
Abstract
Intravoxel incoherent motion has received extensive attention in brain studies for its potential as a non-invasive magnetic resonance perfusion method. However, studies on intravoxel incoherent motion imaging and crossed cerebellar diaschisis detection are relatively scarce. The aim of our study was to evaluate the feasibility of using intravoxel incoherent motion imaging in crossed cerebellar diaschisis diagnosis in subacute ischemic stroke patients by comparing results from intravoxel incoherent motion imaging, single-photon emission computed tomography, and arterial spin-labeling perfusion methods. In total, 39 patients with subacute ischemic stroke who underwent intravoxel incoherent motion, arterial spin-labeling, and single-photon emission computed tomography scanning were enrolled. Intravoxel incoherent motion-derived perfusion-related parameters including fast diffusion coefficient, vascular volume fraction, arterial spin-labeling-derived cerebral blood flow as well as single-photon emission computed tomography-derived cerebral blood flow of bilateral cerebellum were measured. A crossed cerebellar diaschisis-positive result was considered present with an asymmetry index ≥10% of single-photon emission computed tomography. In the crossed cerebellar diaschisis-positive group, fast diffusion coefficient, arterial spin-labeling-derived cerebral blood flow, and computed tomography-derived cerebral blood flow of the contralateral cerebellum decreased compared with those of the ipsilesional cerebellum; whereas vascular volume fraction significantly increased. The National Institutes of Health Stroke Scale score and infarct volume in the crossed cerebellar diaschisis-positive group were significantly higher than those in the crossed cerebellar diaschisis-negative group. A positive correlation was detected between the fast diffusion coefficient-based asymmetry index and the single-photon emission computed tomography-based asymmetry index, fast diffusion coefficient-based asymmetry, and arterial spin-labeling based asymmetry index; whereas the vascular volume fraction-based asymmetry index value had a negative correlation with the single-photon emission computed tomography-based asymmetry index and arterial spin-labeling based asymmetry index. Furthermore, the area under the receiver operating characteristic curve value of the arterial spin-labeling-based asymmetry index was 0.923. The fast diffusion coefficient derived from the intravoxel incoherent motion could be valuable for the assessment of crossed cerebellar diaschisis in supratentorial stroke patients.
Introduction
When an ischemic cerebral stroke occurs, a series of excitotoxicity, apoptosis, and cell death is activated, which may lead to morbidity and mortality 1 . As a common radiological phenomenon, crossed cerebellar diaschisis (CCD) is characterized by hypoperfusion and hypometabolism of the contralateral cerebellar hemisphere, which results from the dysfunction of the related supratentorial region 2 . CCD has been reported in many acute and chronic brain diseases, such as supratentorial stroke, cerebral hemorrhage, infection, tumor, and epilepsy 3 –7 . Growing evidence indicates that CCD plays an important role in assessing neurological improvement and clinical outcomes after infarction 8 –10 . For example, Takasawa et al. have shown that the severity of asymmetry indices (AI) of single-photon emission computed tomography (SPECT) in the early subacute stage correlates significantly with both the final modified Rankin scale and the Barthel Index scores, two indices that represented the clinical outcome 9 . These findings imply that CCD may be a valuable predictor of functional impairment in patients suffering supratentorial infarction.
CCD manifests as decreased cerebellar cerebral blood flow (CBF), which was first observed in a stroke patient using positron emission tomography (PET) in 1981 11 . Based on our knowledge, PET and SPECT have been established as the reference standards for CCD detecting 12,13 . However, the two methods involve the contrast agent injection and radiation exposure, which would inevitably limit their clinical use due to critical concerns among patients. With the development of magnetic resonance (MR) perfusion techniques, many researchers have tried to assess CCD through radiation-free methods. For instance, dynamic susceptibility contrast perfusion-weighted imaging was found to be able to identify CCD by various parameters but the detection rate was lower than PET/SPECT 12 . Chen et al. also observed that arterial spin-labeling (ASL) was useful to detect CCD after stroke because of the consistent results with PET/SPECT series 14 .
