
Abstract
To determine whether non-alcoholic fatty liver disease (NAFLD) and intracerebral hemorrhage (ICH) are connected, and assess the role played by NAFLD in ICH development. A retrospective study evaluated inpatients treated at the First Affiliated Hospital of Zhejiang University. We divided the patients into Group A (ICH with NAFLD) and Group B (ICH alone). Moreover, univariate and multivariate logistic regression analyses were performed to identify the risk factors for unfavorable outcomes. A total of 128 patients were included: 34 ICH with NAFLD (group A) and 94 ICH (group B). Sixteen patients exhibited an unfavorable outcome. There was no significant difference among the two groups on the underlying diseases hypertension and heart disease. Group A had more diabetes mellitus cases (35.29% vs 12.76%, p = 0.004). Levels of alanine aminotransferase and triglyceride were higher in group A than in group B (all p < 0.05), while differences in other blood biochemistry tests were statistically insignificant (all p > 0.05). There was a similarity in bleeding sites except for brainstem hemorrhage, which was higher in group B patients (p = 0.036). Multivariate logistic regression analysis revealed that low-density lipoprotein (OR, 0.278; 95% CI (0.107–0.702), p = 0.008) was a protective factor for ICH patients with NAFLD. The National Institute of Health Stroke Scale (NIHSS) score at discharge (OR, 3.152; 95% CI (1.532–6.486), p = 0.002) was independent of risk factors for unfavorable outcomes. Serum levels of LDL was a protective factor. NAFLD did not increase the unfavorable outcome of ICH patients in our study.
Introduction
The incidence of spontaneous intracerebral hemorrhage (ICH) prevails worldwide and is associated with disability or death 1,2 , causing a heavy burden all over the world. During the first month of ICH ictus, >66% of patients fail to make a good functional recovery 3 ; mortality is 35–52% and only 20% of all patients are independent 6 months later 4,5 . ICH accounts for 10–20% of all strokes 1 .
Hemostatic therapy in the early hours is an effective way to control hematoma growth 6 . Stringent blood control indicated a favorable outcome and functional improvements in an large cohort RCT 7 , and lowering blood pressure to 140 mmHg is recommended by American Heart Association/American Stroke Association (AHA/ASA) guidelines 8 . New therapeutic strategies such as stem cell therapy or biologics, are being developed 9,10 . For instance, it was reported that the application of umbilical cord blood mesenchymal stem cells(UC-MSCs) led to a significant improvement of neurological function in ICH rats 11 . A study by Zhao et al. demonstrated that low dose 6-bromoindirubin-3’-oxime (BIO) treatment was neuroprotective in a mouse model of ICH 12 .
Risk factors for ICH have been extensively investigated. Patients with type 2 diabetes mellitus (T2DM), hyperlipidemia, and infection 13 are vulnerable to suffer from ICH attack. Besides, patients with hypertension 14 , cerebral amyloid angiopathy 15 , vascular abnormalities, the use of anticoagulant or antiplatelet drugs 16 , and tumor-induced vasculitis 17 , are also at increased risk of ICH.
The incidence of non-alcoholic fatty liver disease (NAFLD) is increasing worldwide 18 , and it constitutes a large proportion of all liver disease. NAFLD ranges from steatosis to cirrhosis 19 , and is associated with dyslipidemia, hypertension, and obesity 20 –22 . Several studies have documented associations between NAFLD and an increased risk of cardiovascular morbidity 23,24 . However, much more remains to be explored.
We compared patients with ICH, with or without NAFLD to explore any possible connection between the diseases, and assessed the role played by NAFLD in ICH development, and risk factors for unfavorable outcomes. This study hypothesized that if ICH and NAFLD were linked, early intervention would improve ICH prognosis.
Materials and Methods
Inclusion and Exclusion Criteria
This retrospective study was performed on inpatients treated in the neurology ward from January 2010 to October 2016 in the First Affiliated Hospital of Zhejiang University. We enrolled only spontaneous hemorrhagic patients, thus excluding those with traumatic hemorrhage. Magnetic resonance imaging (MRI) or computed tomography (CT) confirmed all hemorrhages, thus excluding other possible pathologies (such as tumors). All of the patients were evaluated within 1 week of hemorrhage. Patients with a previous history of intracranial hemorrhage were also excluded, as were the patients treated in other hospitals before transferring to our hospital. Patients with vascular malformations were also excluded based on evidence from the CT angiography or digital subtraction angiography. All the included patients underwent liver ultrasonography to identify NAFLD. The study excluded patients who consumed >20 g/day of alcohol as presumably having alcoholic liver disease 25 . Locations of ICH were divided into Deep (thalamus, basal ganglia), Labor (the cortex sections with or without involvement of subcortical white matter), Brainstem, and Cerebellum. The study divided all the patients into two groups: A (ICH with NAFLD, 34 patients) and B (ICH only, 94 patients). Both groups were age- and sex-matched. We adhered to all relevant principles of the Declaration of Helsinki. Moreover, The Ethics Committee of the First Affiliated Hospital of Zhejiang University approved the study.
