
Abstract
The effect of adipose tissue-derived stem cells (ASCs) in combination with heparin transplantation on acute liver failure mice with carbon tetrachloride (CCl4) injection was investigated. CCl4 is a well-known hepatotoxin and induces hepatic necrosis. Heparin did not affect the viability of ASCs for at least 24 h. The injection of heparin into the caudal tail vein decreased slightly the activities of the alanine aminotransferase (ALT), asparate aminotransferase (AST), and lactate dehydrogenase (LDH) in plasma. In the transplantation of ASCs (1 × 106 cells) group, there was a trend toward decreased activities of all markers. However, four out of six mice died of the lung infarction. In the transplantation of ASCs in combination with heparin group, there was also a trend toward decreased activities of all markers. In addition, all mice survived for at least the duration of the study period. In conclusion, the transplantation of ASCs in combination with heparin was thus found to effectively treat acute liver failure.
Introduction
Many of the liver diseases caused by toxic injury, virus infections (32), malignant transformation, and inborn genetic deficiencies (31) lead to hepatocyte dysfunction, resulting in acute or chronic liver failure. These diseases are very difficult to cure. At present, liver transplantation is still the only effective therapy for treating these patients. However, this treatment has many problems, such as insufficient donors, high expense, and surgical damage (36). Recently, cell transplantation therapy has developed into an alternative therapy to whole organ transplantation, because it is a minimally invasive method with fewer potential complications. Petersen et al. (24) first showed that liver stem cells might be derived from the bone marrow in a rat model of liver injury and later many reported similar results (2,12,21,30,37). The replacement of diseased hepatocytes by stem cells or the stimulation of endogenous as well as exogenous regeneration by stem cells is the primary mechanism of liver-directed cell therapy. Therefore, cell transplantation therapy using stem cells is an attractive method for the treatment of patients with severe liver disease (36).
Mesenchymal stem cells (MSCs) are detected in multiple tissues, including bone marrow, umbilical cord blood, periodontal ligament, and adipose tissue. Bone marrow has a multipotent population of cells capable of differentiating via a number of mesodermal pathways (31). Bone marrow-derived stem cells (BMSCs) have the capacity to differentiate into multiple mesenchymal cells such as cardiomyocytes, chondrocytes, osteoblasts, and adipocytes (6,10,13). Therefore, BMSCs have been considered to be an important source of stem cells for cell transplantation therapy. Clinical studies have evaluated the use of BMSCs in regenerating the myocardium and vessels in patients with heart failure and those with limb ischemia (8,34,35,41). Murine and human BMSCs have been reported to develop into hepatocyte-like cells in vitro and in vivo (4,5,9,14,30). However, there remains controversy regarding whether BMSCs can differentiate into hepatocytes.
Recently, ASCs have been identified as an alternative source of BMSCs, because adipose tissue is easer to obtain in abundance through minimally invasive harvest procedures such as lipoaspiration with local anesthesia (38). ASCs, similar to BMSCs, not only possess the ability to self-renew and differentiate into various mesenchymal cell types but also secrete significant levels of many potent growth factors and cytokines, including vascular endothelial growth factor (VEGF) and hepatocyte growth factor (HGF) (7,11,19,26). In addition, ASCs can be easily transduced by virus vectors such as retrovirus, adenovirus, and Sendai virus (25,43). Based on these studies demonstrating the ability of ASCs, ASCs have been focused on as a new cell source for cell transplantation therapy against liver failure. In addition, heparin enhances hepatic regeneration and minimizes hepatic fibrogenesis caused by chronic carbon tetrachloride (CCl4) treatment. The mechanism underlying these effects most likely involves both the upregulation of HGF and the inhibition of HSC proliferation (1,17).
The most important step in developing a new cell transplantation therapy using ASCs is assessing the effectiveness for liver disease. The purpose of this study was to investigate whether transplanted ASCs in combination with heparin could attenuate CCl4-induced acute liver failure with a significant improvement in specific biochemical liver failure markers.
Materials and Methods
Animals
C57BL/6 mice were purchased from SLC Japan. The mice were housed in a controlled environment (12-h light/dark cycles at 21°C) with free access to water and a standard chow diet before killing. All conditions and handing of animals in this study were conducted with protocols approved by the Nagoya University Committee on Animal Use and Care.