Intravoxel incoherent motion (IVIM) MR imaging (MRI), a method that measures the relationship between signal attenuation with multiple b values, could simultaneously estimate the diffusion and perfusion parameters in a noninvasive way 15 . Le Bihan et al. initially obtained the images of diffusion and perfusion through IVIM imaging technique in brain tumor and ischemia 16 . By applying the bi-exponential model, several parameters such as the slow diffusion coefficient (D), the pseudodiffusion fast diffusion coefficient (D*), and the perfusion vascular volume fraction (f) could be obtained from IVIM 17,18 . With the development of IVIM, many researchers have explored and revealed the diagnostic value of IVIM in various diseases 18,19 ,including ischemic stroke 15 . In the previously mentioned IVIM study on stroke, decreases in D, D*, and f were found in the ischemic stroke hemisphere compared with the contralateral side, which was in accordance with the pathophysiology of stroke 20 . Another IVIM study also showed a reduction in f in the infarcted area in acute stroke 21 . According to our literature review, limited information exists on whether IVIM could detect CCD phenomenon in brain diseases.
Thus, the aim of this study was to evaluate the feasibility of using IVIM MRI in CCD diagnosis in patients with subacute supratentorial stroke and compare the results from IVIM with those from SPECT and ASL in identifying CCD.
Materials and Methods
Patients
The whole study followed apporval from the hospital insititutional research ethics board, and all subjects have written informed consent. A retrospective review of our institution’s clinical and imaging database identified 56 patients who were diagnosed with subacute ischemic stroke from August 2013 to December 2014 and underwent IVIM and ASL MRI and SPECT. The definition of subacute stroke was 24 h to approximately 2 weeks from onset according to the study by Kim et al 22 .
Among these patients, 17 were excluded for having one or more of the following conditions: (1) infarct in the brain stem, cerebellum, or bilateral supratentorial infarct; (2) history of intracranial tumor, head trauma, subarachnoid hemorrhage, arteriovenous malformation, or brain surgery; (3) abnormalities in the posterior fossa on T1, T2, and diffusion-weighted MR images; (4) MR angiography showing angiopathy of vertebral basilar artery and the major branches. Of the 39 study patients, 25 were men (mean age 60.6 years; age range 34.0–84.0 years) and 14 were women (mean age 65.64 years; age range 43.0–84.0 years), with an overall mean age of 62.41 years (age range 34.0–84.0 years). The mean duration from stroke onset to MRI in the CCD-positive and the CCD-negative groups were 6.52±3.54 days and 5±3 days, respectively. Meanwhile, the mean time interval from stroke onset to SPECT was 5.75±2.94 days and 4.9±4.84 days, respectively. The National Institutes of Health Stroke Scale (NIHSS) was used to evaluate the neurological and functional status at the time of the admission and at discharge (14 days later).
MRI
All MRI examinations were performed on a 3-T platform (HDxt; General Electric Medical Systems, Waukesha, WI, USA) with a standard eight-channel phased array head coil. The imaging protocol included T1-weighted, T2-weighted, MR angiography, ASL, and IVIM imaging sequences. IVIM imaging was performed through multi b-value diffusion-weighted imaging using a single-shot spin-echo echo planar imaging sequence with the diffusion-weighted gradients along three orthogonal directions and the following parameters: repetition time/echo time = 6000/88 ms, field of view = 260 × 260 mm2, matrix size = 192 × 192, in-plane resolution = 1.35 × 1.35 mm2, 18 slices with a slice thickness/spacing of 5/1.5 mm, bandwidth = 1950 Hz, acceleration factor = 2, number of averages = 2, b values = 0, 20, 50, 100, 150, 200, 500, 800, and 1000 s/mm2, and acquisition time = 5 min. Pseudo-continuous ASL perfusion images were collected using three-dimensional (3D) fast spin echo acquisition with background suppression, with a post labeling delay of 1500 ms. Other parameters were repetition time/echo time = 4601/10.5 ms, field of view = 240 × 240 mm2, matrix size = 128 × 128, 38 slices with a slice thickness of 4 mm, and number of averages = 3.
