
Abstract
Human amniotic membrane (hAM) is the innermost layer of fetal membranes, which surrounds the developing fetus and forms the amniotic cavity. hAM and hAM-derived cells possess many properties that make them suitable for use in regenerative medicine, such as low immunogenicity, promotion of epithelization, anti-inflammatory properties, angiogenic and antiangiogenic properties, antifibrotic properties, antimicrobial properties, and anticancer properties. Many pathological conditions of the urinary tract lead to organ damage or complete loss of function. Consequently, the reconstruction or replacement of damaged organs is needed, which makes searching for new approaches in regenerative and reconstructive urology a necessity. The use of hAM for treating defects in kidneys, ureters, urinary bladder, and urethra was tested in vitro in cell cultures and in vivo in mice, rats, rabbits, cats, dogs, and also in humans. These studies confirmed the advantages and the potential of hAM for use in regenerative and reconstructive urology as stated above. However, they also pointed out a few concerns we have to take into consideration. These are (1) the lack of a standardized protocol in hAM preparation and storage, (2) the heterogeneity of hAM, and especially (3) low mechanical strength of hAM. Before any wider use of hAM for treating urological defects, the protocols for preparation and storage will need to be standardized, followed by more studies on larger animals and clinical trials, which will altogether extensively assess the potential of hAM use in urological patients.
Introduction
Regenerative medicine is an interdisciplinary approach that applies principles and methods of engineering, biology, and medicine toward replacing, engineering, or regenerating human cells, tissues, or organs to restore or establish normal function 1 –4 . Three different methodological approaches can be distinguished: (1) cell-based therapy, (2) the use of biomaterials or acellular scaffolds, and (3) cell-seeded scaffolds 3,5 . The cells can be from autologous, allogenic (same species, different individual), or heterologous (different species) origin 3 . Numerous scaffolds have been used in attempts to regenerate different tissues and organs in the body. The most important considerations in designing scaffolds are (1) biocompatibility, (2) biodegradability, (3) suitable mechanical properties, (4) scaffold architecture, and (5) manufacturing technology 2 . Human amniotic membrane (hAM) and hAM-derived cells (human amniotic epithelial cells [hAECs] and human amniotic mesenchymal stromal cells [hAMSCs]) fit the listed criteria and are already used in clinic, especially hAM is most widely used in ophthalmology (as a graft to treat epithelial damage or as a bandage to cover the ocular surface to promote healing) 6 –9 and dermatology (to treat burns, chronic ulcers, epidermolysis bullosa, and Stevens-Johnson syndrome) 10,11 . There are currently 105 clinical trials registered on the NIH Clinical Trials website (https://clinicaltrials.gov) that are using hAM and hAM-derived cells in running, although to the best of our knowledge, none in the field of urology (Clinical Trials, 2017). However, we believe that hAM and hAM-derived cells would also be suitable for use in regenerative and reconstructive urology.
Structure and Biological Properties of the hAM
hAM is the innermost layer of fetal membranes, which surround the developing fetus and form the amniotic cavity. hAM is normally 0.02 to 0.5 mm thick 7,12,13 and it consists of a monolayer of hAECs, the basal lamina, and avascular stroma. Avascular stroma is composed of the compact layer, hAMSC layer, and spongy layer (Fig. 1) 14,15 .

Structure of human amniotic membrane (hAM). hAM consists of human amniotic epithelial cells (hAECs), basal lamina, and hAM stroma contains human amniotic mesenchymal stromal cells (hAMSCs) and is divided into 3 layers: the compact layer, the hAMSC layer, and the spongy layer.
Pluripotent stem cells are self-renewing cells, capable of differentiating into all 3 germ layers of the developing embryo—ectoderm, mesoderm, and endoderm. A range of assays can be employed to assess the pluripotency: (1) in vitro differentiation, (2) teratoma formation, (3) chimaera formation, (4) germ line transmission, (5) tetraploid complementation, and (6) single-cell chimaera formation 16 . While all of these methods have their advantages and disadvantages, we believe the best way to assess the pluripotent nature of cells is by combining several of these methods 16,17 . hAMSCs and hAECs have been shown to express pluripotent markers and are capable of differentiation into cells of all 3 germ layers in vitro. Additionally, in vivo experiments have been performed in mice, but teratoma formation was not demonstrated 18 –21 . To the best of our knowledge, other methods have not been used to assess the pluripotent potential of hAM-derived cells. Therefore, hereafter, we use the term “pluripotent hAM-derived cells” with this in mind.
hAECs are cuboidal cells that form a monolayer on the basal lamina and are in contact with the amniotic fluid. On the cell surface, they express several antigens, such as ATP-binding cassette transporter G2 (ABCG2/BCRP), E-cadherin, integrins α6, β1, c-met (hepatocyte growth factor [HGF] receptor), CD10, CD13, CD24, CD29, CD44, CD49e, CD73, CD90 (Thy-1), CD105, CD166, and stromal cell surface marker (STRO-1) 18,20,22 –25 . Expression of pluripotent markers was detected in hAECs, namely, all hAECs express stage-specific embryonic antigen 4 (SSEA-4), but only a subpopulation of the hAECs express pluripotent stem cell antigens Tra1-60 and Tra1-81 26,27 and octamer-binding protein 4 (OCT-4) 28 . hAECs also express sex determining region Y (SRY)-related HMG-box gene 2 (SOX-2) and Nanog 20,23 . The hAMSC layer consists of a mixture of amniotic mesenchymal stromal cells (CD34+) and the mature mesenchymal stromal fibroblasts (CD34−) 29,30 . On the cell surface, they both express CD29, CD44, CD73, CD90, CD105, and epidermal growth factor receptor (EGFr). Amniotic mesenchymal stromal cells (CD34+) also express CD117, CD133, CD146, CD201, Globo H, and pluripotency markers, such as SSEA-1, SSEA-3, SSEA-4, SOX-2, OCT-3, OCT-4, Nanog, Krüppel-like factor-4, and REX-1 19,23,26,31 –33 . A minor fraction (less than 10%) of the mature mesenchymal stromal fibroblasts (CD34−) express CD117, CD133, CD146, CD201, SSEA-1, SSEA-3, and Globo H as well. A part of the CD34− stromal fibroblast population also express SSEA-4 (less than 15% of the cells), Nanog (35% of the cells), and OCT-3 and OCT-4 (45% of the cells). hAM-derived cells are capable of adipogenic 18,33,34 , chondrogenic 18 , osteogenic 19,33 –35 , skeletal myogenic 33,34 , angiogenic 33 , hepatic 20,21,36,37 , neurogenic, 18,21,35 pancreatic 34,36 , and cardiomyogenic 36 differentiation 23,24,38 . However, even though the pluripotent potential of hAM-derived cells has been described, their potential for differentiation into urothelial cells has not yet been explored and determined. Pluripotent cells present a powerful resource for application in regenerative medicine. Since extracellular matrix together with the paracrine effect of the surrounding tissue plays a key role in regulating cell behavior and consequent differentiation of pluripotent cells, we presume that placing hAM-derived cells in the patient would result in differentiation of hAM-derived cells into targeted tissue at the site of damage 39 –41 . hAM-derived cells, together with beneficial properties of hAM as a scaffold, would provide a favorable environment for regeneration of targeted tissue.
