
Abstract
The urethra is part of the lower urinary tract and its main role is urine voiding. Its complex histological structure makes urethral tissue prone to various injuries with complicated healing processes that often lead to scar formation. Urethral stricture disease can affect both men and women. The occurrence of this pathology is more common in men and thus are previous research has been mainly oriented on male urethra reconstruction. However, commonly used surgical techniques show unsatisfactory results because of complications. The new and progressively developing field of tissue engineering offers promising solutions, which could be applied in the urethral regeneration of both men´s and women´s urethras. The presented systematic review article offers an overview of the cells that have been used in urethral tissue engineering so far. Urine-derived stem cells show a great perspective in respect to urethral tissue engineering. They can be easily harvested and are a promising autologous cell source for the needs of tissue engineering techniques. The presented review also shows the importance of mechanical stimuli application on maturating tissue. Sufficient vascularization and elimination of stricture formation present the biggest challenges not only in customary surgical management but also in tissue-engineering approaches.
Introduction
Urethral strictures represent a pathologic narrowing of the urethral lumen. This pathology affects mainly men and is manifested by lower urinary tract symptoms: poor stream, hesitancy, terminal dribbling, incomplete voiding, etc 1 . Female urethral strictures are rare. Urinary tract infections, overactive bladder, and stress incontinence are common conditions affecting women´s urinary tracts 2 . Management of the female urethral strictures involves urethral dilatation and urethral reconstruction using vaginal flaps, vaginal grafts, and oral mucosal grafts 3 .
In men, iatrogenic injury is the most common cause of urethral stricture followed by idiopathy, trauma, and inflammation. Systemic diseases (e.g., lichen sclerosus) can also lead to urethral strictures. Scarring of the urethral tissue is the causative process leading to the replacement of the vascular tissue of the corpus spongiosum, which leads to ischemic spongiofibrosis of the urethra. Urethral stricture is often manifested by other complications that can be presented as recurrent or chronic infection, the formation of bladder calculi, fistulas, development of sepsis, or renal failure. Therefore, urethral strictures present a serious health condition that significantly impairs quality of life and may lead to the failure of vital organs if left untreated 4 .
It is estimated that the incidence of the urethral strictures is approximately 1% in males over the age of 55. However, the real incidence of male urethral stricture disease is unknown and strongly depends on certain populations, geography, and income 5 .
The choice of surgical technique depends on the location and length of the stricture. Approximately 50% of urethral strictures are located in the bulbar urethra, 30% in the penile urethra, with the rest in a combination of both. There is a significant interest in optimizing surgical techniques to avoid further interventions and obtain a satisfactory high long-term success rate. Urethral dilatation and direct visualization internal urethrotomy are the preferred techniques for urethral stricture management. However, the management of long urethral strictures remains challenging, as outcomes seem to be poor 6,7 . The success rate of urethroplasty techniques is between 80–90%. The outcomes of anastomotic and graft substitution urethroplasties showed a satisfactory long-term success rate.
In pioneering works, different tissues such as the buccal mucosa and free-skin grafts have been applied to treat these pathological conditions. However, both are accessible in limited quantities and their utilization is accompanied by donor site morbidity and various post-surgery complications, so alternative treatment procedures are needed to improve long-term outcomes 8,9 . Tissue engineering (TE) offers several promising approaches that may help to overcome these problems. TE, in the context of the urethral repair, uses different cell types alone or in combination with different functional biomaterials and specific growth factors to engineer functional urethral tissue suitable for transplantation purposes. Choosing the right cell type together with a supporting matrix (scaffold) is a crucial step in urethral TE 10 –12 .
So far, there have been only a few clinical studies describing the use of cell-seeded templates in urethral reconstruction. Cells isolated from the buccal mucosa and bladder tissue were applied 13 . According to our search criteria, only one article describing clinical application on in vitro cultivated cells was suitable for review.
The main goal of this article is to focus on the various types of cells involved in urethral reconstruction using approach of TE.