SPECT imaging
SPECT was performed in all patients in a silent, dimly lit room with their eyes open and ears unplugged. Approximately 20–25 minutes after intravenous injection of 925–1110 MBq (25–30 mCi) technetium-99methylcysteinatedimer (HAT Co. Ltd. Shanghai, China), data acquisition was done on a dual-headed rotating scintillation gamma camera (Infinia Hawkeye 4, General Electric Medical Systems) with the patient supine, headrest attached, smallest permissible radius of rotation, 128 × 128 matrix, 360°, 120 projections, 25 seconds per view for a total 64 views by using a low-energy high-resolution parallel hole collimator. A 20% window centered at a 140 KeV photopeak for Tc-99 m was used. Raw data were smoothed with the Butterworth filter.
Imaging data processing
IVIM-MRI images were transferred to the dedicated workstation (ADW 4.5; General Electric Medical Systems) for post-processing. IVIM parameters including D, D*, and f were calculated by using the bi-exponential model expressed as follows:

where S(b) and S0 denote the signal intensity at the b values of b and 0, respectively, D and D* are the diffusion coefficient related to molecular diffusion and the pseudodiffusion coefficient related to microcapillary perfusion, respectively, and f is the perfusion fraction.
The standard apparent diffusion coefficient (ADC) was calculated using the conventional mono-exponential model with all b values:

The infract volume was measured according the following formula: Vol =XYZ ×0.5 (cm3), where X, Y, and Z stand for the largest extension in x-, y-, and z-axis 23 . Circular regions of interest (ROI) on SPECT and MRI parametric maps, measuring 30 mm in diameter, were placed in the cerebellar hemispheres ipsilesional (I) and contralateral (C) to the hemispheric stroke. All ROIs were carefully placed to avoid the major vessels and the cerebellar vermis. To evaluate the inter-reader reproducibility, these ROIs were drawn by two experienced neuroradiologists both with 5 years of experience. A CBF SPECT asymmetry index (AI SPECT ) was calculated by using the following equation:

The presence of CCD was defined as AI SPECT ≥10% 24 . AIs were also calculated for mean f, D*, and CBF ASL in all subjects according to:



Statistical analysis
All data were expressed as mean±standard deviation (SD). Statistical analysis was performed using SPSS 20.0 (SPSS, Chicago, IL, USA). Patients were divided into CCD-positive and CCD-negative groups according to their AISPECT. Descriptive data from CCD-positive and CCD-negative groups were analyzed using either the Mann-Whitney U test or the Fisher exact test as appropriate. Paired t test was applied to compare IVIM-derived parameters (ADC, D, D*, and f) and SPECT-/ASL-derived parameters (CBF) between the ipsilesional cerebellum and the contralateral cerebellum, respectively. To explore the relationships among CBF SPECT , CBF ASL , IVIM parameters, and clinical data, Pearson’s correlation analysis was applied. Diagnostic performance (sensitivity, specificity, positive likelihood ratio (+LR), and negative likelihood ratio (-LR)) of IVIM parameters in CCD diagnosis was done by using receiver operating characteristics (ROC) curve analysis. Statistical significance was defined as p < 0.05, p < 0.01 (two tailed).