Low Immunogenicity
hAECs and hAMSCs express low to moderate levels of major histocompatibility complex class I (MHC1) molecules—human leukocyte antigen (HLA), including antigens Ia (HLA-A, B, C) and Ib (HLA-G, E). Moreover, they do not express (or express only very low levels of) HLA II class molecules (HLA-DP, -DQ, -DR) and costimulatory molecules (CD80, CD86) on the cell surface. These properties of hAM decrease the possibility of transplant rejection, which is an important advantage when choosing materials for use in regenerative medicine 42,43 .
Anti-inflammatory Properties
hAM-derived cells have anti-inflammatory properties—they suppress the proliferation of T lymphocytes, induce T regulatory lymphocytes, influence antigen-presenting cells (APCs) by blocking maturation of monocytes into dendritic cells, and inhibit migration of macrophages and natural killer (NK) cells 8,44 –49 . They also produce many anti-inflammatory factors, such as hyaluronic acid, interleukin-10 (IL-10), indoleamine 2,3-dioxygenase (IDO) enzyme, transforming growth factor β (TGF-β), hepatocyte growth factor (HGF), and prostaglandin E2 14,44,47,50,51 , and reduce the expression of type 1 helper cells (Th1) inflammatory cytokines. Additionally, hAMSCs secrete factors that impact peripheral blood monocytes by switching the differentiation of classical pro-inflammatory/activated M1 macrophages into the M2-like anti-inflammatory/regulatory macrophages and also enhance anti-inflammatory profile of regulatory M2 macrophage–like cells 52,53 . This effect is very beneficial in regenerative medicine, since it improves tissue regeneration and repair 52,54 .
Angiogenic and Antiangiogenic Properties
hAM has angiogenic and antiangiogenic properties. hAM excretes angiopoietin-2, IL-8, IL-6, epidermal growth factor (EGF), basic fibroblast growth factor (bFGF), heparin-binding EGF, HGF, platelet-derived growth factor (PDGF), placental growth factor, and vascular endothelial growth factor (VEGF), which promote angiogenesis 55,56 . hAM also excretes antiangiogenic factors, for example, pigment epithelium-derived factor (PEDF), tissue inhibitors of metalloproteinase 1, 2, 3, 4 (TIMP-1, TIMP-2, TIMP-3, TIMP-4), and thrombospondin-1 56 –59 . Niknejad et al. showed that epithelial side of hAM (amniotic epithelial cells facing up) inhibits angiogenesis, while the mesenchymal side of hAM (mesenchymal/stromal side of hAM facing up) increases angiogenesis 60 . Integration of the implanted graft with host vasculature is of the utmost importance for successful engraftment 61 . Therefore, while hAM can promote angiogenesis, one must also pay attention to the correct orientation of hAM to achieve the desired effect.
Promotion of Epithelization
hAM promotes epithelization by excreting EGF, IL-8, insulin-like growth factor 1 (IGF-1), PDGF bFGF, HGF, TGF-β, and other factors that support epithelization and differentiation of different cells. 62 –64 Molecules of hAM extracellular matrix, such as fibronectin, laminin-1, laminin-5, collagen type-I, III, IV, V, and VII, also promote cell adhesion and migration 65,66 . Since epithelization is an essential mechanism of wound healing and tissue regeneration, promotion of epithelization is an important characteristic of hAM 67 .
Antifibrotic Properties
hAM reduces the risk of scarring and adhesion due to secretion of TIMP-1, -2, -3, and -4, which reduce proteases’ activity on the site of application (e.g., reduction of proteinase activities in the cornea, which may induce irreversible stromal deconstruction) 68 . Additionally, hAM has an antifibrotic effect on biliary fibrosis induced in rats, where the antiscarring action of hAM is a result of anti-inflammatory action (suppression of IL-1, IL-6, IL-8, and inflammatory cells) and antiscarring action of hAM stroma (suppression of TGF-β) 69,70 . Furthermore, hAMSC, when injected into the spleen of injured mice, can engraft into the injury site, ameliorate liver fibrosis, and restore liver function 30 . Additionally, hAM also decreases scarring in treatments of wounds and burns 10,71 . Scar formation is a tissue’s normal response to injury or disease and scar tissue is often formed at the expense of normal tissue regeneration 72 . Therefore, to promote healing and normal tissue regeneration, the antifibrotic properties of hAM are very beneficial.
Antimicrobial Properties
hAM has antimicrobial activity in vivo. King et al. and Buhimschi et al. reported that hAECs express natural antimicrobials, such as human β-defensins, elafin, and secretory leukocyte protease inhibitor in vivo 73,74 . Kim et al. showed that histones H2A and H2B, which possess antimicrobial and endotoxin-neutralizing activity, were localized in the cytoplasm and also on the extracellular surface of hAECs 75 . Additionally, hAM has also antiviral activity, since cDNA for cystatin E was found in hAECs 76 . Since bacterial infections inhibit the process of wound healing and tissue regeneration 77 , antimicrobial properties are a valuable characteristic of hAM.
