
Abstract
An increasing number of unruptured intracranial aneurysms (UIAs) has been discovered in elderly patients in recent years, but the optimal treatment strategy for these patients remains controversial. We report our six-year experience treating UIAs in elderly patients (≥ 70 years old). A retrospective review was conducted of elderly patients who harbored UIAs treated by conservative observation, microsurgical clipping, or endovascular coiling between January 2009 and December 2014. The patients’ clinical and imaging information was recorded. Treating methods, procedure-related complications, imaging results, and clinical outcomes were analyzed. A total of 141 consecutive elderly patients with 166 UIAs were enrolled in our study. In all, 64 patients with 79 aneurysms were treated with coiling, and 14 patients with 14 aneurysms were treated with clipping. The remaining 63 patients with 73 aneurysms were placed under conservative observation. The average modified Rankin scale was 0.99 (range 0–6) in the full cohort after a mean follow-up of 50.4 months (range 0–70 months). There was no significant difference of modified Rankin scale in patients with UIAs treated by different methods. Multivariate analysis showed that age (p=0.030) and aneurysm size (p=0.011) were independent risk factors for unfavorable outcome of UIAs in the elderly. Patient age (p=0.010) and aneurysm size (p=0.020) were also significantly associated with unfavorable outcome of UIAs managed with observation initially. Our results indicated that endovascular coil embolization and clipping were both safe and effective treatment methods for UIAs in the elderly. Aggressive treatment for UIAs in elderly patients with risk factors of aneurysm rupture should be considered positively.
Introduction
Due to the increasing proportion of elderly individuals and development of non-invasive imaging techniques, more and more unruptured intracranial aneurysms (UIAs) have been diagnosed in the elderly. Much debate has surrounded which technique better treats UIAs. A recent study demonstrated that endovascular coiling was associated with a lower rate of mortality and short-term complications compared with clipping 1 . However, the recurrence rate was higher with endovascular coiling 2 . For elderly patients, there is a trend that endovascular treatment is more favorable 3 . However, physiologic changes accompanied with aging can increase this method’s difficulty, such as vasculature tortuosity and atherosclerosis. Microsurgery is more durable but quite invasive. For these reasons, some elderly patients chose conservative therapy for fear of surgical complications 4 .
During the past several decades, the development of microsurgical and endovascular techniques has greatly improved outcomes in patients with intracranial aneurysms. Meanwhile, the advancement of neurocritical care and monitoring warrants the safety related to aggressive treatment 5,6 . These factors expand the indications for the management of intracranial aneurysms in elderly patients.
Following the trend of global aging, China has entered the accelerated aging period, and the number of elderly patients with intracranial aneurysms is increasing. How to treat patients in this setting is still a challenging question for neurosurgeons. Thus, this paper retrospectively summarizes the clinical and radiological data of elderly patients (≥ 70 years) with UIAs in our hospital between January 2009 and December 2014, evaluates risk factors associated with their surgical outcomes, and identifies risk factors for UIAs ruptured in this era.
Materials and Methods
Patients
The Research Ethics Board of our institution approved the protocol for this retrospective, single-center study. During the study period (January 2009 to December 2014), all patients harboring intracranial aneurysm were evaluated as potential candidates for the study. The inclusion criteria included: age >70 years old; 2) angiographically verified intracerebral aneurysm. The exclusion criteria were: 1) patients with aneurysmal subarachnoid hemorrhage (SAH); 2) life expectancy less than one year because of another medical condition. A total of 213 consecutive patients with 252 aneurysms were enrolled in our study, including 141 patients who harbored 166 UIAs and 72 patients with ruptured aneurysms. Patients with SAH were excluded. There were 20 male and 43 female patients in the conservative group, with a mean age of 75.08±4.04; 20 male and 44 female patients in the coiling group, with a mean age of 74.09±3.88, and 4 male and 10 female patients in the clipping group, with a mean age of 73.28±2.81, respectively. All the patients gave written informed consent to participate. The treatment strategy was determined the discussion between the neurosurgeon and neurointervention specialist and willing patients. We reviewed the records of these patients to better understand the outcomes obtained using different treatment methods. Hospital records, neuroimaging data, operative reports, and follow-up notes were available in all cases.