Materials and Methods
Literature search methodology
A search was performed (3 January 2019) of the PubMed/Medline databases. Keywords related to TE were combined with synonyms for the urethra, urethral tissue, urothelium, smooth muscle cells (SMCs), stem cells, and urethral TE. The search was restricted to the last 10 years, the English language, and studies performed on humans or animals. A Prisma Flow Diagram represents the outline of the literature search (Figure 1).

Outline of the literature search (n = 20). The database search was performed on 3 January 2019 according to the PRISMA statement. For more details see the Materials and Methods section.
Results
Urine-derived stem sells
Urine-derived stem cells (UDSCs) were the point of interest in the following studies. Either human or animal urine samples were the source of these cells. Urethral catheterization, spontaneously voided urine, bladder irrigation, and bladder washing were the methods used for urine harvesting. To collect the cells, urine samples were centrifuged. Cells were cultured in initiation media, which mainly consisted of a mixture of embryonic fibroblast (EFM) and keratinocyte serum free medium (Figure 2).

Urine-derived stem cells (UDSCs). An example of colonies from primary isolated cells (a) and confluent layer in the first passage (b). Electronogram of UDSC in third passage (c) – the cells display a flattened morphology as a result of contamination by renal epithelial cells. Representative histogram of UDSCs. Cells were positive for typical markers of mesenchymal stem cells CD-73, CD-90, CD-105, CD-271, CD-146 and lack expression of CD14, CD20, CD34, and CD45 typical for hematopoietic and endothelial cells (d).
Tayhan et al. used six fresh urine samples harvested from healthy patients via urethral catheterization. Human UDSCs and urine-derived urothelial cells were studied. Immunocytochemical analysis was performed to characterize isolated cells. Antibodies against cytokeratin 7 were used as urothelial cell markers. Antibodies against CD45 and CD90 were used to determine the presence of the mesenchymal stem cells (MSCs). Results showed that epithelial cell colonies were observed up to 2 days after initial seeding. Overall, 80–90% confluency of human UDSCs was reached within 12 days. Some of these cells were also positive for cytokeratin 7. Those that were positive for CD90 were negative for CD45. This study demonstrated the presence of both cell types in fresh urine samples 14 .
Yang et al. also focused on the characterization of UDSCs, but in this study cells were of the animal origin (rabbit). A total of 12 urine and 13 bladder wash samples were used for cell isolation. For the characterization, cell proliferation assay, flow cytometry, Western blot, and immunocytochemistry were used. A differentiation experiment was also performed and stem cells were successfully differentiated into smooth muscle, urothelial, and osteogenic cell lines 15 .
UDSCs seeded on small intestinal submucosa (SIS) were examined in two studies 16,17 . The aim was to engineer a cell-seeded construct that could be applicable for urethral repair. In one study, modified three-dimensional (3D) porous SIS was colonized with human UDSCs, which were differentiated into urothelial and smooth muscle cell lines. The cell source was 12 voided urine samples. The culture medium for smooth muscle differentiation consisted of Dulbecco’s modified Eagle’s medium, EFM, platelet-derived growth factor-BB, and transforming growth factor β1 (TGF-β1). Cells were analyzed after 7 and 14 days. Cell-seeded constructs were cultured under static and dynamic conditions and also applied in vivo. To confirm urothelial and myogenic differentiation, immunohistochemical tests were performed. The results showed the multilayered mucosal structure was formed under dynamic conditions with similar features to the native urothelial tissue 16 .
In another study, autologous rabbit UDSCs were obtained from bladder irrigation solution samples. The media for urothelial and smooth muscle differentiation were the same as in the study above. Seeded UDSCs were labeled with PKH67 to establish cell differentiation. Labeled cell-seeded constructs were transplanted into rabbits to repair the ventral urethral defect. Histological analyses and retrograde urethrograms were performed at various time points. The results revealed that transplanted UDSCs could differentiate into required cell lineages and, when seeded on SIS, the urethral defect could be regenerated 17 .