Anticancer Properties and Nontumorigenicity
hAECs and hAMSCs or their conditioned medium (culture medium, which was in contact with hAM or hAM-derived cells during culture) are capable of inducing apoptosis in several cells lines (HeLa cervical cancer cells, MDA-MB-231 breast cancer cells, hepatocarcinoma cancer cells HepG2, Hep3B2.1-8, HuH7) 78,79 and animal models (breast tumor in BALB/C nu mice, glioma in BALB/C mice, and hepatocarcinoma in BALB/C nu/nu mice) 80,81 . Magatti et al. have shown that hAMSCs induce the cell cycle arrest of hematopoietic and nonhematopoietic cancer cells in coculture by inhibition of positive regulators of the cell cycle (cyclins, cyclin-dependent kinases, mini-chromosome maintenance complex, proliferating cell nuclear antigen) and upregulation of cell cycle inhibitors (cyclin G2, CDK inhibitor 1A, CDK inhibitor N2B). Additionally, Cullin-1 (mediator of ubiquitination and degradation of several proteins, including p21) and RB-1-like protein (p107) are downregulated and retinoblastoma protein (pRB) is upregulated. Consequently, this leads to cell cycle arrest of cancer cells in the G0/G1 phase and prevention of cell cycle progression to S phase 82 . Additionally, treatment of cancer cells with hAM-conditioned medium leads to inhibition of heat shock protein 90, which triggers apoptosis, inhibition of angiogenesis, and cell cycle inhibition 83 . hAM also reduces metabolic activity of prostate, breast, colon, hepatocarcinoma, pancreatic, bile ducts, endometrial, bladder, esophagus cancer cells, osteosarcoma, and melanoma 84 . Inhibition of angiogenesis by hAECs contributes to inhibition of tumor growth as well 60 . While tumorigenicity is a main concern of using stem cells for therapeutic purposes, in vivo teratoma formation and tumorigenicity of hAM-derived cells per se have not been reported 20,80 .
Two major advantages of using hAM in regenerative medicine are also its accessibility and the fact that the use of hAM is ethically acceptable, since placenta is usually disposed of after birth. Moreover, we believe that as our knowledge of the properties of hAM cells and extracellular matrix improves, we may discover even novel indications for the use of hAM-based therapies in the treatment of urological diseases and other diseases or wounded and inflammatory conditions.
Structure and Biological Properties of the Urinary Tract
Urinary tract is divided into (1) upper urinary tract, consisting of kidneys and ureters, and (2) lower urinary tract, consisting of urinary bladder and urethra. Although each organ of the urinary tract has distinct anatomic features, they all have one feature in common—transitional epithelium (urothelium), which covers the inner surfaces of the renal pelvis, ureter, bladder, and proximal part of the urethra 85 (Fig. 2). Blood–urine barrier, which is the tightest and most impermeable barrier in the body, is formed during differentiation of urothelial cells from the basal to the superficial cell layer. Superficial urothelial cells are adapted to maintain a permeability barrier between urine and blood, which protects the blood from toxic urinary substances 85,86 . Congenital disorders, trauma, inflammatory lesions, iatrogenic injuries, and malignancies can lead to organ damage or complete loss of function. Consequentially, reconstruction or replacement of the damaged organs is needed. Shortage of organ donations, implanted tissue rejections, and complications due to use of nonnative tissues make searching for new approaches in reconstructive urology a necessity 87,88 .
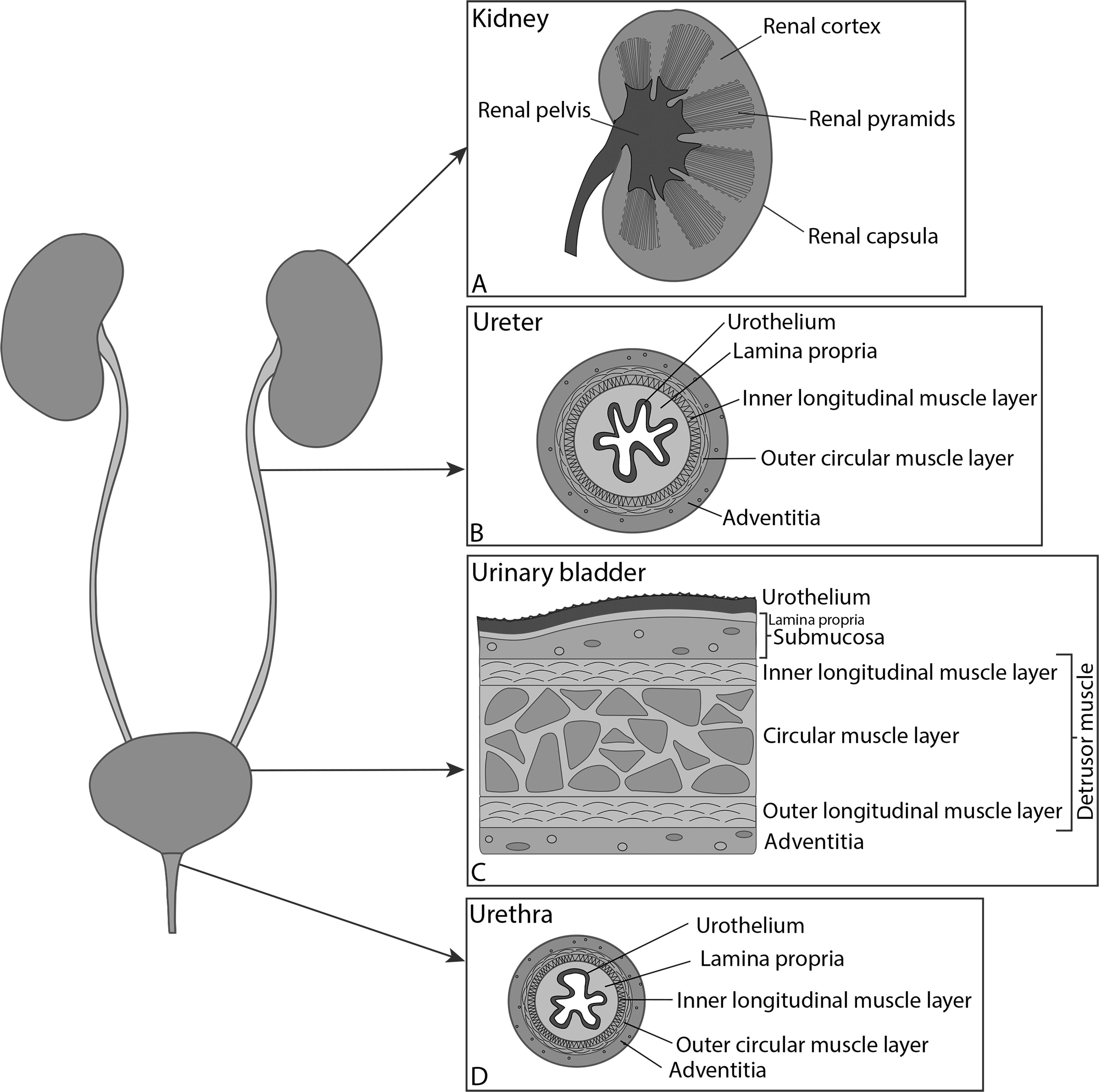
Scheme of the urinary tract: (A) kidney, (B) ureter, (C) urinary bladder, and (D) urethra. Urothelium covers the inner surface of the renal pelvis, ureters, urinary bladder, and the proximal part of the urethra, while the distal part of the urethra is covered with stratified columnar epithelium.
Use of hAM in Regenerative Medicine for the Urinary Tract: Current Situation and Future Prospects
Kidneys