Clinical and Angiographic Outcomes
We retrospectively accessed clinical outcomes on patients at discharge and at last follow-up using the modified Rankin Scale (mRS) respectively; scores of 3–6 represent unfavorable outcome and scores of 0–2 mean good outcome. Complications about ischemic stroke, intracerebral hemorrhage and general complication were also recorded. For follow-up, patients should have computed tomography angiography (CTA) or magnetic resonance angiography performed at three months after the operation and digital subtraction angiography (DSA) at six months or one year after procedure and then follow-up yearly. Repeated angiography confirmed the degree of occlusion, including complete (100% occlusion), neck remnant (>95% occlusion) and partial occlusion (<95% occlusion) and the modified Rankin scale (mRS) was used to measure the clinical outcome at the last follow-up. All follow-ups were performed by return visit and telephone calls. The surviving patients were followed for up to 70 months (50.4 months on average).
Statistical Analysis
Statistical analysis was performed with JMP 12 (SAS Institute, Inc., Cary, NC, USA). Normally distributed continuous data are presented as the mean ± standard deviation (SD). Differences in continuous variables were analyzed with either an independent-sample t-test or one-way analysis of variance test, whereas differences in categorical variables were carried out with either a χ2 test or Fisher’s exact test. A multivariate logistic regression analysis was performed to analyze the risk factors for unfavorable outcomes of intracranial aneurysms and rupture of UIAs in the elderly. A p-value <0.05 was considered to be statistically significant.
Results
General Information
A total of 213 consecutive patients with 252 aneurysms were enrolled in our study, including 141 patients who harbored 166 UIAs and 72 patients with ruptured aneurysms. The SAH patients (Hunt and Hess grade I–II, n=42; III–IV, n=30) were excluded. Of 141 patients, 64 patients (45.4%) with 79 aneurysms were treated with coiling and 14 patients (9.9%) with 14 aneurysms were treated with clipping. The remaining 63 patients (44.7%) with 73 aneurysms were under conservative observation (Fig. 1). Patient and aneurysm baseline characteristics are summarized in Table 1.

Distribution of three treatment modalities of 213 patients in this study.
Baseline Characteristics of Intracranial Aneurysms in Elderly Patients*.

* Data in parentheses are percentages. There were 64 patients with 79 aneurysms treated by coiling, 14 patients with 14 aneurysms treated by surgery and 63 patients with 73 aneurysms under conservative observation.
# Data are number of aneurysms.
Surgical Complications
Procedure-related complications occurred in four patients who received aneurysm coiling and three who received aneurysm clipping (Table 2). Of these 64, two (3.12%) patients suffered severe symptomatic neurological complications in the coiling group compared with one (7.14%, 1/14) in the clipping group. Two of these three patients died due to complications, and the other patient had permanent hemiparesis and dysphasia related to a postoperative ischemic event. Neurosurgical complications not associated with a neurological deficit included two asymptomatic infarctions and two small hematomas, resulting in a rate of 3.12% (2/64) in the coiling group and 14.29% (2/14) in the clipping group. Systemic complications consisted of four episodes of heart dysfunction and two episodes of pneumonia. There was a significantly higher rate of general complications in the clipping group than in the coiling group on this issue (p=0.033). Detailed information of surgical complications is shown in Table 2.
Surgical Complications.

Clinical Outcomes
The average mRS was 0.99 (range 0–6) in the full cohort after a mean follow-up of 50.4 months (range 0–70 months). Of the 129 patients with mRS scores of favorable outcome, 55 (87.3%) patients belonged to the conservative group, 62 (96.8%) belonged to the coiling group, and 12 (85.7%) belonged to the clipping group. There was no significant difference of mRS in patients with UIAs treated by different methods (odds ratio (OR) 0.224, 95% confidence interval (CI) 0.046–1.093, p=0.064, coiling versus conservative group; OR 1.100, 95% CI 0.203–5.944, p=0.912, clipping versus conservative group; OR 0.204, 95% CI 0.26–1.606, p=0.131, coiling versus clipping group) (Fig. 2(A)). For untreated patients, eight achieved unfavorable outcomes at the last follow-up, including six patients experiencing SAH and two patients with ischemic stroke who were excluded from the analysis of UIA rupture rate. The cumulative rate of SAH for untreated UIAs was 6.78% (95% CI 6.7–29.7) at 24 months after diagnosis and 11.6% (95% CI 10.85–27.09) at 69 months after diagnosis (Fig. 3).

