
Abstract
Crossed cerebellar diaschisis (CCD) is well described in the chronic phase of stroke, but few data describe acute CCD and its serial changes after reperfusion. Using positron emission tomography (PET), we studied acute CCD with respect to supratentorial perfusion and outcome measures. In 19 acute stroke patients receiving intravenous thrombolysis (<3 h), 15O-water PET assessed CCD and supratentorial hypoperfusion volume before thrombolysis, 3, 24 h and 14 days later. Infarct volume at day 14 and NIHSS score at 3 months were assessed. Supratentorial hypoperfusion decreased from 25 cm3 (median) before thrombolysis to 0.1 cm3 at day 14. Baseline CCD was 13.4% and decreased continuously to 6.1% after 14 days. The NIHSS score decreased from 11 to 4 pts after 3 months. Infarct volume was 1.1 cm3. Crossed cerebellar diaschisis correlated to the hypoperfusion volume within the first 24 h after stroke, but not later. Hypoperfusion correlated to outcome measures at the early stage only. In contrast, CCD correlated to outcome values at all four measurements. Reperfusion with recovery of CCD was seen in patients with small infarcts and good clinical outcome and vice versa. Our data suggest that (i) CCD occurs as early as 3 h after stroke and might be reversible; (ii) acute CCD is closely related to the volume of supratentorial hypoperfusion. At later time points, however, CCD is disconnected from supratentorial perfusion but strongly associated to outcome measures; (iii) CCD is not susceptible to nonnutritional reperfusion and adds valuable information to interpret supratentorial reperfusion patterns.
Introduction
‘Crossed cerebellar diaschisis’ (CCD) refers to an asymmetry of blood flow or metabolism in the cerebellar hemispheres contralateral to a remote supratentorial lesion (Baron et al, 1980; Feeney and Baron, 1986). The interruption of corticoponto-cerebellar pathways causes a remote functional deactivation by a reduced excitatory input and a decreased cerebellar blood flow (Gold and Lauritzen, 2002). Using single-photon emission computed tomography (SPECT) and positron emission tomography (PET), the degree, localization and size of cerebral hypoperfusion have been related to the presence and degree of CCD with controversial results (Flores et al, 1995; Infeld et al, 1995; Kim et al, 1997; Pantano et al, 1987; Martin and Raichle, 1983). In studies of stroke patients without thrombolytic treatment, CCD was generally considered a persistent phenomenon (Baron et al, 1980; Kamouchi et al, 1996; Lenzi et al, 1982; Pantano et al, 1986, 1987; Serrati et al, 1994; Meneghetti et al, 1984), even despite clinical recovery (Infeld et al, 1995). Under certain conditions, however, a remission of CCD was reported: in patients with internal carotid artery occlusion after extra-intracranial bypass surgery (Pantano et al, 1987), in patients with small infarcts (Lenzi et al, 1982; Miura et al, 1994), in transient ischemic attacks (Pantano et al, 1987; Perani et al, 1987) and in cases of temporary balloon occlusion (Brunberg et al, 1992).
Considering that CCD reflects a potentially reversible functional inactivation (Gold and Lauritzen, 2002), the serial changes after supratentorial reperfusion by thrombolysis (Heiss et al, 1998) are of major interest. Our study was therefore designed (i) to detect hyperacute CCD in human middle cerebral artery (MCA) stroke; (ii) to describe the time-dependent changes after thrombolysis and its association to supratentorial perfusion and (iii) to investigate its relation to outcome parameters.
Materials and methods
Patients
Nineteen patients (8 women; mean age 67 ± 7 years) with first-ever unilateral MCA stroke (10 left MCA) were selected for our study. After informed consent, thrombolysis was initiated within 3 h after symptom onset as previously described (Heiss et al, 1998). The average time interval between symptom onset and thrombolysis was 112 mins (± 34; range: 35 to 175 mins). The clinical status was assessed by the National Institute of Health Stroke Scale (NIHSS) at the time of admission (NIHSS0), 24 h later (NIHSS24 h) and 3 months later (NIHSS3mo).
Positron Emission Tomography Imaging
Positron emission tomography studies of cerebral blood flow (CBF) were performed in resting state on an ECAT EXACT or EXACT HR scanner (Siemens/CTI, Knoxville, TN, USA) as previously described (Heiss et al, 1998). Data reconstruction provided 47 contiguous 3-mm slices of 5 mm full-width at half-maximum in-plane reconstructed resolution. Cerebral blood flow measurements were obtained with 15O-water according to the intravenous bolus method. Scan duration was 120 secs with 60 mCi (2.2 Gbq) per scan. Each patient received four consecutive PET scans: before thrombolysis, that is, within 3 h after symptom onset; 3 h, 24 h and 14 days after thrombolysis. A total of 73 PET scans were performed in 19 patients.
