage. The increase in cardiac workload observed in hyperfunctional heart hypertrophy is associated with increased endogenous antioxidant enzyme activities 49 . HF due to a variety of conditions has been shown to be associated with oxidative stress indicated by reduced antioxidants, a depressed redox state, and increased lipid peroxidation. Treatment using antioxidant Tempol has been shown to be protective for compromised cardiac stem cells in hypertension-induced cardiac hypertrophy 50 .
Molecular chaperones direct the correct folding of proteins. the failure of which leads to accumulation of misfolded proteins. The deletion of the HSPA4, a member of heat shock protein family (HSP) 110, was found to induce cardiac hypertrophy and fibrosis 51 . However, some molecular chaperones can induce hypertrophic signaling. For instance, Hsp90 was found to associate with cell division cycle 37 and modulated cardiac hypertrophy 52 . Long noncoding ribonucleic acids (lncRNAs) and microRNAs (miRNAs) have been implicated in cardiac hypertrophy and its transition to HF 53 . miR-208 was discovered to be associated with myosin gene expression and cardiac hypertrophy 54 . Several other miRNAs like miR-24, miR-21, and miR-1991 are found to be upregulated in hypertrophy and failing myocardium 55,56 . Replacement therapy with miR-455 aggravated pressure-induced cardiac hypertrophy by targeting calreticulin 57 . Several lncRNAs have been identified in cardiac physiology and disease. The expression of the cardiac hypertrophy–related factor is upregulated whereas the MHC-associated RNA transcript is downregulated in cardiac hypertrophy 58,59 .
The mechanisms by which the heart adapts to chronic pressure overload by undergoing adaptive remodeling and its transition eventually leading to HF are still not well defined. Mining new mechanisms involved in the transition will help in developing new and efficient therapeutic strategies.
Cardiac Changes Associated with Aging
Aging is associated with physiological changes in all organ systems, including the vasculature and heart. With aging, physiological functional capacity of various organs, cardiovascular responsiveness, and autonomic homeostasis go down. Aging starts with birth and accelerates with advancing age. The alterations that occur during the aging process go unnoticed for a long time until it requires medical attention. The risk for various diseases increases dramatically with age. Aging is a dominant risk factor for CVDs and predisposes the heart to various adverse structural and functional alterations. A high prevalence of HF is noted in the older population, generally above the age of 65. Many of these changes are the consequence of CVDs. Nevertheless, changes can occur even in the absence of clinical cardiac dysfunction.
Microscopic changes like increase in intimal thickness and deposition of collagen with aging ultimately lead to arterial wall thickening and stiffness. This is manifested as increased systolic blood pressure and pulse wave velocity as well as widening of the pulse pressure. Arterial stiffness can lead to the development of LVH as a result of increased afterload and wall stress. In the heart, myocardial volume is found to be unaltered with age. Between 30 and 70 years of age, 35% of the total myocytes in the ventricle is reported to be lost 60,61 . To compensate for the cell loss, the remaining myocytes undergo hypertrophy and this occurs along with the expansion of the nonmyocyte compartment. Though the reason for cell death is unclear, reduction in capillary density is noted to occur with aging leading to ischemic injury 60 .
An age-dependent increase in the prevalence of LVH in healthy individuals has been reported in the Framingham Heart Study and the Baltimore Longitudinal Study on Aging without concomitant CVDs. They have also shown age-dependent decline in diastolic function and relatively preserved systolic function at rest 61 . A decline in exercise capacity and the prevalence of atrial fibrillation is also implicated with aging. In older population during exercise, increase in heart rate and EF indicates reduced cardiac reserve 62,63 . Myocardial performance index (MPI) increases with age which indicates that a greater fraction of systole is spent to cope with the pressure changes during isovolumetric phases. MPI has been shown to reflect both LV systolic and/or diastolic dysfunction 64 . These variations are independent of the conventional risk factors for heart disease such as smoking, hypertension, blood lipid levels, and diabetes. Hence they may be considered to be part of intrinsic cardiac aging. In the absence of systolic HF, diastolic dysfunction is increasingly seen in the elderly, a condition named as HF with preserved EF 65 .