Clinical and image outcome at the last follow-up. (A) Distribution of modified Rankin scale score at the last follow-up for intracranial aneurysm in elderly patients (odds ratio (OR) 0.224, 95% confidence interval (CI) 0.046–1.093, p=0.064, coiling versus conservative group; OR 1.100, 95% CI 0.203–5.944, p=0.912, clipping versus conservative group; OR 0.204, 95% CI 0.26–1.606, p=0.131, coiling versus clipping group). (B) Image outcome of treated unruptured intracranial aneurysms in elderly patients at last follow-up (OR 1.61, 95% CI –1.769 to 2.720; p=0.679).

Kaplan–Meier curve showing the cumulative rates of subarachnoid hemorrhage (SAH) for untreated unruptured intracranial aneurysms.
Imaging Follow-Up
Imaging follow-up (range 6–66 months; mean 40.5 months) was performed by CTA or DSA in 61 patients. Forty-three of 49 patients (87.8%) in the coiling group showed complete occlusion compared with 11 of 12 (91.7%) in the clipping group; three patients (6.1%) in the coiling group and one patient (8.3%) in the clipping group showed neck remnant. In addition, three patients (6.1%) suffered from aneurysm recanalization in the coiling group. However, we found no difference in angiographic outcome between coiling and clipping in this aged cohort (OR 1.61; 95% CI –1.769 to 2.720; p=0.679) (Fig. 2(B)).
Predictors of Poor Outcome of All Patients and Untreated Patients
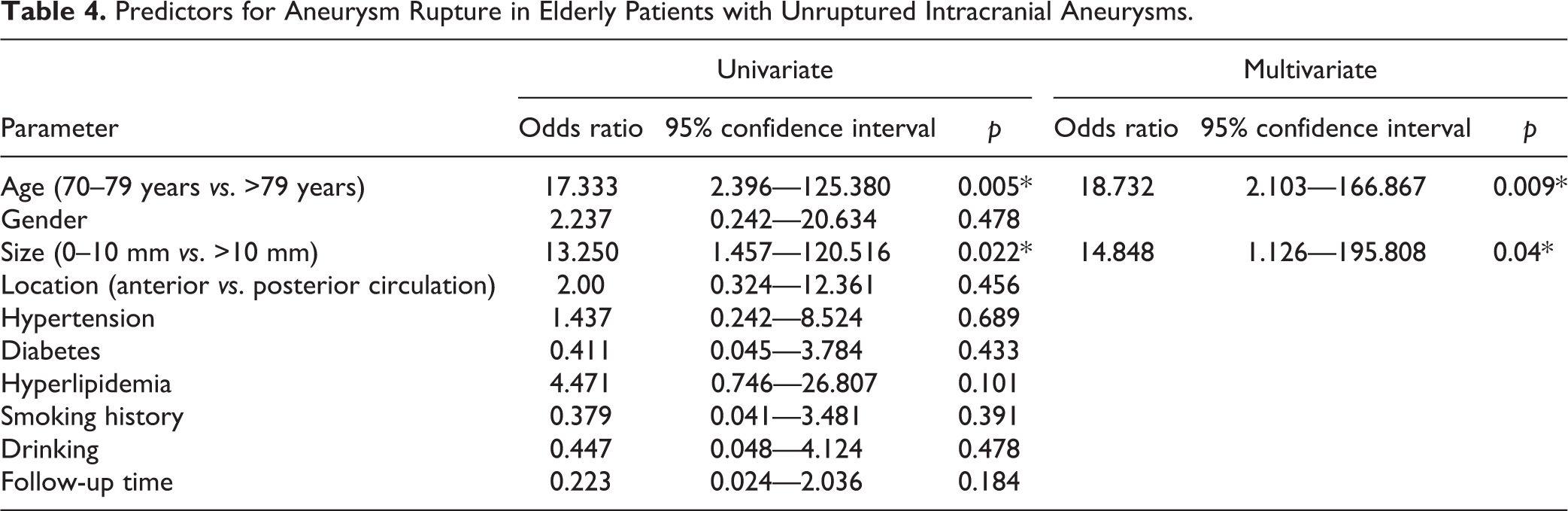
Based on univariate analysis, the following variables were associated with unfavorable outcome (morbidity, mortality, and aneurysm recanalization) in the elderly patients: age (p=0.023) and aneurysm size (p=0.009). Using multivariate logistic regression, we found that age (p=0.030) and aneurysm size (p=0.011) were also independent risk factors for intracranial aneurysm in the elderly (Table 3). Furthermore, we also analyzed the predictors of poor outcomes in elderly UIAs in the aggressive surgery group (coiling and clipping) and conservative group respectively. In the aggressive surgery group, the aneurysm size (0.023) and heart dysfunction (0.028) were related to the poor outcomes in the elderly (Supplementary Material Table 1 online). However, age (0.018) and the aneurysm size (0.009) were independent risk factors for intracranial aneurysms that underwent conservative therapy (Supplementary Table 2). We also performed a multivariate logistic regression analysis to analyze risk factors of unfavorable outcome for UIAs managed with observation initially, which demonstrated that age (p=0.01) and aneurysm size (p=0.02) were independent risk factors of aneurysm with unfavorable outcome in the elderly (Table 4).