Data Acquisition and Analysis
The four sequential CBF images per patient were coregistrated by a software previously described (Pietrzyk et al, 1994). For CCD measurement, a representative transaxial slice showing the highest degree of asymmetry was chosen. A circular region of interest (ROI) of 30 mm diameter was placed in the cerebellar hemisphere ipsilateral to the ischemic MCA territory and then mirrored to the contralateral cerebellar hemisphere (Figure 1, lower row). Crossed cerebellar diaschisis was expressed as an asymmetry index: CCD = [(I—C)/I]*100 (C is the mean value of the cerebellar hemisphere contralateral, I is the mean value of the cerebellar hemisphere ipsilateral to the stroke). The ROI pair was copied on the co-registered follow-up PET scans. Higher positive values represented a marked diaschisis and vice versa. For supratentorial hypoperfusion asymmetry (HYPOAI), the area of hypoperfusion was outlined on a representative transaxial slice (Figure 1, upper row), copied to the unaffected hemisphere and expressed as an asymmetry index. The supratentorial hypoperfusion volume (HYPOVOL) was defined by the volume of CBF below 20 mL/100 g min−1 on PET images assessed by relative CBF values lower than 70% of the mean value of the unaffected hemisphere as previously described (Thiel et al, 2001). The volume was measured as Vol = XYZ × 0.5 (cm3), where X, Y and Z stand for the largest extension in x-, y- and z-axis (van der Worp et al, 2001) (Figure 1, middle row). Likewise, the final infarct volume (INF) was defined on the follow-up CT scans after 14 days. Study data thus included four values for CCD, HYPOAI and HYPOVOL, three values for NIHSS and one value for INF per patient.
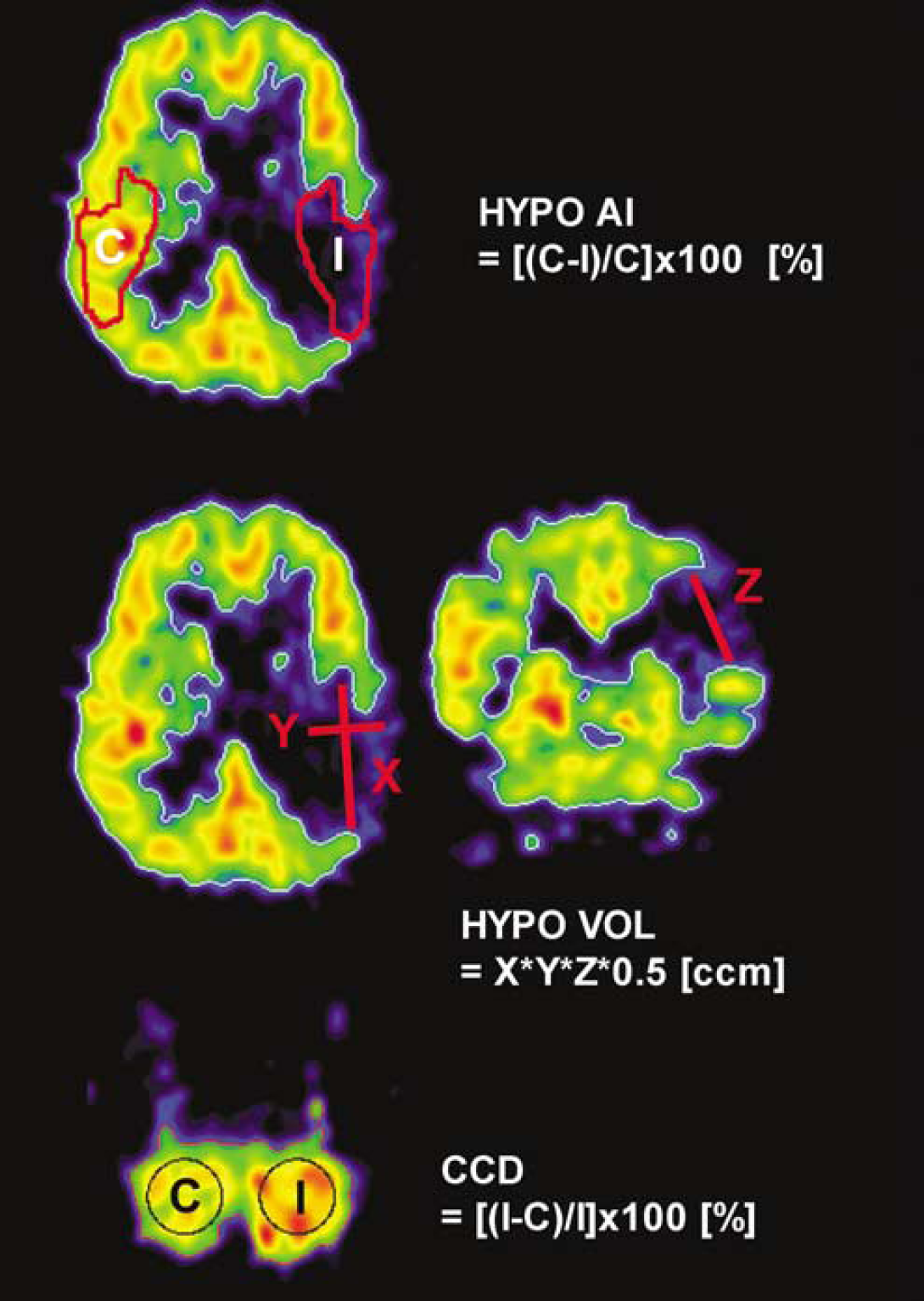
Assessment of supratentorial hypoperfusion asymmetry (HYPOAI, upper row), hypoperfusion volume (HYPOVOL, middle row) and cerebellar perfusion asymmetry (CCD, lower row). For details, see Materials and methods section.