Using human UDSCs to optimize their differentiation into a functional urothelium together with the emphasis on proper urothelial barrier function was the main aim in the study Wan et al. carried out 18 . The harvested stem cells were cultured both under static and dynamic conditions for 1, 2, or 3 weeks. The following media were used for induction of the UDSCs: conditioned medium obtained from urothelial cells, induced medium supplemented with epidermal growth factor (EGF), and conditioned medium from SMCs supplemented with EGF. An orbital shaker was used for culturing under dynamic conditions. Stem cells were also seeded on a scaffold generated from SIS as well as on the Transwell system to form a multilayered uroepithelium in vitro. Successful differentiation was confirmed via reverse transcription polymerase chain reaction (RT-PCR), Western blotting, and immunofluorescent staining. Permeability assays and transmission electron microscopy were used to assess the properties of the urothelial barrier function. Required phenotypical and functional features were observed in induced UDSCs. When seeded on SIS, induced UDSCs were able to form a multilayered urothelium within 14 days.
The role of the bioreactors and mechanical stimuli in TE
Use of the bioreactor and the influence of in vitro mechanical stimuli was tested in the following studies. Cattan et al. observed terminal urothelium differentiation in engineered tubular grafts that were subjected to dynamic culture conditions. The graft was composed of human dermal fibroblasts and human urothelial cells. No exogenous scaffolding was used. Fibroblasts were cultured for 1 month until they formed tissue sheets. These sheets were subsequently placed on a tubular support and left to mature for another 3 weeks. After this, intraluminal seeding with human urothelial cells was performed. This construct was placed in the bioreactor in which dynamic flow and hydrostatic pressure acted on the graft for 14 days. Histology, immunofluorescence, and RT-PCR were performed as well as electron microscopy and permeation studies. Terminal urothelium differentiation was determined in the results of this study 19 .
In another study, adipose-derived stem cells (ADSCs) and sorted primary epithelial cells were seeded onto a biodegradable poly-glycolic acid (PGA) scaffold and constructs were placed in the bioreactor. The PGA scaffold had a fibrous tubular structure and layered seeding technology was used to load both types of the cell onto the scaffold. Constructs in a bioreactor were subjected to a mechanical extension. Engineered grafts were applied in vivo (beagle dogs) to repair a 1 cm-long urethral defect. Results showed a positive effect of the mechanical extension on viability and differentiation capability of ADSCs. The use of mechanical stimuli together with cell sorting of primary epithelial cells resulted in the successful engineering of the two-layered epithelial-muscular urethra 20 .
The bioreactor was also used in another study in which ADSCs were seeded on a PGA mesh. The goal was to engineer a muscular tube suitable for potential urethral repair. Adipose tissue was harvested from the inguinal regions of adult dogs and the first passage of the isolated stem cells was used for seeding. When induced by 5-azacytidine, ADSCs acquired a myoblast phenotype. The cell-scaffold construct was statically cultured for 7 days and subsequently placed into the bioreactor to be subjected to the mechanical extension for another 5 weeks. The muscular tubes of the urethra were successfully engineered and the importance of the mechanical stimuli on the tissue maturation was highlighted 21 .
Seifarth et al. applied a bioreactor-based technique of mechanotransduction to achieve the bi-directional orientation of porcine bladder SMCs within a structure of the tubular biohybrids. SMCs were isolated from porcine bladders and seeded onto tubular fibrin-poly(vinylidene fluoride) scaffolds. The engineered biohybrid was mechanically stimulated using a balloon kyphoplasty catheter. The bursting pressure together with the permeability of urea and creatinine was also evaluated. The results showed the bidirectional orientation of the primary porcine SMCs in both a circumferential and axial direction 22 .
The ventral penile subcutaneous cavity was used as a bioreactor in a study carried out by Sun et al. Hypoxia-activated human umbilical cord MSCs (hUCMSCs) and pedicled rabbit muscles served as cell sources. hUCMSCs were isolated from fresh human placentas. These cells were cultured under normoxic or hypoxic conditions. Pieces of skeletal muscles were harvested from the rabbits. To prepare a construct suitable for urethral repair, hUCMSCs were mixed with muscle fragments and injected into the ventral penile subcutaneous cavity. Pre-incubation in a bioreactor lasted for 3 weeks. Afterwards, the generated urethral patch was used around the ventral urethral defect. Cells and tissues were tested using histological, immunohistochemical, microscopic, and molecular-genetic analyses. Results showed that hypoxia-activated hUCMSCs continually secreted angiogenic cytokines. The muscle-derived construct was successfully engineered as a living graft and used for urethral reconstruction 23 .