Prognostic Factors for Unfavorable Outcomes in Elderly Patients with Unruptured Intracranial Aneurysms.

Predictors for Aneurysm Rupture in Elderly Patients with Unruptured Intracranial Aneurysms.
Discussion
How to manage UIAs in elderly patients is always controversial. Clinicians should perform aggressive therapy on ruptured aneurysms if the patients are admitted in good condition 7,8 , and conservative therapy may be the first choice in elderly patients in poor initial condition 9,10 , which was the same as the result of our excluded SAH patients, especially for patients initially suffering grade I–III SAH in our research, 54.5% (6/11) of whom died or became disabled as a result of aneurysm rebleeding. Therefore, it is of great importance for patients with low-grade SAH to undergo aggressive treatment. Compared with the prevalence of ruptured aneurysms, the prevalence of UIAs is even higher in the elderly. Much literature has been produced regarding the management of UIAs 11 –14 . However, the data on how to treat UIAs in the elderly are lacking. Due to special characteristics of elderly patients, such as poor health, malnutrition, and high rate of perioperative complications, how to treat UIAs in aged patients is still under debate. Treatment paradigms for aneurysms in elderly patients have shifted dramatically over the past 10 years. Historically, most elderly patients with intracranial aneurysms were ruled out from surgery because of poor outcome and high risk 4 . However, this has changed, especially since the revolutionary endovascular technique began to emerge. Endovascular coil embolization has been widely used to treat intracranial aneurysms because it is less invasive, which is considered more favorable for elderly patients with weak health and poor tolerance of invasive treatment 15,16 . Although endovascular treatment has benefits for the elderly, its efficacy is still under debate. A recent meta-analysis demonstrated that endovascular treatment in the elderly is effective but associated with a perioperative complication rate of 14%, leading to high morbidity and mortality, especially in SAH patients 17 . Meanwhile, open surgery is now becoming safer and tolerated in patients even in their eighth decade with the assistance of modern intraoperative monitoring and postoperative intensive care 5,6 . In our study, although clipping caused more asymptomatic procedure-related complications than coiling, these complications had no further impact on patients’ neurological condition. These results differ from the previous viewpoint that endovascular coiling had decreased morbidity and mortality compared with surgical clipping 11,18 . We believe that intraoperative monitoring and postoperative intensive care played an important role in preventing permanent neurological deficits in our patients. The routine application of intraoperative motor evoked potential monitoring and Doppler ultrasound improved the preservation of parent artery and perforators and reduced the occurrence of catastrophic ischemia. According to our data, therefore, endovascular coiling and clipping were both safe and effective for intracranial aneurysms in older patients. Notably, however, the number of clipping procedures was still limited in this cohort due to patient concerns. In fact, aneurysm clipping could also achieve complement meant good outcomes for some suitable elderly patients.
Age played an important role in the outcomes of treatment of UIAs. When age increases, patients treated with coiling have less morbidity and mortality than those treated with surgical clipping 11,18 . In addition, age itself has been reported to be a risk factor for aneurysm rupture 19 . Conversely, increasing age has been a factor in more surgical complications 20 . Hence, the paradoxical relationship between aged-related rupture risk and surgical risk makes the management of UIAs in elderly patients more difficult. Many elderly patients preferred conservative treatment due to fear of surgical complications. Our cohort revealed comparable outcomes between the aggressive treatment group and the conservative observation group. This result coincided with our concept that the aggressive management for UIAs should be determined with careful evaluation of many factors, including age, health, durability, life expectancy, vascular condition, and aneurysm features. Based on our result, we consider that the overall outcomes of UIAs in the elderly treated with different methods are similar. However, our data also showed that the cumulative rate of SAH in the conservative group was very high, which brought poor outcomes for patients. Therefore, the indication of treatment of UIAs in elderly patients should be determined individually.