Kidneys are crucial for purifying toxic metabolic waste products from the blood. Under normal conditions, the epithelial turnover of the kidney is slow, but an acute injury can rapidly trigger extensive cellular proliferation and induce repair 89 . Since mammalian adult kidneys are not capable of de novo nephrogenesis, renal cells need to be recovered upon kidney injury to avoid nephron loss and renal atrophy 90 . Nonetheless, the innate ability of the kidney to repair itself is limited and reaches a barrier when faced with repetitive episodes of injury or chronic damage. The latter results in interstitial fibrosis and parenchymal loss 89 . However, if kidney structure is completely disrupted, the only cure might be allogenic transplantation or the development of a functional whole kidney de novo 91 (Fig. 2A).
Kidney diseases pose a global health problem, with very high incidence that continues to rise 89 . Consequentially, new therapeutic approaches are needed in dealing with kidney disease, and since hAM promotes epithelization, reduces scarring and fibrosis, and also has low immunogenicity, it has the potential to be used in treating kidney disease.
Currently, there is only one record of using hAM (Fig. 3A) for treating renal injuries. Erdener et al. (1990) used fresh hAM for repair of severe renal injuries in albino rats. They made incisions extending from the hilum to the lateral edge of the kidney, and immediately after trauma wrapped the injured kidneys in a circular sheet of hAM. The control group received no surgical treatment. After 30 d, there were no significant differences in renal function between the treated and nontreated groups; however, there were significant histological differences. The nontreated group showed defects, the kidneys were irregular in shape, the healed lacerations were deep and wide, and most of them contained hematoma. In the treated group, there were no signs of perirenal fibrosis or hematoma and the renal capsule was thin and regular. The scars were thin and healed well 92 . Although significant differences in renal function between the treated and nontreated groups were not evident, we believe that a lack of fibrosis or hematoma in the treated group is of greater importance. Renal scarring leads to renal function deterioration 93 , and to ensure long-term recovery, circumvention of scarring is necessary. Since inflammation and immune system activation have been identified as a common underlying mechanism for chronic and acute renal diseases 94 , anti-inflammatory and antiscarring properties make hAM a very appropriate candidate for use in regenerative medicine.

Different scaffolds of human amniotic membrane (hAM). (A) hAM: The scaffold consists of human amniotic epithelial cells (hAEC), basal lamina, and hAM stroma. (B) dAM (denuded hAM): hAECs were removed from hAM before the application. (C) sAM (stroma hAM): hAM is oriented with hAM stroma facing the site of the application. (D) Folded hAM: hAM was folded in half with hAECs facing outside. (E) Multilayered hAM: Four hAM were stacked into multilayered hAM and dried. (F) hAM + PLCL: The sandwich-structured biocomposite, constructed from hAM, covered from both sides with a 2-layered poly(
Many studies suggest that bone marrow–derived mesenchymal stem cells (BM-MSCs) are able to ameliorate tissue damage in response to kidney injury and to reduce allograft rejection. However, such beneficial effects are mostly attributable to their immunomodulatory capacity and the release of paracrine factors (growth factors, e.g., HGF, IGF-1, VEGF, EGF) 89,95 –97 . Additionally, their use is restricted due to low content of stem cells in bone marrow, prolonged time of in vitro expansion, and patient discomfort during bone marrow aspiration 88 . Like BM-MSCs, hAMSCs also have anti-inflammatory properties and they too excrete various growth factors, such as HGF, EGF, keratinocyte growth factor, and bFGF 98,99 . Moreover, unlike other stem cells, hAM-derived cells could also be used in cell-based therapies with fewer safety concerns and ethical issues. Vidane et al. (2016) have used amniotic mesenchymal stromal cells isolated from cat amniotic membrane, which they administered intravenously into 9 cats with chronic kidney disease (2 × 10 6 cat amniotic mesenchymal stromal cells suspended in 3 to 4 mL of normal saline via intravenous infusion, 21 d apart). They have shown significant improvement in the renal function (decrease in serum creatinine and urine protein concentrations and increase in urine specific gravity), although the kidney architecture and morphology did not change after treatment 100 . The results of this study are promising and the potential of hAMSCs for the treatment of kidney diseases should be further investigated.