Modulation of the inflammatory response and stricture formation
MSCs combined with CD34+ hematopoietic stem/progenitor cells were used in a study carried out by Liu et al. The aim was to determine whether a graft composed of these cells, which were seeded on poly(1,8-octanediol-co-citrate) (POC), could influence the inflammatory response and enhance wound regeneration when applied in vivo. In this rat-model study, polymerized scaffolds were cut into the desired parameters (2 x 8 x 0.15 mm) and subsequently seeded with bone marrow-derived MSCs and CD14+ hematopoietic stem/ progenitor cells. These grafts were implanted into nude athymic male rats and an unseeded POC scaffold was used in a control group. Histological, immunohistochemical, and microscopic analyses were performed. Postoperatively, the proliferation of MSCs and CD34+ hematopoietic stem/progenitor cells in the area of the substitution was demonstrated by using human-specific γ-tubulin antibodies. A statistically significant decrease in pro-inflammatory markers such as tumor necrosis factor α, interleukin-1β (IL-1β), neutrophil, and macrophage markers myeloperoxidase and CD68 was detected. Results showed that implanted grafts could modulate the inflammatory response, scar formation and promote angiogenesis 24 .
The formation of a stricture after urethral surgery is a common complication that often requires re-operation. Overcoming the scarring and contraction of the urethral tissue was the main interest in the following studies.
Li et al. studied whether TGF-β1 small interfering RNA (siRNA)-transfected fibroblasts could inhibit the secretion of collagen type I and thus reduce stricture formation. Both rabbit oral keratinocytes (isolated from the buccal mucosa) and fibroblasts (harvested from dermal tissue) were used in this experiment. Bladders from male rabbits were decellularized and prepared as bladder acellular matrix grafts (BAMGs). Rabbit fibroblasts were transfected with TGF-β1 siRNA and cell culture medium was collected for 1 week. The concentration of collagen type I was assessed using enzyme-linked immunosorbent assay (ELISA). The second passage of oral keratinocytes was seeded on to BAMG and another side was covered with transfected fibroblasts. Compound grafts were left to mature for 1 week and subsequently implanted into rabbits. The control groups used the following grafts: BAMGs seeded with autologous oral keratinocytes and cell-free BAMGs. Urethral calibers were assessed using retrograde urethrography. Histological, immunohistochemical testing, and scanning electron microscopy evaluated the neo-urethra features. The results showed that transfected fibroblasts could inhibit the secretion of collagen type I. In the experimental group, defected mucosa was successfully repaired without the presence of the strictures 25 .
Epithelial cell-conditioned medium (ECCM) was used to demonstrate the proliferation and migration of the stricture fibroblasts in a study carried out by Nath et al. Patients undergoing urethroplasty were the donors of the urethral mucosa, urethral stricture samples, buccal mucosa, and penile skin. The control group was represented by normal urethras. Hematoxylin and eosin (H&E) and Masson trichrome staining were used for the histological analysis of normal urethral and stricture tissue histology. Fibroblasts were obtained from human urethral stricture samples. Human penile skin, buccal, and urethral mucosa served as a source for the epithelial cells. ECCM was collected from confluent cell cultures of the penile skin, buccal, and urethral mucosa and this medium was added to the fibroblast culture. In vitro scratch assay was chosen as the preferred test and the behavior of the fibroblasts was observed for 3 days. Images were taken using a phase contrast inverted microscope. The results revealed that all three different types of ECCM had an inhibitory potential on stricture fibroblast proliferation and migration in the scratch area. An explanation of this effect could be that specific soluble molecules might have been present in the ECCM 26 .