Results
Among all 39 eligible patients enrolled in this study, 13 (33.3%) exhibited CCD based on their SPECT results, the standard reference. As shown in Table 1, no significant difference in age or sex distribution was observed between CCD-positive and CCD-negative groups (both p > 0.01). However, the admission NIHSS score and infarct volume in the CCD-positive group were significantly higher than those in the CCD-negative group (p = 0.02 and p = 0.042, respectively). The NIHSS score was significantly lower at discharge than at admission in the CCD-negative group (p = 0.021), whereas no significant difference was found between the admission and discharge NIHSS scores in the CCD-positive group (p = 0.724). In the CCD-positive group (n = 13), infarcts were located in the gray matter in eight (61.5%), the white matter in five (38.5%), and the thalamus in zero (0%) patients. We also found that patients with lesions in the gray matter were more likely to suffer CCD (p = 0.005) (Table 1).
Comparison of characteristics between CCD (+) and CCD (-) subjects.

CCD: crossed cerebellar diaschisis; NIHSS: National Institutes of Health Stroke Scale.
Values are mean ± standard deviation or number of patients.
*Results indicated a significant difference (p<0.05), p values refer to the Mann-Whitney U test, Fisher’s exact test as appropriate.
aNot significantly different (p=0.724) between admission and discharge NIHSS score in the CCD (+) group.
bSignificantly different (p=0.021) between admission and discharge NIHSS score in the CCD (-) group.
Figure 1 shows the images of diffusion weighted image (DWI) (b = 1000 sec/mm2) (a), SPECT (b, c), ASL (d), and maps of IVIM parameters ADC (e), D (f), D* (g), f (h) of representative patients with supratentorial stroke in the left parietal lobe for 10 days. Paired t tests were used to compare the average values of these parameters between ipsilesional and contralateral cerebellums in CCD-positive and CCD-negative groups, respectively. As shown in Tables 2 and 3, D*, CBF ASL , and CBF SPECT of the contralateral cerebellum were significantly