Statistics
Due to the skewed distribution (all data except CCD values), a nonparametric approach was applied. Data are given as median and interquartile range (25th and 75th percentiles). Spearman's rho was used for correlation analysis. Differences along the four measurements were assessed by an ANOVA on ranks (Dunn's method). Serial CCD changes were tested by an ANOVA (Dunett's method). Data analysis was performed with SAS Version 6.11 for Unix (Statistical Analytic System, SAS Institute Inc.) and Sigmastat 3.00 (SPSS Inc. 2003). The threshold of significance was set to P < 0.05 for all analyses.
Results
For all 19 patients (Table 1), the median supratentorial hypoperfusion volume (HYPOVOL) decreased from 25 cm3 before thrombolysis to 0.1 cm3 14 days after thrombolysis. Supratentorial hypoperfusion asymmetry before thrombolysis was 40.4% and decreased to 4.9% at day 14. The median CCD value before thrombolysis was 13.4% and decreased continuously to 6.1% along the four measurements. For CCD and supratentorial hypoperfusion, the changes were significant between 0 and 24 h and between 0 h and 14 days (P < 0.029 for CCD, P < 0.001 for HYPOVOL). The changes between 0 and 3 h were not significant. The median NIHSS value at baseline was 11 pts and decreased significantly to 4 pts after 24 h and to 1 pt after three months. Median infarct volume at day 14 was 1.1 cm3 (range 0 to 165). Six of 19 patients had no infarct on their follow-up CT.
Study data of all 19 patients
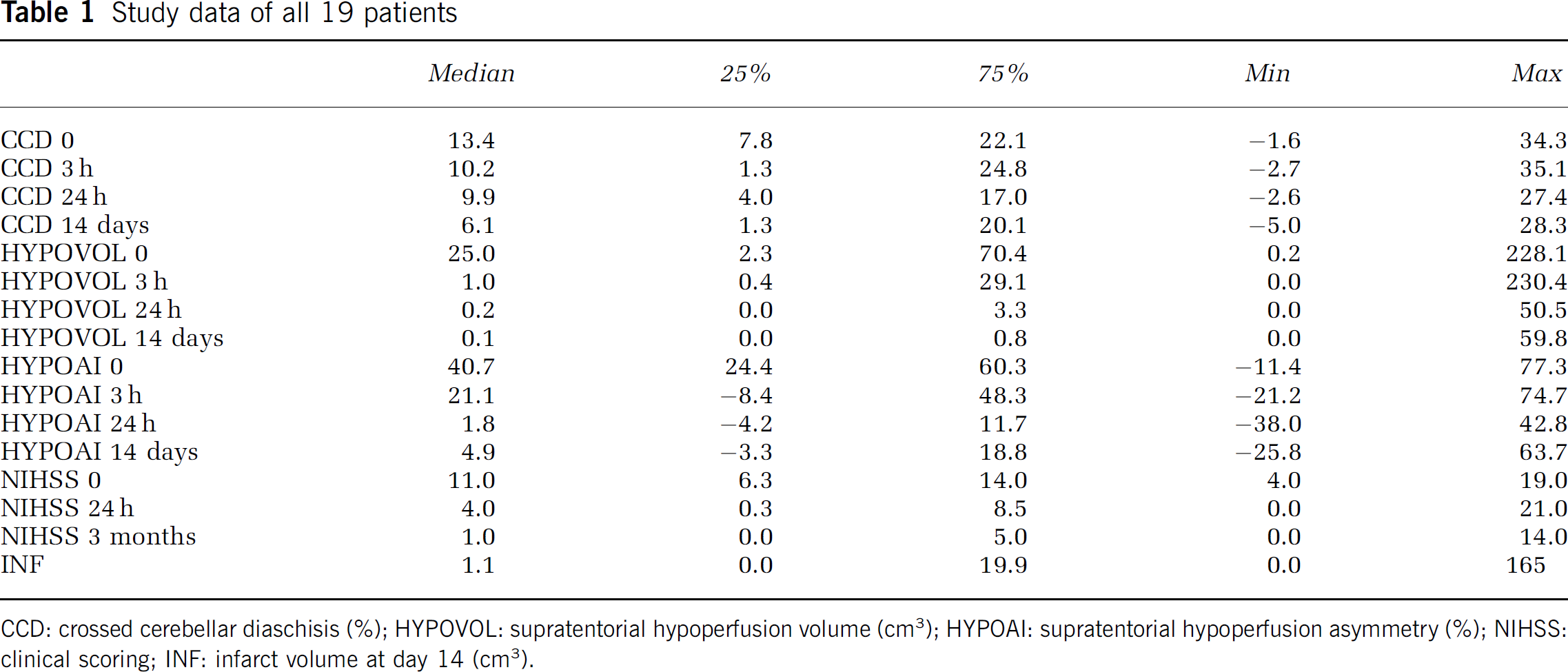
CCD: crossed cerebellar diaschisis (%); HYPOVOL: supratentorial hypoperfusion volume (cm3); HYPOAI: supratentorial hypoperfusion asymmetry (%); NIHSS: clinical scoring; INF: infarct volume at day 14 (cm3).