Clinical Data
We recorded any presumable history of hypertension, T2DM, alcohol intake, and/or heart disease. This study defined hypertension as systolic blood pressure (SBP) > 140 mmHg and/or a diastolic blood pressure (DBP) > 90 mmHg, or a history of antihypertensive drug use. The blood pressures during presence in the emergency room were recorded. The patients and/or their family members estimated alcohol consumption. Body mass index (BMI) was calculated on admission as the weight divided by height squared (kg/m2). Systolic and diastolic blood pressure were referred to records without intervention at admission, all blood tests were performed within 24 h of admission. We measured the levels of alanine aminotransferase (ALT), aspartate transaminase (AST), r-glutamyl transferase (r-GT), high-density lipoprotein (HDL), low-density lipoprotein (LDL), triglyceride (TG), and total cholesterol (TC). The ICH location, National Institutes of Health Stroke Scale (NIHSS) score, neutrophil-to-lymphocyte ratio (NLR), infection status, and condition at discharge were also recorded.
Outcomes
We compared condition at discharge with condition at admission. Neurological deterioration ≥ 4 points from the baseline NIHSS score after initiation of treatment, or death, was defined as an unfavorable outcome.
Statistical Analyses
This study used SPSS software ver. 21.0 for all data analyses. Chi-squared or Fisher’s exact test were performed to compare categorical variables between the groups. Continuous variables were shown as means with standard deviations. Also, we conducted an independent sample of student’s t-test continuous variables between the groups. A p-value < 0.05 was considered statistically significant.
Results
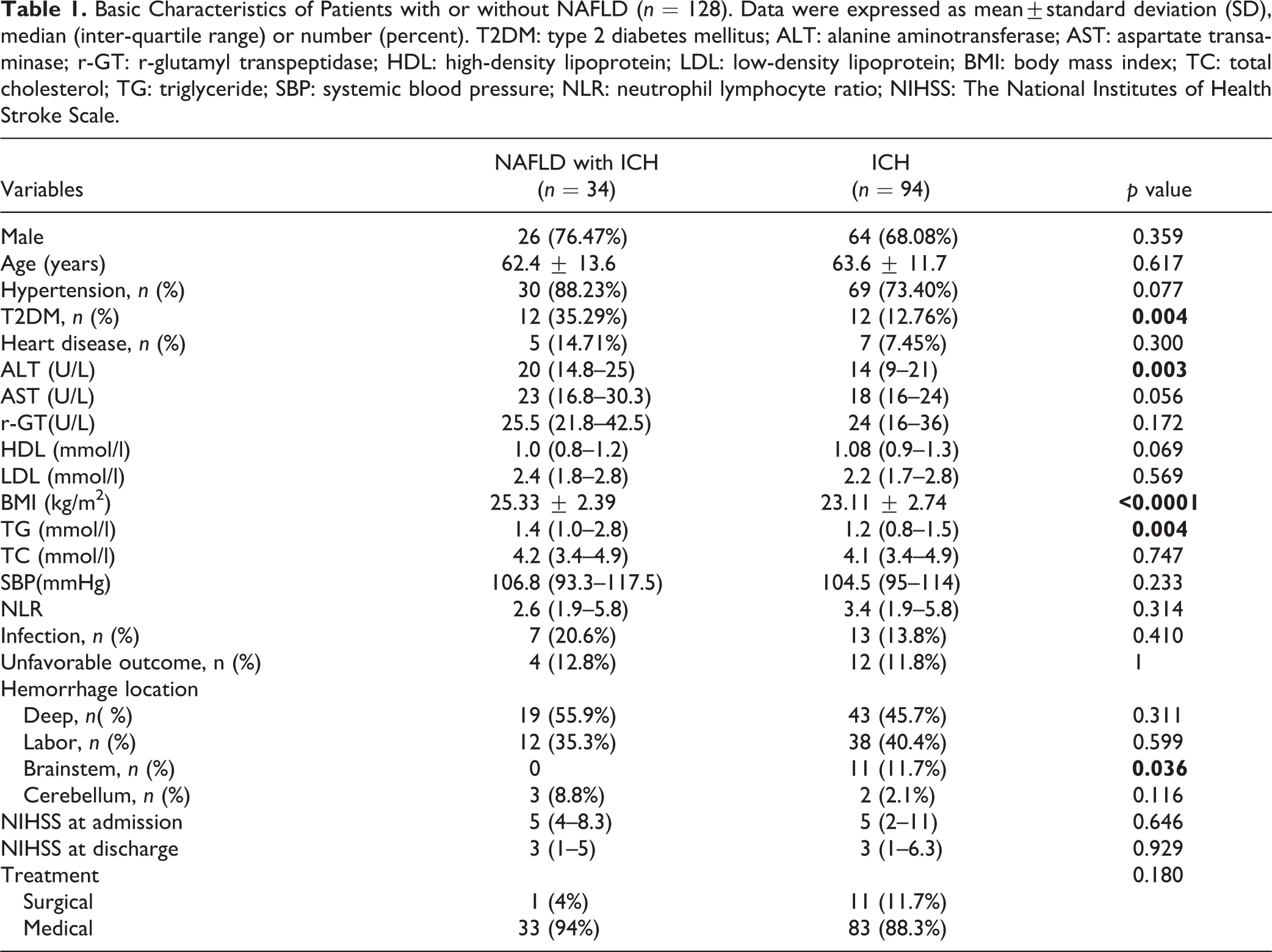
We enrolled 1155 inpatients in the neurology ward, of whom 647 were excluded because liver ultrasonography data were lacking, 305 had incomplete data, 23 had a history of ICH, and 52 had ICH of other etiologies. We finally included 128 patients. There were 34 ICH with NAFLD (group A) and 94 with ICH (group B) (Table 1). There was no significant difference among the two groups on underlying diseases, such as hypertension and heart disease. T2DM was more prevalent in group A (35.29% vs 12.76%, p = 0.004). Levels of ALT