lower than those of the ipsilesional cerebellum in the CCD-positive group (p = 0.0001, p < 0.0001 and p < 0.0001, respectively), whereas f was significantly higher (p = 0.001),and no statistical difference was observed in D and ADC (p = 0.53 and p = 0.30, respectively). In the CCD-negative group, all IVIM parameters did not significantly differ between the contralateral and the ipsilesional cerebellums (p > 0.05).
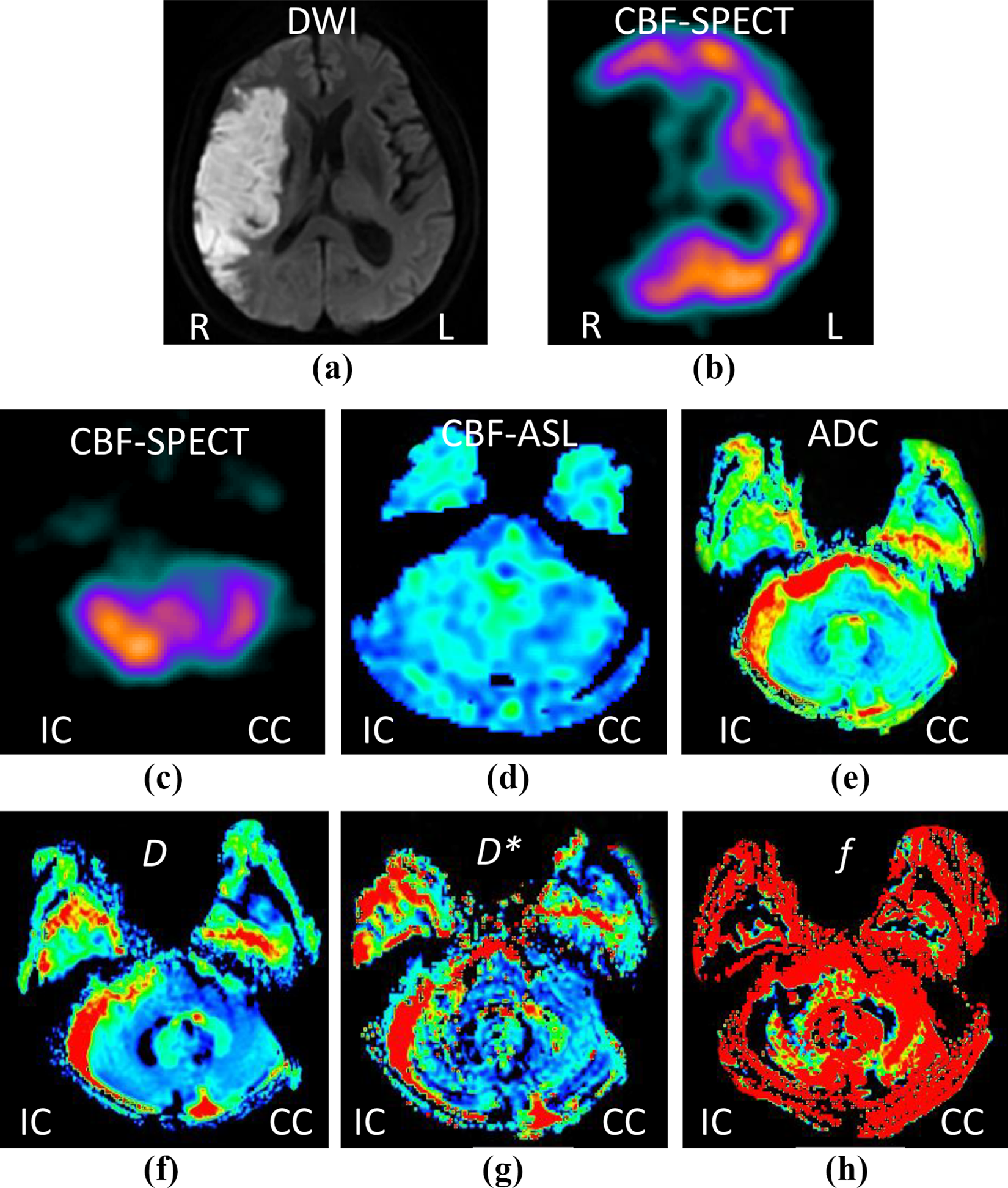
A 65-year-old man with supratentorial stoke in the right parietal for 10 days: hyperintensity stroke lesion can be recognized on the diffusion weighted image (DWI) (b = 1000 sec/mm2) (a). SPECT maps show hypoperfusion in the same lesion (b). SPECT maps (c) and ASL imaging (d) show hypoperfusion in the contralateral cerebellum. The IVIM-derived ADC (e) and D (f) maps have no change between the ipsilesional cerebellum and the contralateral cerebellum, whereas D* (g) and f (h) values show a difference in the ipsilesional cerebellum compared with those in the contralateral hemisphere. CCD: crossed cerebellar diaschisis; CBF: cerebral blood flow; SPECT: single-photon emission computed tomography; ASL: arterial spin-labeling MR imaging; IC: ipsilateral cerebellum; CC: contralateral cerebellum; ADC: the apparent diffusion coefficient; D: slow diffusion coefficient; D*: fast diffusion coefficient; f: vascular volume fraction.
Comparison of different parameters in bilateral cerebellum.

CCD: crossed cerebellar diaschisis; CBF: cerebral blood flow; SPECT: single-photon emission computed tomography; ASL: arterial spin-labeling magnetic resonance imaging; IC: ipsilateral cerebellum; CC: contralateral cerebellum; ADC: the apparent diffusion coefficient; D: slow diffusion coefficient; D*: fast diffusion coefficient; f, vascular volume fraction.
Values are mean ± standard deviation. *Results indicate a significant difference (p < 0.01).
D* and AI D* parameters in stroke patients.

CCD: crossed cerebellar diaschisis; IC: ipsilateral cerebellum; CC: contralateral cerebellum; D*: fast diffusion coefficient; AI: asymmetry index.