Mouse models are normally used for cardiac aging studies since they closely recapitulate the phenotypes of human cardiac aging 66 . The relatively short lifespan and the availability of genetically modified mice are other advantages of using mouse model for studying molecular mechanisms of cardiac aging. Laboratory mice do not develop elevated blood pressure or adverse blood glucose and lipid profiles which allow the investigation on intrinsic cardiac aging without the added cardiac complications. The echocardiography performed on a mouse model exhibited phenotypic changes like increased LV mass, decreased diastolic function, and worsened MPI similar to human cardiac aging 67 .
With aging, the heart rate of wild-type mice does not vary significantly. The ECG parameters that exhibit strong correlation with heart weight are QTc interval, QRS duration, ST height, R amplitude, P amplitude, and PR interval. Of these the most sensitive parameter is QTc length, and the most specific parameters are P- and R-wave amplitude, QRS duration, and ST height. Studies that analyzed the echocardiographic functions of young (1–2 months) and old mice (7–9 months) found that R-wave amplitude was the only parameter that was significantly decreased with aging 33 .
Cellular and Molecular Mechanisms in Aging Heart
The functional abnormalities of the aging myocardium occur not only due to structural changes but also due to cellular and molecular alterations. Multiple molecular mechanisms are involved in the pathogenesis of cardiac aging. Hypertrophy of the heart is a hallmark of cardiac aging. Nutrient and growth signaling in the heart are altered with advancing age due to hypertrophy. Two major signaling pathways implicated in cardiac hypertrophy and aging are mechanistic target of rapamycin (mTOR) and insulin-like growth factor-1 (IGF-1). mTOR regulates growth and has been shown to be a major modulator of aging and age-related diseases. Increased mTOR signaling impairs and reduced mTOR signaling improves resistance to cardiac aging in mouse models 68 . One of the best characterized pathways of lifespan regulation in animal models is insulin/IGF-1 signaling. Deficiency in insulin/IGF-1 signaling attenuates age-related cardiomyocyte dysfunction in mice. Age-dependent decline in serum IGF-1 levels in humans is associated with increased risk of HF. Unlike the observations in mice, interventions that increase IGF-1 signaling were beneficial in HF in rat. In aged rats, IGF-1 treatment was protective against mitochondrial oxidative stress 69 . These studies confirm the beneficial effects of IGF-1 to mitochondrial protection mechanisms.
The vicious cycle of ROS-induced ROS release seen in dysfunctional mitochondria can lead to cellular and organ functional damage that limits lifespan 70 . Mitochondrial ROS production in heart is found to increase with advancing age. The mitochondria are usually enlarged with swelling along with loss of cristae in aged cardiomyocytes. The inner membranes of mitochondria are destructed and are deficient in ATP production 71 . One of the key regulators of mitochondrial biogenesis, peroxisome proliferator–activated receptor coactivator 1α (PGC-1α) enhances mitochondrial function in the heart 72 . The expression of PGC-1α is repressed in the failing heart. The mitochondrial gene expression was reduced in PGC-1α knockout mice and was found to develop cardiac dysfunction at 7 months of age 73 . Mitochondrial dysfunction and aberrant ROS production contribute to aging through both direct damage to cellular macromolecules and interfering with normal signaling and energetics.
ECM is a complex collection of proteins located outside the cells. The function of ECM is to provide structural and biological support to the surrounding cells. The primary sources of cardiac ECM proteins are cardiac fibroblasts, which secrete proteins like collagen type I, II, III, IV, V, and VI, elastin, fibronectin, laminin, and fibrinogen 74 . Excessive ECM deposition increases the stiffness of the myocardium and mediates diastolic dysfunction 75 . The synthesis and degradation of ECM proteins are dynamically regulated by matrix metalloproteinases (MMPs), tissue inhibitors of MMPs (TIMPS), and other proteases. Myocardial fibrosis and deregulation of ECM protein synthesis and degradation are observed in aging heart. Profibrotic factor, like transforming growth factor-β, has been shown to induce the expression of ECM proteins and also inhibit matrix degradation by MMPs 76 . The expression of another matricellular protein, secreted protein acidic and rich in cysteine, was found to be increased with age, and its deletion resulted in reduced fibrillar collagen in the LV and decreased LV diastolic stiffness 77 . These evidences suggest the critical role played by ECM proteins in diastolic dysfunction during aging. MMPs are zinc-dependent enzymes that regulate ECM degradation whereas TIMPS regulate MMP proteolytic activity in the tissue 78 . MMPs and TIMPs are differentially regulated by aging but their roles in cardiac aging have not been established.