Ureter
Ureters are slender tubes that convey urine from the kidneys to the urinary bladder (Fig. 2B). Damaged ureters are a consequence of an injury or a pathologic condition that may result in stricture formation, urolithiasis, or chronic inflammation 101 . Most ureteral injuries are induced by a surgeon, medical treatment, or diagnostic procedures. They are often underreported, possibly due to a lack of early recognition or short-term postoperative follow-up 102 . In addition to iatrogenic injuries, trauma can also result in ureteral damage. Several techniques to repair the long ureteral defects have been introduced, such as a Boari flap, psoas hitch, transureteroureterostomy, and ileal interposition. They are not always applicable and they too carry their own risks for complications, for example, recurrent strictures, urinary leakages, metabolic complications, and donor tissue harvesting problems 103 . Due to limitations and complication rates that traditional surgical procedures pose, new therapeutic approaches are needed in ureteral surgery.
The ideal material for ureter reconstruction should be easily accessible, impermeable for urine, nonimmunogenic, should guarantee future remodeling, and should also possess appropriate conditions for cell growth and migration. 103 –105 Very few studies have been performed in the field of ureteral tissue engineering. Most of them focused on using different scaffolds, such as tubular(ized) small intestinal submucosa (SIS) without cellular preseeding 106 –108 , collagen 109,110 , and Gore-Tex 111,112 . In general, collagen and SIS, but not Gore-Tex, were capable of facilitating some degree of urothelium and smooth muscle regeneration; however, fibrosis occurred in most cases 113 . Since hAM is easily accessible, is low immunogenic, promotes epithelization, decreases fibrosis, and also promotes cell growth and migration 114 , we believe it would make a suitable scaffold for ureter regeneration and reconstruction.
Koziak et al. used hAM for reconstructive surgery of the ureteral obstruction in 11 patients with extensive ureteral strictures. hAM was first deeply frozen for preservation and radiation-sterilized (35 kGy). Before implantation, the hAM was thawed and folded with hAECs facing outside (Fig. 3D). The ureter was incised longitudinally without intersecting and then the ureteral wall defect was covered with hAM in an on-lay fashion, followed by sewing in the implant. A JJ catheter was used as a ureteral stent to bridge the reconstructed segment for 3 weeks following the procedure. The follow-up was at 3, 9, and 24 mo following intervention, and it included excretory urography and ultrasound. The procedure was successful in all patients, the only complications included 1 stricture recurrence and 2 cases of an isolated, symptomatic urinary tract infection 115 . This is a very important study, because it is the only one so far in which the use of hAM was tested in a larger number of patients. The greatest shortcoming of hAM is its mechanical fragility.
Since most early studies in ureteral tissue engineering used bare scaffolds and almost all of them resulted in fibrosis, this may indicate the necessity of cell seeding 106 –112 . Studies show that hAM is an appropriate scaffold for epithelial cells 114,116 and not only that hAM promotes epithelization, cell proliferation, and migration, it also has an antifibrotic effect 69 . The listed properties would contribute to better epithelization and reduce the number and extent of complications. Consequentially, hAM would be an appropriate scaffold for ureteral tissue engineering.
Urinary Bladder
The main function of the urinary bladder is the storage of urine. It consists of 4 distinct layers: urothelium, submucosa, detrusor muscle, and adventitia (Fig. 2C). Conditions such as vesical exstrophy, neurogenic bladders, contracted bladder, and urothelial carcinoma make it necessary to find new approaches for surgical reconstruction of the bladder 88 . Currently, the gold standard technique for bladder augmentation is enterocystoplasty, which consists of removing a gastrointestinal segment and using it for a bladder replacement or repair. Due to the difference in function of gastrointestinal tissue compared to bladder tissue, multiple complications may occur, such as infection, metabolic disturbance, urolithiasis, perforation, increased mucus production, and malignancy 117 –119 .
Many different approaches have been used in bladder reconstruction, based on the use of unseeded and cell-seeded scaffolds and/or stem cells, but unfortunately the current knowledge of bladder reconstruction is insufficient to use it as a clinical standard 87,88 . Biomaterials used for bladder reconstruction should be easily manipulated into a hollow, spherical configuration, and they should be able to biodegrade for complete tissue development and mimic the ability of the extracellular matrix to regulate differentiation, cell division, and apoptosis 120,121 . hAM can be easily manipulated and is able to biodegrade 29,122 , and since hAM’s extracellular matrix, that is, macromolecular components and local mediators (growth factors, etc.), promotes cell adhesion and growth 29 , we believe hAM could be a suitable scaffold for bladder regeneration and reconstruction.
Iijima et al. performed bladder augmentation in rats using fresh hAM (Fig. 3A). The experimental animals, female Sprague Dawley rats, were divided into 3 groups regarding the procedure used: (1) partial cystectomy and augmentation with hAM, (2) partial cystectomy and augmentation with SIS, and (3) partial cystectomy with primary closure. In the first 2 groups, a small piece of omentum was placed on top of the bladder to cover the graft. At 1, 3, or 6 mo postoperatively, urinary bladders were removed and analyzed. Three main findings for bladders augmented with hAM were made: (1) regeneration of nerve fibers in all 3 (mucosal, muscular, and serosa) layers of the bladder wall, (2) in vitro regenerated bladder strips exhibited contractile responses to a muscarinic receptor agonist and to electrical intramural nerve stimulation, and (3) such bladders displayed competent bladder capacity and compliance. However, 42% of the 31 rats with hAM augmentation and 33% of the 27 rats with SIS augmentation died postoperatively. The main cause of death in the hAM- and SIS-augmented groups was uremia, resulting from massive urinary leakage into the peritoneal cavity. This problem may have arisen mainly because of the difficulty of suturing in a watertight fashion in a rat model 123 , which may not be so problematic when suturing larger organs, for example, in the bladder augmentation in humans using hAM. However in that case, some other complications connected with mechanical strength, inadequate or absent innervation, and vascularization might arise.