Vascularization of the engineered tissues
Sufficient vascularization of the engineered tissue is another challenge in regenerative medicine. A cell-based genetic strategy was developed to improve the vascularization of the urethral grafts in a study carried out by Guan et al. The goal was to modify urothelial cells with human vascular EGF (VEGF) via retrovirus transduction. In a control group, urothelial cells were modified with green fluorescent protein (GFP). Eight whole bladders from New Zealand rabbits were used to isolate epithelial cells. Cells from the third passage were used for viral transduction. Transduction efficiency was evaluated 4 days after the procedure. Transgene expression was examined by immunofluorescence and RT-PCR. Western blot and ELISA analyses were also performed. Cells were seeded onto rabbit carotid arteries. Grafts were analyzed by H&E staining or Weigert’s elastic staining. The porosity of the material was assessed by scanning electron microscopy. Modified cells were statically seeded onto scaffolds and left to culture for 1 week. Then 1 cm-long grafts were subsequently implanted subcutaneously into nude mice. Implants were left in vivo for 1 month and analyzed. Results showed that VEGF-modified cells enhanced the neovascularization of the urethral wall and the formation of the urothelium. Moreover, secretion of VEGF appeared to be in a time-dependent manner 27 .
Native collagen and cross-linked collagen membranes were seeded with a tri-culture of primary buccal epithelial cells, fibroblasts, and microvascular endothelial cells to engineer a pre-vascularized buccal mucosa equivalent. Human gingiva served as a source for epithelial cells and fibroblasts. Microvascular endothelial cells were harvested from the human juvenile foreskin. At first, endothelial cells were seeded on to the rough site of the scaffold and left to incubate for 24 hours. Subsequently, fibroblasts were added and cells cultured for 3 days. After this, the scaffold was carefully turned upside-down and epithelial cells were seeded. Cell-seeded scaffolds were cultured for 21 days, implanted in vivo (a murine model) and then analyzed. Results demonstrated that tri-culture of human epithelial cells, fibroblasts, and endothelial cells together with a collagen membrane could form a pre-vascularized buccal mucosa equivalent. Capillary-like structures were better formed on native collagen membrane 28 .
Other approaches used in the urethral TE
In a study carried out by Jiang et al., a natural autologous tubular graft was used for long-segmental urethral reconstruction. At first, silastic tubes were implanted subcutaneously into male New Zealand white rabbits. Tubes were totally covered with granulation tissue 14 days post-implantation. Mesenchymal cells were obtained from omentum biopsies. Pancytokeratin AE1/AE3 and vimentin were used as staining antibodies to prove cells’ phenotypic features. At the third passage, mesenchymal cells were used for seeding onto the outer surface of the tubular tissue (grafts were everted prior to the urethral surgery). Prepared compound grafts, with a length of 2 cm, were incubated for 1 week prior to implantation in animals. Grafts were also analyzed using transmission electron microscopy. Unseeded tubular grafts were used in the control group. Urethral calibers were assessed by retrograde urethrography. Results showed compound grafts consisted of the inner lining of mesothelium, myofibroblasts, and collagen. The urethral lumen in the control group was severely contracted, whereas in the experimental group wide urethral calibers were observed. Moreover, the newly formed urothelium replaced the mesothelium 4 weeks post-implantation 29 .
The transdifferentiation potential of epidermal keratinocytes was investigated in a study in which living skin equivalent (LSE) was considered an alternative graft source for urethral replacement. In total, 20 male chinchilla rabbits were involved. Briefly, the skin biopsy was performed and epidermal rabbit keratinocytes subsequently isolated from the samples. After the destratification and trypsinization of the cell cultures, cells were plated on LSE. A Spongostan sponge and prepared collagen gel containing postnatal human or animal (rabbit) fibroblasts were put into a Petri dish. After 24 hours of incubation, this construct formed a connective tissue equivalent. Autologous keratinocytes used for in vivo testing were labeled with a DiI membrane tracer and transfected with enhanced GFP as well. Cells were subsequently seeded onto the LSE surface. The LSE graft was implanted into the de-epithelialized urethra. Histological and immunohistochemical analyses were performed. The results revealed that keratinocytes acquired phenotypic features characteristic for the urothelium. LSE together with autologous epidermal keratinocytes could fully restore damaged urothelium 30 .