Crossed Cerebellar Diaschisis, Supratentorial Perfusion and Clinical Scoring
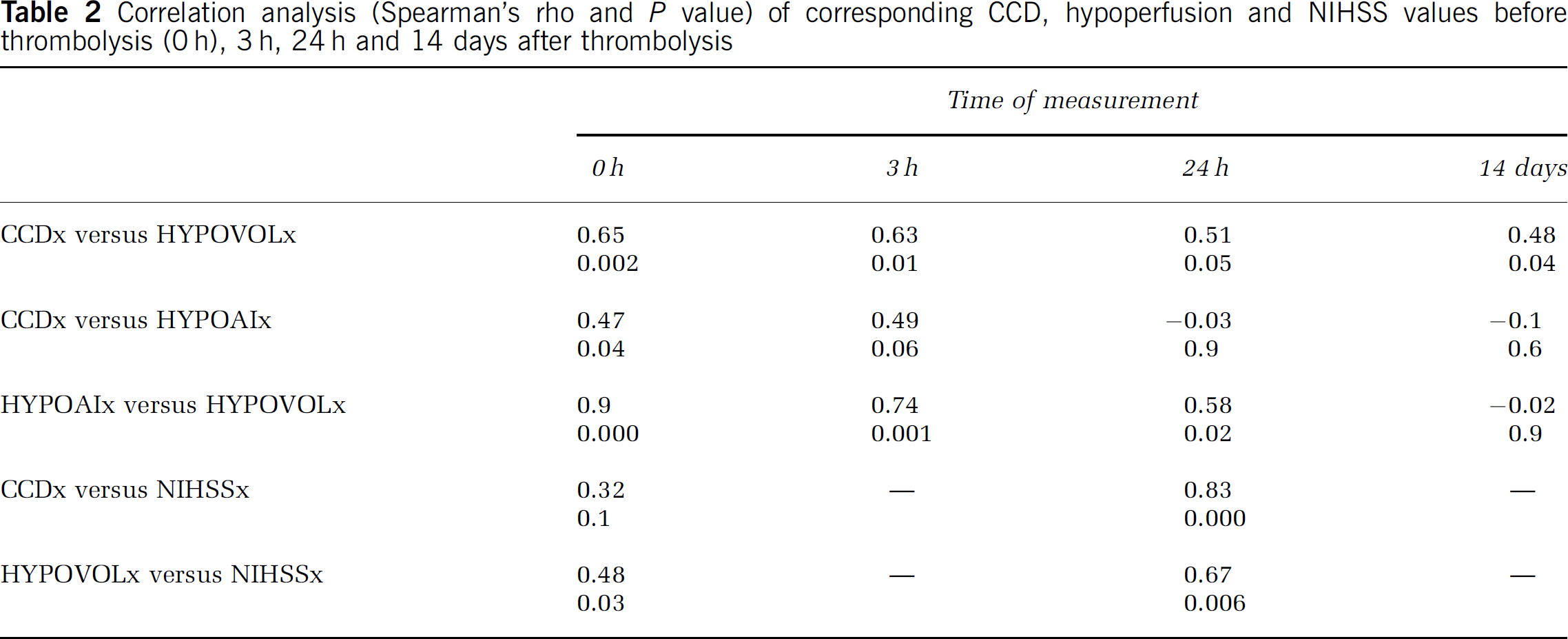
The volume of supratentorial hypoperfusion correlated with the corresponding CCD values (HYPOVOL versus CCD) before and 3 h after thrombolysis, but not in the later measurements (Table 2). The severity of supratentorial hypoperfusion (HYPOAI) was not significantly correlated to CCD at any time point.
Correlation analysis (Spearman's rho and P value) of corresponding CCD, hypoperfusion and NIHSS values before thrombolysis (0 h), 3 h, 24 h and 14 days after thrombolysis
Crossed Cerebellar Diaschisis, Supratentorial Perfusion and Outcome Scores
Within 3 h after stroke, the supratentorial hypoperfusion volume correlated significantly to infarct volume and to NIHSS score at 3 months (Table 3). In the following measurements, this association decreased continuously. The CCD values, in contrast, correlated strongly to infarct volume and clinical outcome at all four measurements.