On multivariate analysis, age, aneurysm size, and pulmonary infection were found to be the important risk factors for the final outcome among the elderly. In addition, age and aneurysm size were also associated with poor outcome in patients with UIAs under conservative observation. Age would affect the treatment and prognosis of intracranial aneurysm in elderly patients. Individuals older than 75 years have an increased risk of aneurysm development 21 . Based on patient age, we often choose different treatments for intracranial aneurysm, and prognosis also varies due to different ages. For example, for patients less than 50 years old, surgical clipping of UIAs has been shown to prevent hemorrhage during the first year post-surgery and improve survival; however, among patients over 65 years old, surgical clipping resulted in a high rate of disability and mortality 22 , and the rate of complications during the perioperative period also increased with age 23 . However, our results showed that open surgery for intracranial aneurysms in elderly patients could also achieve good outcome. Therefore, in our opinion, advanced age should not prohibit aneurysm clipping for elderly patients. In addition, larger aneurysm size would increase the rate of aneurysm rupture. Jabbarli et al. performed a retrospective study about the predictors and clinical impacts in patients with aneurysm with SAH and found that larger aneurysm size was a main risk factor for occurrence of aneurysmal intraventricular hemorrhage and associated with poor prognosis 24 . General complications, such as heart dysfunction and pneumonia, often accompanied the procedure during the perioperative period. A recent study demonstrated that pneumonia is associated with poor physical quality of life one year after SAH 25 . In our study, we also found no significant association between unfavorable outcome and pneumonia, but heart dysfunction was related to poor outcomes for intracranial aneurysm in elderly patients who received aggressive therapy. Therefore, increased attention to perioperative airway nursing and heart function protection may help patients achieve better outcomes. Although the natural history of UIAs in the elderly was still not well understood, some previous literature has demonstrated that aneurysm size and age were significant risk factors for aneurysm rupture and poor outcome 19,26,27 , which was similar to our result. Therefore, elderly patients with risk factors for aneurysm rupture should undergo aggressive treatment to avoid unfavorable outcomes.
Several limitations of this study should be addressed. Our data were retrospectively collected and patients were not treated in a randomized manner. Therefore, a potential selection bias might affect the outcomes of patients treated by different methods. The other limitation is the small size of this cohort, especially of the clipping group. Thus, a large prospective randomized study should be arranged in the future to offer a more accurate “real-world” perspective on this issue.
Conclusion
Although limitations exist, this study provides some useful data on the management of elderly patients with intracranial aneurysms. Based on our findings, we conclude that endovascular coil embolization and clipping are both safe and effective treatment methods for intracranial aneurysms in elderly patients. Elderly patients with UIAs should be treated based on careful evaluation. Aggressive therapy for UIAs in elderly patients with risk factors for aneurysm rupture should be considered positively.
Supplemental Material
Supplementary_table_1 - Treatment Strategy for Unruptured Intracranial Aneurysm in Elderly Patients: Coiling, Clipping, or Conservative?
Supplementary_table_1 for Treatment Strategy for Unruptured Intracranial Aneurysm in Elderly Patients: Coiling, Clipping, or Conservative? by H. Yang, H. Jiang, W. Ni, B. Leng, X. Bin, G. Chen, Y. Tian and Y. Gu in Cell Transplantation
Footnotes
Acknowledgements
Author contribution: conception and design: YG and HY. Analysis and interpretation of data: WN, BL, BX, GC, and YT. Drafting the article: HY and HJ. All authors critically revised the article, reviewed the final version of the manuscript, and approved it for submission. HY and HJ are co-first authors; they contributed equally to the work. Supplemental material for this article is available online.
Author Contribution
H. Yang and H. Jiang, equal contribution on this work as the co-first authors.
Ethical Approval
The study was approved by the Ethics Committee of Huashan Hospital (Shanghai, China).
Statement of Human and Animal Rights
This study was carried out according to the ethical standards of the Ethics Committee of Huashan Hospital (Shanghai, China).
Statement of Informed Consent
All patients provided written informed consent to participate in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: the study was supported by grants National 973 Programs (2014CB541604-LFZ), National Natural Science Foundation of China (NSFC) (81500987, 81771237, 81801155, and 81870917) and Science and Technology Commission of Shanghai Municipality (STCSM) (15140902300).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.