and TG were higher in group A than group B (all p < 0.05), while the difference of other blood biochemistry tests was not significant in statistics (all p > 0.05). There was a similarity in the bleeding sites, except for brainstem hemorrhage in the two groups, which was higher in group B patients (p = 0.036). Of the 34 group A patients, 1 received surgery, compared with 11 out of 94 in group B (p > 0.05).
Basic Characteristics of Patients with or without NAFLD (n = 128). Data were expressed as mean±standard deviation (SD), median (inter-quartile range) or number (percent). T2DM: type 2 diabetes mellitus; ALT: alanine aminotransferase; AST: aspartate transaminase; r-GT: r-glutamyl transpeptidase; HDL: high-density lipoprotein; LDL: low-density lipoprotein; BMI: body mass index; TC: total cholesterol; TG: triglyceride; SBP: systemic blood pressure; NLR: neutrophil lymphocyte ratio; NIHSS: The National Institutes of Health Stroke Scale.
In total, 16 patients had unfavorable outcomes. In the Univariate analysis, factors associated with unfavorable outcomes were WBC, HDL, LDL, AST, NLR, or NIHSS score at discharge (OR, 1.191, 95%CI (1.026–1.384), p = 0.022) (Table 2). By multivariate analysis, LDL (OR, 0.278; 95%CI (0.107–0.702), p = 0.008) was a protective factor for ICH patients with NAFLD. NIHSS score at discharge (OR, 3.152; 95%CI (1.532–6.486), p = 0.002) was an independent risk factor for an unfavorable outcome (Table 2).
Risk Factors Associated with Unfavorable Outcome in ICH Patients with and without NALFD. Statistical Analysis was performed using univariate and multivariate analysis. WBC: white blood cell; HDL: high-density lipoprotein; LDL: low-density lipoprotein; AST: aspartate transaminase; NLR: neutrophil lymphocyte ratio; NIHSS: the National Institutes of Health Stroke Scale.

Discussion
Few reports on a possible connection between ICH and NAFLD exist; it is uncertain whether NAFLD affects ICH development or severity. Therefore, we aimed to explore a possible association. We found that Group A patients had a greater prevalence of T2DM and a higher BMI than Group B patients; the TG level was significantly higher in Group A, although the HDL level was lower. However, there was no difference between hemorrhagic features and the severity of ICH.