Correlation analysis (Spearman's rho and P value) of CCD values (CCD) and supratentorial hypoperfusion volume (HYPOVOL), assessed at different time points, with outcome measures
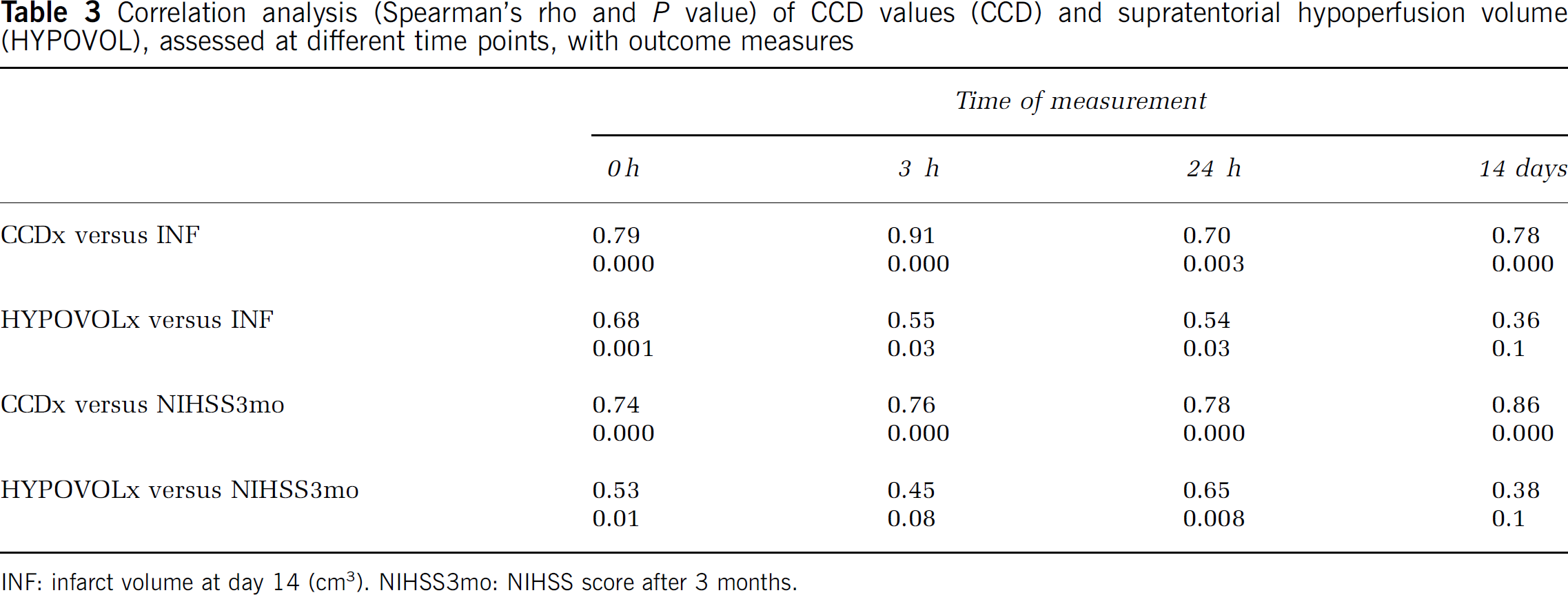
INF: infarct volume at day 14 (cm3). NIHSS3mo: NIHSS score after 3 months.
Reperfusion Patterns
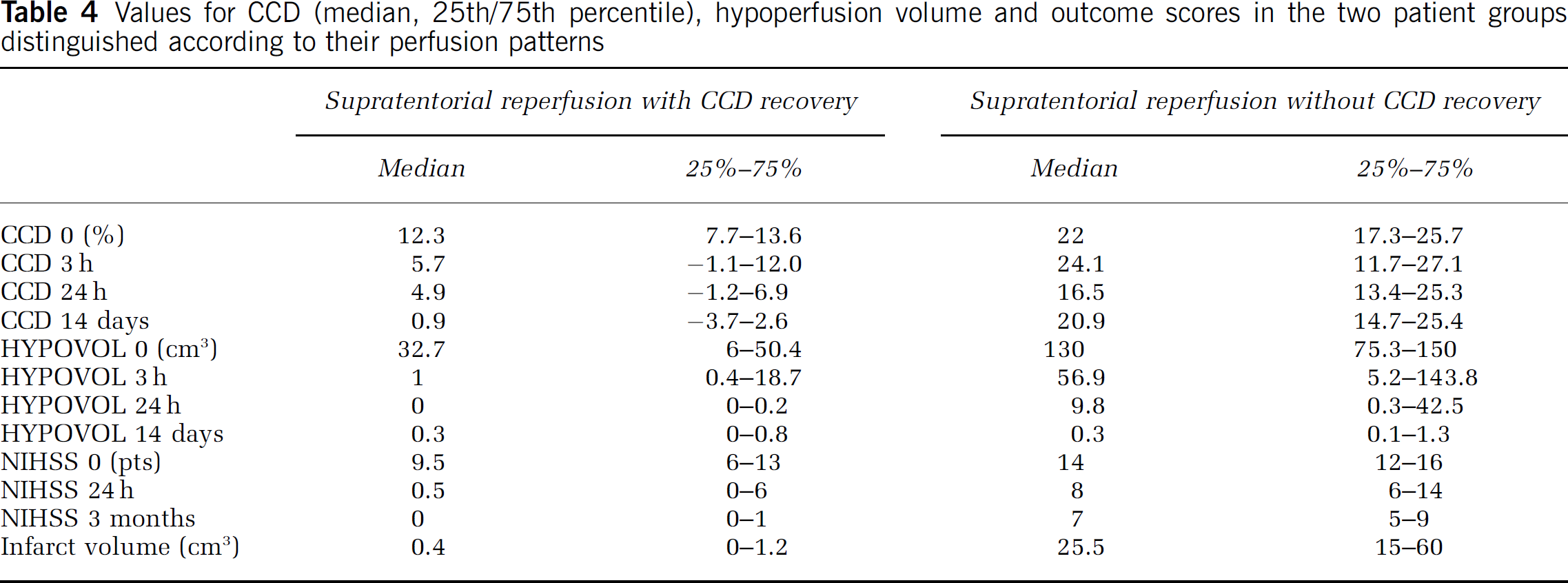
To define CCD changes with respect to supratentorial reperfusion, we identified 13 out of 19 patients with a relevant hypoperfusion volume (i.e. HYPOVOL >5 cm3). Out of these 13 patients, 12 showed a substantial reperfusion (i.e. >90% reduction of the initial hypoperfusion volume at day 14). The patients were then subdivided according to their CCD response (Table 4): if reperfusion was accompanied by decreasing CCD values (CCD reduction ≥50% between baseline and day 14; n = 6), the final infarct was small and outcome at three months was favorable. Reperfusion with persistent CCD or