A similar study was performed by Shakeri et al., who tested whether hAM (Fig. 3A) could be used for bladder reconstruction and replacement in dogs. Twelve cross hybrid dogs underwent partial cystectomy and augmentation with a 4 cm × 4 cm fresh hAM or only subsequent closure (controls). Fresh hAM was harvested from a healthy human placenta 3 to 12 h prior to surgery. Surgery was completed successfully. Gravity cystograms were performed at 3 and 6 wk postoperatively, and the bladder appearance showed no evidence of vesicoureteral reflux or diverticula. One animal died 7 d postoperatively, due to urinary leakage into the peritoneal cavity, which was a result of a hole in the central part of the hAM. At 6 wk postoperatively, the degree of adhesions between the bladder wall and bowel was minimal in all but 2 dogs in the testing group, which showed moderate inflammation and adhesion. The ureter and upper urinary tract were normal in all animals. The mucosa covering the scaffold was normal, but the bladder wall in the hAM scaffold area was thinner than the normal bladder wall. Histologic examination of 6 animals showed evidence of complete regeneration of the bladder mucosa with urothelium, the reconstitution of a normal lamina propria, and neovascularization, but no ingrowth of the bladder muscle cells. The histologic examinations of other 3 animals showed significant, but not complete healing. Control bladders showed intact urothelium and thick muscle layer 124 . Although the mucosa regeneration was indeed promising when using hAM for bladder augmentation, the follow-up period was only 6 wk, which leaves us to questioning whether this period was too short to enable the regeneration of all bladder layers.
Low strength and overall fragility of hAM are one of few reservations we have in mind when considering the use of hAM in regenerative medicine. Due to low mechanical strength of hAM, Adamowicz et al. prepared an hAM-based biocomposite, where frozen hAM was thawed and then reinforced with electrospun nanofibers. The sandwich-structured biocomposite material was constructed from frozen hAM and covered from both sides with a 2-layered poly-(
Recently, Barski et al. published a study in which they examined the possibility of bladder reconstruction with the multilayered hAM (Fig. 3E) in a xenograft rat model. They used hAM, which was stored at −20 °C for 24 h before use. After defrosting in water, sterilization in peracetic acid, and alcohol mixture for 2 h on the shaker, hAMs were rinsed. Then 4 hAMs were stacked into multilayered hAM and dried under laminar flow (Fig. 3E). Twenty-seven male Sprague Dawley rats were anesthetized and a midline laparotomy was performed. After evaluation of bladder capacity and pressure, a 0.5 cm lesion was cut at the bladder dome. In the treated group (n = 18), the multilayered hAM graft was used to seal the lesion, while in the first control group (C1; n = 6), the defect was closed with a suture and fibrin glue, and in the second control group (C2; n = 3), the multilayered hAM graft was sutured to the intact bladder wall. The animals were sacrificed at 1, 3, and 6 wk after surgery, the bladder capacity was determined, and the specimens were prepared for histological and immunohistochemical analysis. Two animals of the treated group died (one due to postoperative sepsis and the other during anesthesia), while no animals from control groups died and no other severe complications higher than grade II (Clavien-Dindo classification) were observed. The bladder capacity did not change in the treated group, but it did reduce significantly in the C1 control group. After 1 wk, the signs of inflammation were present and meso-adhesions to the hAM graft were detected in most of the treated cases, but the inflammation was less prominent in the control groups. After 3 wk, the inflammation was significantly reduced, the adhesions were still present in some cases, and new capillaries started to grow into surrounding connective tissue and scattered smooth muscle cells appeared. After 6 wk, the slight inflammation was still present, periamniotic vascularization increased, and connective tissue, bundles, and thin muscle layers were abundantly found in all groups. No shrinkage of the hAM grafts or signs of rejection were detected in any of the specimens. The authors describe no signs of leakage and believe that the multilayered hAM is elastic and durable enough for the reconstruction of small defects 126 .
Since the main function of the urinary bladder is the storage of urine with potentially noxious levels of urea, ammonia, and other toxic metabolites for prolonged periods of time, the maintenance of the blood–urine barrier is crucial 127,128 . For this reason, use of scaffolds, which enable and promote the proliferation and differentiation of highly specialized superficial urothelial (umbrella) cells, is necessary 129,130 (Fig. 4). Our group already performed an in vitro study, which showed that hAM is a suitable scaffold for urothelial cells, since it promotes their proliferation and differentiation. Moreover, hAM enables the development of a normal urothelium with molecular and ultrastructural properties comparable to that of native urothelium 114 . Additionally, urinary bladder must be able to endure considerable changes in volume of the organ. Therefore, good mechanical properties are vital when choosing a biomaterial for urinary bladder reconstruction. While Iijima et al. and Shakeri et al. report a good regeneration of the mucosa, they face the same pivotal problem—the fragility of hAM. Adamowicz et al. and Barski et al. have recently successfully overcome this challenge by reinforcement of hAM with PLCL and by using multilayered hAM, respectively. We believe that by achieving good mechanical properties of hAM, the hAM is a very good candidate for applications in regenerative medicine of the urinary bladder.

Histology of the urinary bladder. (A) Porcine urinary bladder, which is histologically similar to normal human urothelium. The analysis of porcine urinary bladder was approved by the Veterinary Administration of the Slovenian Ministry of Agriculture and Forestry in compliance with the Animal Health Protection Act and the Instructions for Granting Permits for Animal Experimentation for Scientific Purposes. Urothelium is marked with a dotted square. Scale bar 100 µm. (B) The scheme of the urothelium: Urothelium is composed of superficial (umbrella), intermediate, and basal urothelial cells.
Urethra
The urethra is a tubular structure composed of multiple layers of tissues—epithelium, which is urothelium in the proximal part and nonkeratinized stratified squamous epithelium in the distal part of urethra, lamina propria, muscular layer, and adventitia 88 (Fig. 2D). It functions as a channel permitting the passage of urine out of the bladder 131 .