A study carried out by Li et al. investigated the feasibility of epithelial-differentiated rabbit ADSCs (Epith-rASCs) to be the proper cell source for the substitution urethroplasty. Adipose tissue donors were New Zealand rabbits. Passage three of the ADSCs was used for the experiments. Epithelial differentiation was performed in a specific microenvironment established using a 3D culture system. Epith-rASCs were used for in vivo implantation 12 days after initial induction. Epithelial and smooth muscle phenotypes were detected by proteinic and genetic analyses. To establish Epith-rASC differentiation and proliferation capacity, cells were labeled with BrdU. Rabbit BAMGs were used as scaffolds. Matrices were characterized using histological staining and scanning electron microscopy. In the experimental group, BAMGs seeded with Epith-rASCs were incubated for 1 week and subsequently implanted into rabbits. Cell-free BAMGs and BAMGs seeded with undifferentiated rADSCs formed the control groups. A ventral urethral defect with a mean length of 2 cm was repaired using mentioned grafts. Cell proliferation assay, transmission electron microscopy, retrograde urethrography, Western blot and multicolor immunofluorescence analyses were performed. Results showed that Epith-rASCs differentiated into the urothelium and prevented the contraction of the urethral lumen 31 .
Cell sheet technology was used to fabricate the bionic urethra in a study carried out by Zhou et al. The following cell types were used: ADSCs, oral mucosal epithelial cells, and oral mucosal fibroblasts. Cell sheets were prepared from mentioned cell types. For myoblast induction of adipose-derived cell sheets, 5-azacytidine was used. Cell sheets were subsequently tabularized to create a hierarchical structure. Ultra-small super-magnetic iron oxide (USPIO) nanoparticles were synthesized and used for labeling the tissue-engineered urethras. Constructed neo-urethras were subcutaneously implanted in vivo (canine model) for 3 weeks to support the neo-vascularization and mechanical strength of the construct. Afterward, a 2 cm-long urethral defect was created and prepared tissue-engineered urethras were used for the surgical repair. USPIO nanoparticles could be detected by magnetic resonance imaging at the transplant site. Engineered urethras formed a functional three-layer structure and promoted urethral regeneration 32 .
In vitro cultured cells applied in a clinical study
Autologous in vitro cultured urothelial cells were used for hypospadias repair in a clinical study carried out by Fossum et al. Cells were harvested from bladder washings of patients with scrotal or perineal hypospadias and pronounced chordee. The second passage of the urothelial cells was used and seeded on the allogenic acellular dermis. The prepared transplant was subsequently applied in vivo (six patients). Patients were evaluated 6–8 years post-operatively: results revealed the neourethras had a satisfactory function and the cosmetic appearance was good 33 .
Challenges and future directions in urethral TE
As MSCs represent a promising cell source for TE applications, proper culture conditions for sufficient proliferation are crucial. To maintain a typical MSC phenotype not only during the early stages of culture but also after numerous passages, new synthetic culture media together with the optimized combination of the growth and differentiation factors might be a point of interest. Focusing on stem cell reprogramming might also broaden their application.
An engineered functional urothelium should fulfill several requirements that also seem to be major challenges – the cells are interconnected by tight junctions, providing sufficient vascularization and innervation of the new tissue 34 .
Discussion
Urethral strictures are a common pathology of the urethra and management of long-segment strictures presents a challenging surgical problem primarily because of stricture recurrence 3 . So far, the treatment of urethral strictures depends on the length, location, and severity of the urethral strictures. The aim of TE is to reduce recurrence of strictures, morbidity, and the use of invasive methods. TE uses several approaches, scaffolds, cells, cell sources, and techniques mainly in an experimental setting 5 .
In this article, we performed a search within PubMed/Medline to select papers focused on cells used in urethral TE. Based on results, various cell types such as hUDSCs, UDSCs, MSCs, and ADSCs and several techniques for urine cell harvesting (urethral catheterization, spontaneously voided urine, bladder irrigation, and bladder washing) have been utilized in this context (Table 1).
Overview of Cells Used in Urethral Tissue Engineering.