Adult tissues harbor a small portion of embryonic stem cells from the inner cell mass/blastocysts and retain their developmental potential. These tissue-specific stem cells play an important role in the normal homeostasis of the organ as well as aid in regeneration or repair during damage. Depending upon their tissue location, stem cells reveal a tremendous heterogeneity in growth kinetics, differentiation, and survival. Appropriate balance between stem cells, precursor cells, and differentiated cells is maintained by various feedback mechanisms that regulate the proliferation, survival, and differentiation signals 79 . Stem cells are carefully regulated so as to meet the demands of the tissue in which they reside, especially when injured. Various intrinsic regulators like telomerase and Bcl-2 family members and extrinsic regulators like Notch signaling pathway, growth factors/cytokines, and cell adhesion molecules influence the fate of stem cells. Stem cells comprise only a very small population within a tissue which makes it hard to delineate the cellular and molecular changes that occur with aging. The difficulty of obtaining pure stem cell populations in sufficient quantities to perform various analyses is yet another barrier. However, considering the importance of stem cells in tissue homeostasis, analysis of these cells is imperative in aging research. Understanding the molecular pathways involved in age-dependent deterioration of stem cell function will be critical for developing therapeutic strategies for aging-related diseases.
Previous studies have examined the effect of aging and HF on cardiac stem cells 80 . The human Cadiac Stem Cells (hCSCs) from explanted human hearts exhibited lower proliferative capacity, lower migration rate, high expression of senescent markers, and lower telomerase activity compared to hCSCs from donor hearts. However, a definite distinction between physiological and pathological aging was not possible since the donors were younger compared to older patients who underwent transplantation. Also variations in the disease pathologies in these patients made the comparison less possible 80 . Though not conclusive, this study for the first time reported the age- and disease-associated decline in the functional ability of hCSCs.
An age-dependent study on the quality and quantity of cardiosphere-derived cells (CDC) found that the impact of age on CDCs was quite limited though there was variation in CDC characteristics between patients. Though the growth rate, growth factor production, and angiogenic potency of CDCs were not impaired with age, the CDCs from older patients exhibited senescent markers and damaged DNA 81 . These studies have important clinical implications for autologous stem cell transplantation in elderly patients. A study by Saheera et al. found that the cardiac stem cell efficiency deteriorated with physiological aging in rats. Cardiac stem cells isolated from adult Wistar rats, when compared to pups, showed signs of aging as confirmed by their decreased density, proliferation, and migration potential. Also, deterioration of stem cell attributes was accelerated in HHD. The study used SHR, which is a genetic model of hypertension. The proliferation and migration potential were reduced whereas proportion of senescent cells and DNA damage was increased in SHR compared to normotensive Wistar rats 82 .
The differences and similarities of the cardiovascular changes associated with HHD and aging are depicted in Fig. 1.