The results of Pearson’s correlation analysis are presented in Table 4. Although no significant correlation was detected between D* and CBF SPECT or between D* and CBF ASL , there were positive correlations between AI D* and AISPECT, as well as between AI D* and AIASL(r = 0.48, p = 0.002; r = 0.502, p = 0.001, respectively) (Figure 2). The AI f value had a negative correlation with both AI SPECT and AI ASL (r = -0.325, p = 0.04; r = -0.347, p = 0.03, respectively). The area under the ROC curve value of AI D* for CCD diagnosis was 0.923 (Figure 3). The sensitivity, specificity, +LR, and -LR values of AI D* in CCD diagnosis were 84.6%, 92.3%, 10.9, and 0.16 respectively, at the optimal cut-off value of 8.54%.
The results of Pearson’s correlation between various parameters.

AI: asymmetry index. CBF: cerebral blood flow; SPECT: single-photon emission computed tomography; ASL: arterial spin-labeling magnetic resonance imaging; D*, fast diffusion coefficient; f, vascular volume fraction.
Values are mean ± standard deviation. *Results indicate a significant difference (p < 0.05).
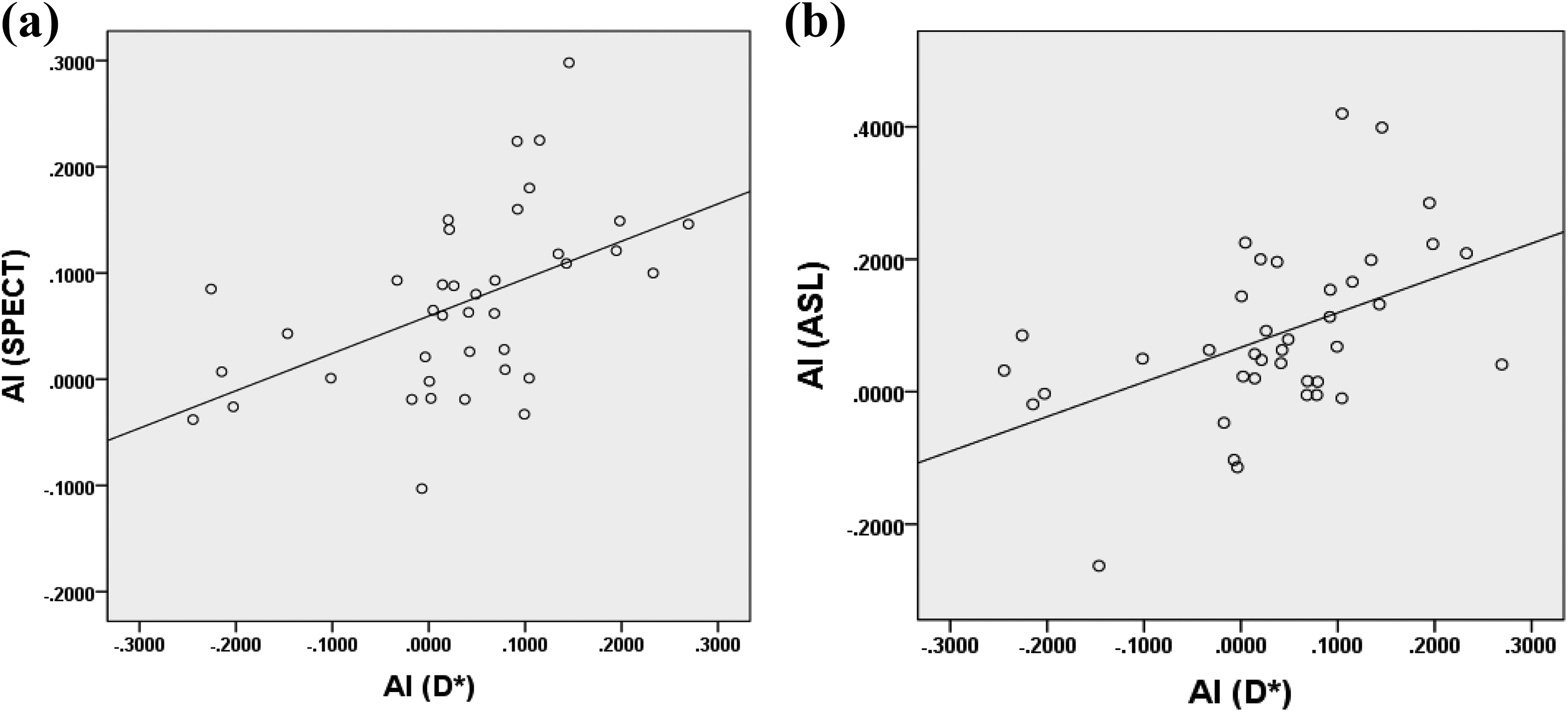
The scatter plot for the relationships between AI D* and AI SPECT (a) (r = 0.48, p = 0.002) and between AI D* and AI ASL (B) (r = 0.502, p = 0.001). AI: asymmetry index; SPECT: single-photon emission computed tomography; ASL: arterial spin-labeling magnetic resonance imaging; D*: fast diffusion coefficient.