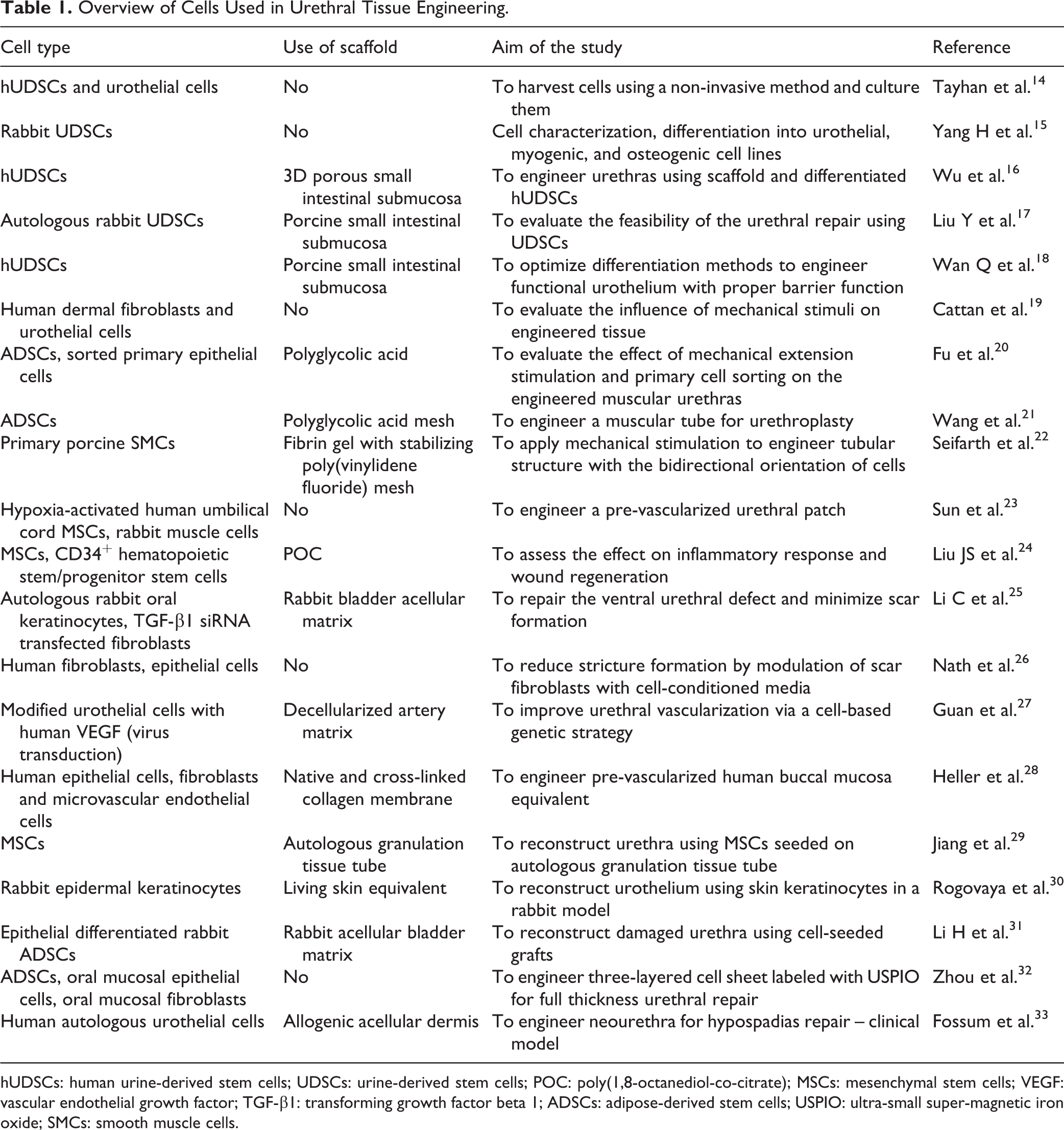
hUDSCs: human urine-derived stem cells; UDSCs: urine-derived stem cells; POC: poly(1,8-octanediol-co-citrate); MSCs: mesenchymal stem cells; VEGF: vascular endothelial growth factor; TGF-β1: transforming growth factor beta 1; ADSCs: adipose-derived stem cells; USPIO: ultra-small super-magnetic iron oxide; SMCs: smooth muscle cells.