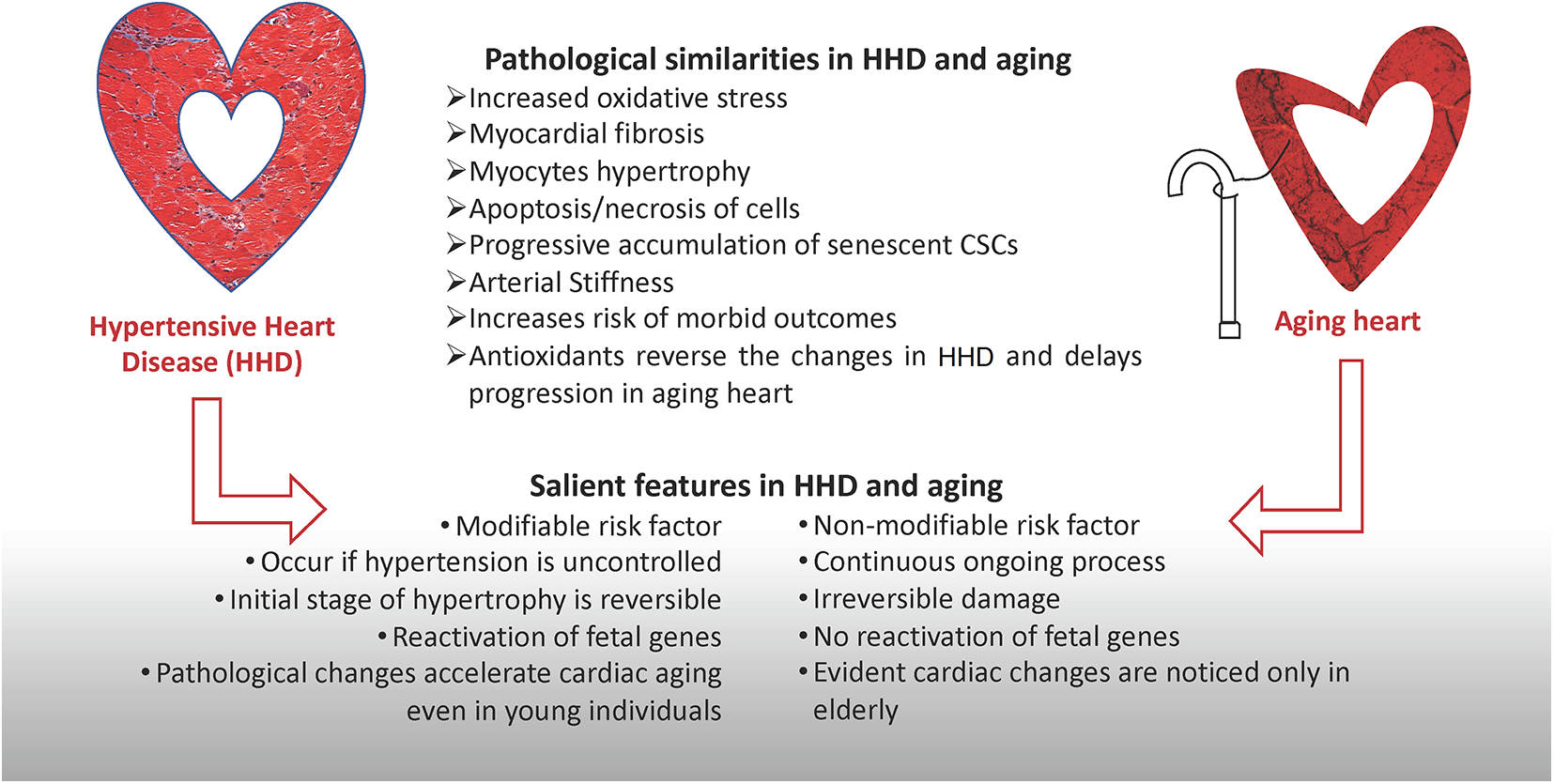
The differences and similarities of the cardiovascular changes associated with hypertensive heart disease and aging. CSC: cardiac stem cell
Conclusion
Chronological age is a contributing factor for the changes in the cardiovascular structure and function. The presence of cardiovascular ailments accelerates the cardiac aging process. The changes observed in HHD and aging are more or less similar in terms of the cellular and molecular mechanisms. In both hypertension and aging, increased oxidative stress is a major source for the activation of signaling molecules and its downstream pathways culminating in the expression of genes involved in functional and phenotypical alterations. Cardiac aging is a complex process and involves intrinsic and extrinsic factors. Management of aging with well-balanced diet and lifestyle will help to maintain the heart young and healthy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is supported, in part, by the National Institutes of Health (NIH) grants HL116729 and HL138023 (to PK) and American Heart Association Transformational Project Award 19TPA34850100 (to PK).