Receiver operating characteristic (ROC) curves for AI D* in patients based on AI SPECT . AI: asymmetry index; SPECT: single-photon emission computed tomography; D*= fast diffusion coefficient.
Discussion
In the present study, we evaluated whether IVIM could predict CCD in patients with supratentorial stroke. We found that D* was decreased in the contralateral cerebellum compared with in the ipsilesional cerebellum in CCD-positive cases. Furthermore, we determined the optimal cutoff value for AI D* and analyzed its reliability in CCD detection.
According to recent literature on CCD, decreased blood flow and metabolism were more commonly observed in the contralateral cerebellum compared with the ipsilesional side using PET and SPECT methods 9,25 . Although these imaging methods have enhanced our understanding of CCD, the requirement of radioactive tracers and lack of spatial resolution limit their application in the clinical setting. With the development of MR perfusion techniques, several studies have been carried out to detect CCD by noninvasive MRI. ASL takes endogenous arterial water as a diffusible tracer, which enables us to estimate brain perfusion frequently over a long-term follow-up period 4 . A previous study indicated that ASL could identify CCD by using asymmetric CBF ASL 26 .
As a new contrast-free imaging method, IVIM could separate microcirculation or perfusion effects from true diffusion by applying DWI obtained with multiple b values and a bi-exponential model. It has been proven that IVIM can monitor the change in cerebral blood flow in a gradual way after the vasodilation or vasoconstriction induced by CO2 and O2 17 . In stroke cases, IVIM analysis showed a significant reduction in D, D*, and f values in lesions compared with the contralateral side 20 . In our previous study, we successfully assessed the tissue diffusion and perfusion parameters simultaneously in ischemic stroke patients by using IVIM-MRI 27 . The studies mentioned above implied it was feasible to measure the perfusion of brain tissue by IVIM.
In our present study, IVIM imaging was applied to detect CCD, which has rarely been reported in previous studies. In CCD-positive cases,patients had lower D* and higher f values in contralateral cerebellum compared with those in the ipsilesional cerebellum, but no significant difference was observed in ADC or D, which implied the CCD was related to changes of the microvascular perfusion but not tissue microstructure indicated by diffusivity. This finding is consistent with the results reported by Meyer et al., revealing that CCD was directly related to the loss of afferent stimuli from the supratentorial cortex, but not structural change in animal models 28 . Similarly, in another previous study, a reduction in perfusion-related CBF value was observed in the contralateral cerebellum of CCD-positive stroke patients using contrast-based imaging modalities 12 . Although D* did not have a direct correlation with CBF SPECT and CBF ASL , AI D* was found to have a positive correlation with AI SPECT and AI ASL in our study. A significant positive correlation was also observed between D* and CBF ASL in both tumor and white matter by Lin et al 18 . Therefore, D* derived from the IVIM model can reflect cerebral perfusion and may be an alternative parameter in the assessment of CCD in stroke.