Based on a comparison of different tissue sources and because spontaneously voided urine, which is considered biological waste, is a non-invasive and low-cost technique, urine should be considered a reliable source of cells. These cells display characteristics comparable to MS (stromal) cells 35 . However, articles describing the use of this source are still scarce 7,33 .
Previously mentioned studies in this review prove that urine is a suitable cell source for urethral TE and that using proper scaffolds and bioreactors can create biologically and biomechanically functional tissue that can be used for urethral TE. Because of telomerase activity, the proliferation capacity of these cells is high. Moreover, they attach well on various surfaces, which highlights their MSC origin. When differentiated into smooth muscle or urothelial cell lines, typical markers can be detected (e.g., α- smooth muscle actin, desmin, myosin, cytokeratins, and uroplakins). Within this context, one study compared the differentiation capability of UDSCs with bone marrow-derived stem cells. Results showed that for both cell types, differentiation into smooth muscle cell line was successful. However, generating urothelial cells was much more efficient in UDSCs (70:5% success rate). This phenomenon might be due to their uroepithelial origin 36,37 .
Until now, the kind of cultivation method and type of cell that should be used for urethral TE has been a matter of debate. The results from experimental studies demonstrate the importance of dynamic conditions during in vitro cultivation, which are provided by bioreactors. They positively influenced the proliferation of cells, their growth into the scaffolds, and the maturation of engineered tissues 17,19,20 –23 .
Moreover, several interesting techniques were introduced to reduce scarring and scar formation (TGF-β1 siRNA-transfected fibroblasts, modulation of scar fibroblasts with cell-conditioned media), which could be used alone or in combination with other techniques (e.g., using modified urothelial cells with human VEGF by virus transduction) 25 –28 .
For clinical use and implantation in vivo, tubular multilayered tissue engineered grafts show much promise, but the lack of clinical trials limits their broader use in a clinical setting.
Conclusions
This systematic review summarizes recent articles on cells used in urethral TE. Cell culture techniques and ADSC (human and rabbit), UDSC, human urothelial, fibroblasts, and keratinocytes cell types were studied using different types of scaffold or a scaffold-free approach. Studies show that proliferation and differentiation of cultured cells are affected both by the culture conditions and type of scaffold. After choosing the cell source and cell culture technique, the choice of a scaffold (biological, synthetic, composite) is another determinant of the clinical outcome. Currently used scaffolds show varied results. However, there is no standardized or optimal scaffold that could be recommended for use in a clinical setting. In the near future, development can be expected in the construction of new bioreactors providing dynamic cultivation conditions that may improve the process of cell proliferation and differentiation.
To reduce invasivity, autologous urinary stem cells and autologous ADSCs show much promise, as they can be expanded in vitro and used for TE and 3D bioprinting. Further development of urethral TE may be associated mainly with introducing new composite biomaterial and 3D bioprinting technology in combination with various cells including urinary stem cells to mimic the native urethral architecture.
Current trends of experimental studies in the context of urethral TE might be summarized as follows. The focus is on the use of UDSCs, as their harvesting is non-invasive and economic, and efficient stem cell differentiation with proper culture media supplemented with regulatory factors (growth, differentiation) is highlighted, as the application of an inadequately engineered construct in vivo might lead to urine leakage or insufficient vascular supply with resultant stricture formation. A detailed understanding of immunomodulatory processes under in vitro conditions provides the necessary insight on how urethral strictures are formed. As contraction and expansion are the physiological features of the urethra that might be mimicked in vitro under dynamic conditions, bioreactors play a key role in the process of tissue maturation. Another crucial point is to develop a technique to provide sufficient nutrient supply for the engineered construct, which could also enhance long-urethral segment reconstruction using TE approaches. This type of reconstruction requires an adequate tubular cell-seeded graft with the inner lining of the urothelium and outer lining composed of SMCs. Therefore tubularization of TE constructs is also a point of interest. Cell labeling with specific particles allows better visualization of the reconstructed tissue site.
This review shows that many studies have been done on animal experiments. However, the transformation of these results is still lacking in the field of clinical medicine.
Footnotes
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
There are no human subjects in this article and informed consent is not applicable.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Presented work was supported by the grants APVV-15-0111 and UK/240/2018.