incomplete recovery of CCD (CCD reduction less than 50%; n = 6) resulted in large infarcts and poor outcome at three months. Figure 2 illustrates these findings in two representative cases. In one of the 13 patients, reperfusion was seen 3 h after thrombolysis, but infarct at day 14 exceeded initial hypoperfusion. In this case initial CCD values were high, persisted despite early reperfusion and indicated poor outcome (Figure 3). Six of 19 patients were not included in this analysis, since they showed no relevant initial hypoperfusion volume (median 1.1 cm3).
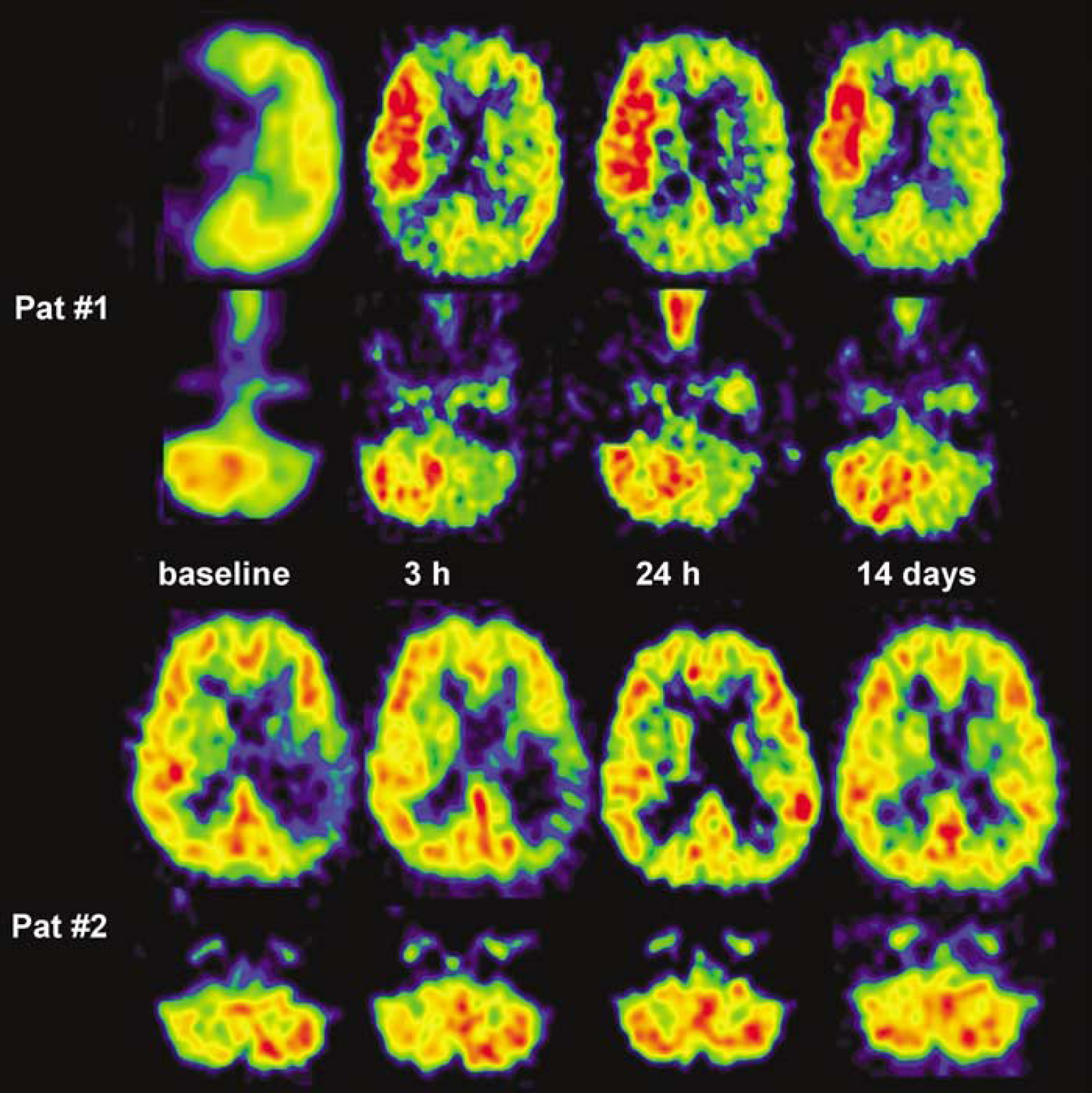
Reperfusion with different responses of CCD. In patient #1, CCD persisted despite a marked supratentorial reperfusion/hyperperfusion. Infarct volume was 60 cm3, clinical outcome was poor (NIHSS 9 pts). In patient #2, supratentorial reperfusion was accompanied by a CCD decrease. Follow-up CT showed no infarct, outcome NIHSS score was 0 pt.