Urethral reconstruction due to urethral injury, long-distance urethral stricture, hypospadias, or epispadias continues to be a challenge for urologists. There are more than 300 techniques implemented for urethral stricture and hypospadias repair 132 , which illustrates the complexity of these conditions and also a lack of a perfect procedure. The availability of appropriate tissue poses a large challenge, since substitutes such as (vascularized) skin grafts, bladder, and buccal mucosa have limitations compared to the urethral tissue 133 . Complications such as stricture formation or graft failure can arise due to these limitations, and consequentially, there is a need for alternative materials for urethral reconstruction 134 .
The ideal engineered urethral substitute should not undergo contraction, fibrosis, or rejection after implantation. The scaffold should be impermeable, easily obtainable, cheap, and have good handling characteristics 131 . Two types of scaffolds have been used for urethral reconstruction: (1) cell-free (acellular) scaffolds, obtained from cadaveric sources and (2) scaffolds, containing living autologous cells, obtained from biopsy. The choice of the best scaffold varies between individual clinical situations, for example, short primary bulbar strictures may be treated with acellular scaffolds or anastomotic urethroplasty, while the longer strictures are best treated by cellularized scaffolds 131 . Since hAM is easily obtainable, reduces the risk of scarring and fibrosis, and is also low immunogenic, we believe it would make a suitable scaffold for urethra regeneration and reconstruction.
Another aspect one has to keep in mind when choosing an appropriate scaffold for regeneration of the urethra is the anatomy and histology of the human urethra. While the female urethra is shorter (3.8 to 5.1 cm) and covered with urothelium, the male urethra is longer (15 to 29 cm, the mean urethra length is 22.3 cm) and only the proximal part is covered with urothelium. The distal part is covered with nonkeratinized stratified squamous epithelium 135 . Consequently, when choosing the scaffold for tissue regeneration of the whole male urethra, it is necessary to select the scaffold that enables the growth and differentiation of both epithelia.
Shakeri et al. tested application of hAM as xenograft for urethroplasty in rabbits. They used hAM preserved in glutaraldehyde (0.6%). In the first 2 animals, the hAM scaffolds (Fig. 3A) were put on the distal part of the urethra, but the rabbits easily removed them, probably due to irritation of the catheter in the meatus. In the remaining rabbits, 5 mm × 10 mm hAM scaffolds were put on the ventral surface of the urethra mucosa. The operation was successful in all 20 rabbits. After 30 d, all animals were checked for urethral fistula and urethral diameters were evaluated. There were no intraoperative complications. One animal developed an infection 1 wk after the surgery, but despite the treatment with a second antibiotic, a fistula formed later. All histological samples revealed complete epithelization of reconstructed urethra by nonkeratinized stratified squamous epithelium, without any inflammation or tissue loss. Histopathologic changes showed a thin-walled urethra with no definite muscle layer. There was only vascular proliferation and fibrosis suggestive of regeneration 136 . The largest shortcoming of this study is the lack of a control group. Although the results of epithelial regeneration are promising, we should keep in mind that the hAM scaffolds were used to correct a urethral defect in normal urethra with good surrounding tissue and not to correct urethral strictures. The results showed no muscle layer regeneration, which again leaves us to questioning whether this could be attributed to a short follow-up time.
Wang et al. performed a similar study in which they tested the use of different scaffolds of hAM, specifically hAM, dAM, and cell-seeded dAM (Fig. 3), for urethral reconstruction in rabbit urethral injury models. First, to obtain dAM, amniotic epithelial cells were removed from hAM by incubation with 0.02% ethylenediaminetetraacetic (EDTA) acid at 37 °C for 2 h. Then dAM and hAM were freeze-dried and sterilized by irradiation (25 kGy) 137 . Twenty male New Zealand white rabbits were used in the experiments, 4 of them underwent subcutaneous implantation of dAM (n = 4) and another 4 of hAM (n = 4). In the follow-up studies, no serious inflammation or rejection was observed in the cell-seeded dAM group, while the accumulation of CD4+ and CD8+ cells in the dAM group indicated an inflammatory response. The others were segregated into 2 groups for urethral reconstruction surgery—the experimental group received cell-seeded dAM (n = 6; Fig. 3G) and the control group received intact hAM scaffolds (n = 6; Fig. 3A). Mucous membrane (4 mm × 3 mm) was harvested from the posterior wall of the rabbits’ urethra, then the epithelium layer was separated from the mucous membrane and cut into pieces, followed by digestion. Cell suspension was collected and the cells were cultured for 3 to 5 passages. To obtain cell-seeded dAM, dAM was seeded with 10 5 epithelial cells/mL, which were dripped on the surface of dAM placed in a petri dish. The cell-seeded dAM was cultured for 2 wk. Briefly, during the surgical procedure for creating the urethral injury model and urethroplasty, a 5 mm × 10 mm defect was made and covered with hAM or cell-seeded dAM. Two wk and 3 mo after surgery, implants in the rabbits were collected for histological examination. The rabbits behaved normally during the 3-mo follow-up examination. One rabbit developed serious infection and another was found with fistula in the group that received hAM. Neither infection nor fistula was observed in the group with cell-seeded dAM implantation. Three months after surgery, the urethral defect was completely repaired in the cell-seeded dAM group and the formation of a smooth muscular layer and rich blood vessels were apparent 116 .
Two studies, which tested the use of hAM for reconstructing urethra, were performed in the clinic. Brandt et al. investigated the use of hAM grafts in 8 female patients with urological congenital defects. They reported the procedure was quick and effective for appropriate restoration of the function and the cosmetics of the lower urogenital tract 138 . The second study was performed by Koziak et al. who used hAM for treatment of recurring strictures of urethra in 2 males. They covered the whole length of strictured segment with hAM, and 3 mo after the surgery, the follow-up procedures showed wide urethra lumen and graft, covered with epithelium. No scarring was observed 139 . Since hAM is known to promote epithelization and reduce fibrosis, the studies showed that hAM would be a suitable scaffold for urethra regeneration as it was anticipated. Nevertheless, the same reservations concerning mechanical properties of hAM persist also in the case of urethral reconstruction. After overcoming challenges concerning the mechanical properties, we believe that hAM could be used as one of the most appropriate scaffolds for urethral reconstruction. Moreover, new studies should also clearly show and determine which epithelium (urothelium or nonkeratinized stratified squamous epithelium) is regenerated. Currently, in most studies, these data are missing.