The ALT levels were similar in Groups A and B. ALT may remain within the reference range in patients with NAFLD 26,27 . Thus, we considered that Group A patients exhibited early-stage steatohepatitis. Liver function did not differ between the two groups. Table 1 illustrates that there was no difference in ICH features between the groups, except for hemorrhage in brainstem. The limited sample size may explain the apparent significant difference between group A and group B patients. There is increasing evidence that NAFLD not only affects the liver but is also a multisystem disease that increases T2DM, cardiovascular, and cardiac diseases 28 . However, although our results showed that NAFLD had no obvious effect on ICH severity, it remains possible that advanced NAFLD (our patients did not have advanced disease) affects ICH development; this will require further investigation.
Hypertension 29 and T2DM 30,31 increase the risk of ICH. As all our patients had ICH, the prevalence of these two conditions was very high in both groups. Admission SBP did not differ between the two groups, although mean levels were higher than normal. A high SBP after therapy for acute ICH suggests poor outcome 32 . Both diabetes and an elevated BMI are closely associated with NAFLD, explaining the differences evident between the two groups. An elevated BMI may increase the likelihood of ICH 33,34 . Hypercholesterolemia and hypo-HDL cholesterolemia increase the incidence of ICH 35,36 . Dyslipidemia is often accompanied by fatty liver disease (FLD), explaining why Group A patients had a higher TG but lower HDL level than Group B patients. Surgical or medical therapy suggests no significant difference in outcome in our study, which is consistent with two serial RCTs 37,38 . Less invasive surgery is a trend for ICH therapy; however, large scale studies about its effects on outcome are lacking. Increasing evidence suggests that NAFLD is a major risk factor for the development of cardiovascular disease (CVD) 39 , but any effect of NAFLD on ICH development remains unclear. Risk factors for ICH vary by ICH location. Cerebral amyloid angiopathy causes non-ventricular hemorrhage, but ventricular hemorrhage is always attributed to hypertension 14 . The NLR is used as an indicator of inflammation caused by infection and indicates that 20% of patients in both the Groups A and B are infected. Therefore, NAFLD had no effect on the NLR of ICH patients.
The NIHSS score at discharge was a risk factor for unfavorable outcome in our study (OR 3.152, p = 0.002), which is consistent with the study of Ji et al 40 . Moreover, in a study by Satopaa et al., comparing 19 published prognostic scores, the authors concluded that NIHSS was the best and should be performed to quantify risk factors for in-hospital death 41 . NIHSS score at admission was not a significant prognostic factor, which may mean that the condition is changing rapidly. We consider treatment initiation of NIHSS might be more suitable for the prediction. However, because this was a retrospective study, the original medical record data only recorded the NIHSS score at admission, and, unfortunately, there was no score at the beginning of treatment; hence, data collection at various time-intervals should be more precise in future research.
Increasingly, studies focusing on the interaction of NAFLD with T2DM, CVD, chronic kidney disease (CKD) are indicating that NAFLD affects multiple systems and may associate with the pathogenesis of these extra-hepatic chronic illnesses 28 . Research on the pathogenesis of ICH is gradually being investigated, and factors affecting the prognosis of ICH have also been discussed extensively. Although our research achieved negative results, the possibility of correlation between the two diseases still cannot be ruled out. Therefore, it requires more systematic and in-depth research.
Limitations to our study exist. Firstly, our study was a single-centered retrospective study, which may limit generalizability to other centers. Excluding a number of ICH patients who did not undergo liver ultrasonography may have affected our conclusion. Together with the short time frame due to lack of follow up data, other unknown biases may also have occurred. C-Reactive protein level is a good indicator of ICH, but as data were lacking for >50% of patients, we did not include this index.
In conclusion, patients with ICH and NAFLD differed from ICH patients in terms of the prevalence of T2DM, BMI, and HDL and TG levels, while NAFLD did not affect ICH development or severity. LDL was a protective factor for ICH patients with NAFLD, whereas NIHSS score at discharge was a risk factor for unfavorable outcome.
Footnotes
Author Contributions
JF Sheng, RH Zhao, AW Shao designed the study, RH Zhao, S Tu, H Fang and CN Jin collected and analyzed the data. RH Zhao, S Tu, H Fang, CN Jin, JF Sheng and AW Shao drafted the manuscript; JF Sheng and AW Shao reviewed and modified the manuscript. All authors agreed on the final version.
Statement of Human and Animal Rights
All procedures in this study were conducted in accordance with the First Affiliated Hospital of Zhejiang University Ethics Committee-approved protocols.
Statement of Informed Consent
Written informed consent was obtained from the patients for their anonymized information to be published in this article.
Ethical Approval
Ethical approval to report this case series was obtained from the Ethics Committee of The First Affiliated Hospital of Zhejiang University.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by China Postdoctoral Science Foundation (2017M612010) and National Natural Science Foundation of China (81701144, 81670567).