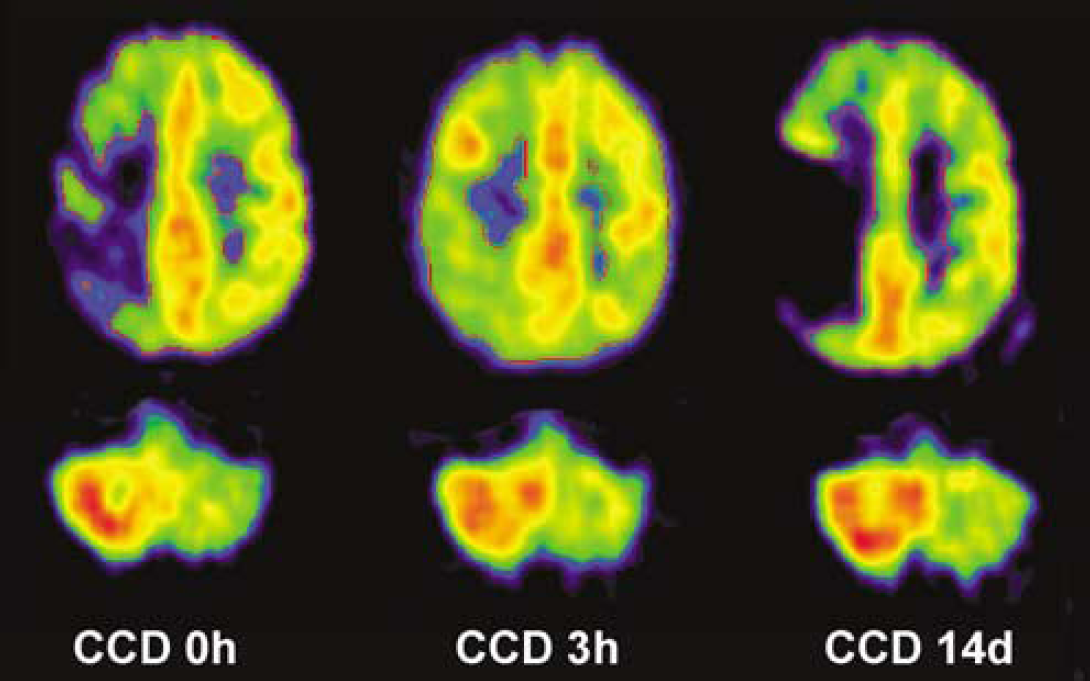
After initial reperfusion (from 13.9 to 1.0 cm3), hypoperfusion at day 14 (26.6 cm3) exceeded initial hypoperfusion. CDD values were high before thrombolysis and persisted (27.1%, 30.3% and 26.6%) despite initial reperfusion. Final infarct was 58 cm3 and clinical outcome was poor (NIHSS 14 pts).
Values for CCD (median, 25th/75th percentile), hypoperfusion volume and outcome scores in the two patient groups distinguished according to their perfusion patterns
Discussion
Our study described serial changes of acute CCD with respect to supratentorial perfusion and outcome parameters. We present the first PET data of serial CCD changes after intravenous thrombolysis within a 3-h time window. Crossed cerebellar diaschisis occurred as early as 3 h after stroke and recovered over time. In the first hours after stroke, CCD was closely related to the volume of supratentorial hypoperfusion. At later time points, however, CCD was disconnected from supratentorial perfusion but strongly associated to outcome parameters.