What Kind of hAM Would Make the Best Scaffold?
hAM has many properties that make it suitable for use in regenerative medicine. Characteristics of hAM such as promotion of epithelization, cell adhesion and migration, low immunogenicity, anti-inflammatory properties, and reduction of fibrosis are very advantageous when choosing a hAM scaffold for tissue engineering or as a scaffold per se for use in regenerative medicine. However, there are also a few disadvantages of hAM: (1) lack of a standardized protocol in hAM preparation and storage, (2) heterogeneity of hAM, and (3) low mechanical strength of hAM (Table 1). Lack of a standardized protocol prevents a thorough analysis of hAM’s potential for use in regenerative medicine; since due to different gestation ages, protocols of hAM preparation and storage, low number of studies, and diverse experimental designs, we cannot draw solid conclusions about the best way for preparation and preservation of hAM without changing its vital properties. The span of variability in hAM preparation and storage procedures in the case of studies, examining the potential of hAM use in reconstructive and regenerative urology, is demonstrated in Table 2. Heterogeneity of hAM is also a challenge, since hAM differs from one donor to another and there is also variability between different regions of hAM 140 . Another big challenge is hAM’s fragility. To make it applicable for use in regenerative medicine, it will be necessary to improve its mechanical resistance without affecting other hAM properties. Good examples of improvement in hAM mechanical properties were reported by Adamowicz et al., who prepared a hAM-based biocomposite where hAM was reinforced with electrospun nanofibers 125 , and by Barski et al., who used a multilayered hAM 126 .
Overview of Advantages, Disadvantages, and Challenges of hAM’s Use in the Regenerative and Reconstructive Urology.

Abbreviation: hAM, human amniotic membrane.
Overview of hAM Preparation and Storage Procedures Used in Studies, Examining the Potential of hAM Use in the Reconstructive and Regenerative Urology.

Abbreviations: cAM, cat amniotic membrane; cAMSC, cat amniotic mesenchymal stromal cells; dAM, denuded human amniotic membrane; DMSO, DMSO, dimethyl sulfoxide; FBS, fetal bovine serum; hAM, human amniotic membrane.
Interestingly, in vivo studies included only the use of hAM and dAM, but none of them tested the effect of hAM stroma (sAM) on urothelial cells. An in vitro study performed by our group showed that hAM scaffolds enable the development of tissue-engineered urothelium with molecular and ultrastructural properties comparable to that of native urothelium 114 . We studied growth and differentiation of normal porcine urothelial (NPU) cells on 3 different hAM scaffolds. We used hAM, which was cryopreserved at −80 °C in Eagle’s medium and glycerol (volume ratio 1:1). NPU cells were seeded on (1) the epithelium of hAM (Fig. 3A), (2) the basal lamina of hAM (denuded hAM [dAM]; Fig. 3B), and (3) the hAM stroma (sAM; Fig. 3C) and cultured for 3 wk. Unexpectedly, the fastest growth and the highest differentiation of NPU cells was achieved on sAM scaffold, where the superficial NPU cells were the largest and they displayed molecular (uroplakins, occludin) and ultrastructural properties (urothelial plaques, microridges, well-developed tight junctions, and lateral membrane overlaps) of superficial NPU cells in highly differentiated urothelia. Since hAECs acted as a physical barrier, NPU cells’ growth was the slowest when the cells were seeded on the epithelium of hAM scaffold and therefore also their differentiation was at the time of analysis still lower than on the sAM and dAM scaffolds. Even though the fastest growth and the highest differentiation of NPU cells were expected on dAM scaffold, our findings demonstrated only the establishment of the urothelium with partially differentiated superficial NPU cells 114 . This study shows that the scaffold’s orientation and topography have an immense impact on the characteristics of the scaffold. Similarly, Niknejad et al. showed that angiogenic and antiangiogenic effects of hAM are side-dependent. While the epithelial side of hAM inhibits angiogenesis, the latter is promoted by the mesenchymal side of hAM 60 . Slow or insufficient vascularization of tissue-engineered grafts is one of the major limiting factors toward their clinical implementation 141 , and therefore, angiogenic properties of hAM are very important. Findings of these studies emphasize the importance of the orientation and the manner of preparation of hAM, which should be well thought over to achieve the desired results.
Research on potential use of stem cells in regenerative medicine is peaking, but urology is somewhat behind other specialties when it comes to stem cell research 142 . Only a few studies exploring the potential value of stem cell therapy in urology have been performed and they included studies of bladder dysfunction, erectile dysfunction, stress urinary incontinence, and prostate and bladder cancer. Despite the favorable results, clinical applications of stem cells in urology are limited mainly due to poor differentiation of the cells and inflammation-mediated graft rejection 143 . To the best of our knowledge, studies of hAM-derived cells’ differentiation to urothelium have not yet been published, but it has been confirmed that they are capable of differentiation toward endodermal, mesodermal, and ectodermal lineages 23 . Among other advantages of use of hAM-derived cells are also their anti-inflammatory properties, nontumorigenicity, and lack of ethical concerns, since placenta is usually disposed of after birth.
In conclusion, hAM and hAM-derived cells show a great potential for use in regenerative medicine and a small number of performed studies offer a good starting point for further research. However, before broader use of hAM and hAM-derived cells in urology, there is an urgent need for standardization of procedures for preparation and storage, followed by additional studies on larger animals (to overcome difficulties with handling hAM in surgical procedures) and clinical trials (in human allogen settings to also explore immunological hAM impact), which will assess the potential of hAM use in urological patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Slovenian Research Agency (Grant No. P3-0108, J3-7494, and Young Researchers Program).