Theoretically, the volume fraction of the rapid diffusion component, the f value, is expected to be lower in the contralateral cerebellum of CCD. Interestingly, we observed a higher f value in the contralateral cerebellum of the CCD-positive group, which is inconsistent with the reported hypoperfusion, such as reduced perfusion in the contralateral cerebellum of patients with CCD 10,29 , using other imaging techniques. According to previous studies, two facts might explain this phenomenon: different choices of b values and times of echo (TE). A lower b value contributes to the pseudodiffusion component 30 . Thus, the b values might be important for calculating the f value accurately. Lemke et al. demonstrated that f was influenced by TE; the longer the TE, the greater the signal attenuation at low b values and the higher the f value 31 . On top of that, cautious interpretation of f in supratentorial stroke with CCD is needed, as f itself might not purely reflect capillary blood flow within each voxel 32 . Moreover, we also found the AI f value has a negative correlation with AI SPECT and AI ASL, respectively. Therefore, further studies are needed to investigate this in more detail. IVIM can provide both diffusion and perfusion imaging information, which has the advantage of providing more opportunities to further explore the clinical value of IVIM in the brain. Furthermore, as a radiation and contrast-free method, IVIM could be more beneficial to patients than other imaging methods.
The incidence of CCD in our clinical subjects was 33.3% using SPECT, whereas various values were reported by other studies using different imaging methods: 15.61% using dynamic susceptibility contrast MRI 12 , 31% using CT perfusion 33 , 39.8% using SPECT 24 , 52% using ASL MRI 14 , and 89% using PET 34 . Such differences could be attributed to multiple factors, such as the median time interval from onset to image acquisition, the differences in patient selection criteria, and the imaging principles. In our study, the infarct volume was significantly larger and the admission NIHSS score was significantly higher in the CCD-positive than in the CCD-negative group. Meanwhile, the NIHSS score decreased significantly in the CCD-negative group at discharge, but there was no significant difference between admission and discharge NIHSS scores in the CCD-positive group. These results demonstrated the NIHSS score and infarct volume were closely related to being CCD positive, and that patients with CCD may have a worse outcome than those without CCD in subacute stroke. Previously, a PET study on CCD detecting reported the volume of supratentorial infarct volume played a significant role in CCD development 35 . Shinohara et al. proved that the asymmetry index of the contralateral cerebellar hemisphere was significantly correlated with NIHSS score using 3D ASL 29 .
As for the location of lesions in our study, CCD was found to be more frequent in patients with infarcts in the gray matter. Meanwhile, Forster et al. indicated that CCD was a frequent phenomenon in acute thalamic infarct 36 . However, some other studies suggested that lesions in other locations such as the frontal lobe and the temporal lobe could contribute to the occurrence of CCD 37,38 . The discrepancies may be explained by factors such as the number of cases or classification method and so on.
Conclusion
In this study, for the first time we demonstrated that CCD could be diagnosed with IVIM by a decreased D* value in the contralateral cerebellum compared with that in the ipsilesional side. Furthermore, we report that AI D* has a statistically significant correlation with AI ASL and AI SPECT, respectively. Consequently, as a noninvasive quantitative MRI method, IVIM could obtain perfusion characteristics and might be a novel method of assessing supratentorial stroke with CCD. Based on the findings above, IVIM could be a novel valuable imaging technique in detecting CCD with the advantage in predicting outcome of patients with CCD.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved from the hospital insititutional research ethics board.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this work was supported by the Foundation of Renji Hospital South Campus, Shanghai Jiao Tong University School of Medicine. (Nos 2017PYQB04, 2016PWGY02); Shanghai Municipal Natural Science Foundation (16ZR1420700); Medical Guidance Project from Shanghai Science and Technology Committee (19411971200).
Statement of Human and Animal Rights
The whole study followed apporval from the hospital insititutional research ethics board, and all subjects have written informed consent.
Statement of Informed Consent
All subjects have written informed consent.