The present study has to be interpreted with respect to two characteristic features: the rigorous chronology of the PET scans and the restriction to a vascular territory: We have shown that the time interval from stroke onset is critical to assess the dynamic character of diaschisis after stroke even within the first 24 h. Most of the previous reports clustered CCD values from several days (Infeld et al, 1995; Kamouchi et al, 1996; Laloux et al, 1995; Meneghetti et al, 1984; Serrati et al, 1994) to several weeks and more (Baron et al, 1980; De Reuck et al, 1997; Kim et al, 1997; Pantano et al, 1986, 1987) and therefore summarized different stages of CCD. The strokes we investigated were restricted to the MCA territory. With few exceptions (Infeld et al, 1995; Kamouchi et al, 2004; Serrati et al, 1994; Takasawa et al, 2002), previous reports included strokes from various vascular territories (Baron et al, 1980; Bowler et al, 1995; Kamouchi et al, 1996; Kim et al, 1997; Laloux et al, 1995; Lenzi et al, 1982; Martin and Raichle, 1983), which may disperse the obtained results.
The reversibility of CCD under thrombolytic therapy reflects the functional and initially reversible character of cerebellar flow asymmetry. This finding contrasts with previous studies without reperfusion that considered CCD a persistent phenomenon (Baron et al, 1980; Bowler et al, 1995; Infeld et al, 1995; Meneghetti et al, 1984; Serrati et al, 1994; Takasawa et al, 2002). Most of these studies were performed in the subacute or chronic stage. Thus, the detection of CCD changes was compromised by either a late measurement, or—if measured early (Infeld et al, 1995; Kamouchi et al, 2004; Serrati et al, 1994)—by the lack of supratentorial flow improvement within a critical time window. Only one SPECT study used a comparable design performing thrombolysis and found a recovery of CCD in 4 of 8 patients measured within 6 h after stroke, but did not provide quantitative data (Sperling et al, 1995).
The median CCD value before thrombolysis was 13.4% in our study, which represents the first extensive PET data within 3 h in human stroke. The rapid cerebellar response, which was not observed in some earlier studies (Hossmann et al, 1985), is in line with the current pathophysiogical concept (Gold and Lauritzen, 2002) and our findings add to previous studies that described acute CCD (Kamouchi et al, 2004; Sperling et al, 1995). The most pronounced CCD changes were seen within 24 h after stroke since CCD values decreased significantly to 9.9%.
Within 3 h after stroke, the CCD values correlated to the corresponding volume of supratentorial hypoperfusion, but not to the degree of supratentorial flow asymmetry. The main determinant of CCD was therefore the number of functionally impaired neurons and the resulting interruption of the cortico-ponto-cerebellar pathway, not the severity of the ischemic damage. This supports previous studies in which distinct thalamic infarctions without affecting the internal capsule did not cause CCD (Szelies et al, 1991). Due to the limited patient number, we did not correct for different localizations within the MCA territory since our study focused on a longitudinal analysis of patients. However, a more pronounced CCD with hypoperfusion of the anterior MCA territory has to be postulated according to the literature.
The association of CCD and hypoperfusion volume was time-dependent and diminished along the follow-up measurements. This ‘disconnection’ suggests that CCD is not a simple mirror of supratentorial perfusion but contains additional information: we found that the supratentorial hypoperfusion before thrombolysis correlated to outcome measures. With increasing time from stroke onset, however, this association became weaker and was lost after 14 days. The CCD values, in contrast, were strongly correlated to outcome measures at all four measurements. Two patterns of reperfusion were therefore distinguished with respect to CCD development: when reperfusion met viable tissue (nutritional reperfusion), small or absent infarct volumes and a good clinical outcome were observed. In these cases, CCD was moderate and was reversible over time. In contrast, the reperfusion of irreversibly damaged tissue (nonnutritional reperfusion) resulted in large infarction and poor outcome, although reperfusion (or hyperperfusion) was observed. In these cases, CCD was pronounced and recovery was incomplete or absent.
The finding that CCD is reversible and is not susceptible to nonnutritional reperfusion has not yet been issued in a larger series of patients. However, it provides the clinical counterpart of a recently published animal model of CCD. Gold and Lauritzen (2002) found an immediate and severe decrease of contralateral Purkinje cell spiking activity and blood flow due to a functional neocortical lesion. After recovery of neocortical function, cerebellar blood flow was restored. The authors concluded that an irreversible neuronal damage is not necessary to produce CCD. Our data equally confirm that a functional neocortical impairment is sufficient to cause CCD in humans within the first hours after stroke: CCD was not only seen in patients with final infarcts but also in patients with initial hypoperfusion that recovered without morphologic sequelae. This finding corresponds to previous reports on transient ischemic episodes (Brunberg et al, 1992; Pantano et al, 1987; Perani et al, 1987). In the acute phase, CCD therefore indicates impaired tissue function due to penumbral flow (defined by CBF values below 20 mL/100 g min−1). Later than 24 h after stroke, however, persisting CCD becomes a surrogate marker of tissue damage, independent of cortical (re)perfusion.
In conclusion, the serial CCD changes after intravenous thrombolysis within a 3-h time window suggest that (i) CCD occurs as early as 3 h after stroke and is reversible; (ii) in the first hours after stroke, CCD is closely related to the volume of supratentorial hypoperfusion. At later time points, however, CCD is partly disconnected from supratentorial perfusion but stronger associated to outcome parameters than the volume of supratentorial hypoperfusion itself; (iii) CCD seems not susceptible to nonnutritional reperfusion and can add valuable information to interpret supratentorial reperfusion patterns.