Isolation and Culture of Mouse Adipose Tissue-Derived Stem Cells (ASCs)
ASCs were collected from 7-14-week-old female C57BL/6 mice. The mice were killed by cervical dislocation and the adipose tissues in the inguinal groove were isolated and washed extensively with Hank's balanced salt solution or phosphate-buffered saline (PBS) to remove blood cells. The isolated adipose tissues were cut finely and digested with 1 ml of 1 mg/ml type I collagenase (Collagenase Type I, 274 U/mg, Koken Co., Ltd., Tokyo, Japan) at 37°C in a shaking water bath for 90 min. Adipose tissue cells were filtered using 250-μm nylon cell strainers (BD Biosciences) and suspended in Dulbecco's modified Eagle's medium (DMEM)/F12 containing 20% fetal bovine serum (FBS; Trace Scientific Ltd., Melbourne, Australia, Uin: 53141, Lot: B01249-500) and 100 U/ml penicillin/streptomycin. The cells were centrifuged at 1,200 rpm for 5 min at room temperature and the pellet contained ASCs. The cells were washed three times by suspension and centrifugation in the culture medium and incubated overnight at 37°C with 5% CO2 in culture medium (DMEM/F12, 20% FBS, and 100 U/ml penicillin/streptomycin). The primary cells were cultured for 4–5 days until they reached confluence and were defined as passage 0. The passages of cells used in experiments were between passages 2 and 5.
Adipogenic Differentiation
Adipogenic differentiation was induced by culturing the cells for 3 days in DMEM (high glucose) containing 100 μM indometacin, 1 μM dexamethasone, 1 μM hydrocortisone, 10 μM insulin (Sigma, I-5500), and 10% FBS. The cells were cultured further in DMEM (high glucose) containing 10% FBS for 2 weeks and the medium was changed every 3 days. Differentiation was confirmed by microscopic observations of intracellular lipid droplets and Oil Red O staining as an indicator of intracellular lipid accumulation. Briefly, the cells were fixed in 10% solution of formaldehyde in PBS for at least 10 min at room temperature and washed with 60% isopropanol. The cells were then stained with 2% (w/v) Oil Red O reagent for 10 min at room temperature followed by repeated washing with distilled water and destaining in 100% isopropanol for 1 min.
Osteogenic Differentiation
Osteogenic differentiation was induced by culturing the cells for 2 weeks in DMEM containing 200 μM dexamethasone, 50 μM ascorbate-2-phosphate (Wako Pure Chemical Industries Ltd., 013-12061), 10 mM α-glycerophosphate (Sigma, G-9891), and 10% FBS and the medium was changed every 3 days. The differentiation was confirmed by an examinations of the extracellular matrix calcification using Von Kossa's method. The cells were washed twice with PBS and fixed in 10% formalin for 15 min at room temperature. They were washed and incubated with deionized water for 15 min. Thereafter, they were stained with a solution containing naphthol AS MX-PO4, N,N-dimethylformamide, Red Violet LB salt, and Tris-HCl (pH 8.3) for 45 min. Von Kossa staining was carried out with 2.5% silver nitrate solution for 30 min.
Cytotoxicity of Heparin in ASCs
ASCs (1.5 × 104 cells) were seeded in each well of a 96-well plate (BD Biosciences) with 100 μl of culture medium for 2 h and were confirmed to adhere to the plate bottom. The medium was replaced with 150 μl of DMEM/F12 containing 2% FBS and 1.25, 2.5, 5.0, and 10.0 μl of heparin solution (Mochida Pharmaceutical; 10,000 U/10 ml) and were incubated at 37°C. After 24 h, the viable cells were counted using Cell Counting Kit-8 (CCK-8; Dojindo Laboratories, Kumamoto, Japan). CCK-8 reagent (10 μl) was added into each well and the reaction was allowed to proceed for up to 4 h. The absorption of the sample at 450 nm was measured against a background control, using a microplate reader.
Transplantation of ASCs Into C57BL/6 Mice
To generate a liver damage group, 6-week-old male C57BL/6 mice were injured by an IP injection of 0.5 ml/kg of CCl4 and divided into four groups (six mice each). After 4 h, transplantation was conducted as follows: 1) saline (150 μl) as a positive control (described as mice treated with CCl4 alone), 2) saline (150 μl) containing 5 μl of heparin (described as mice treated with heparin alone), 3) ASCs (1 × 106 cells) suspended in 150 μl saline (described as mice treated with ASCs alone), and 4) ASCs (1 × 106 cells) suspended in 150 μl saline containing 5 μl of heparin (described as mice treated with ASCs + heparin). These cells were thereafter slowly injected into the caudal tail vein of mice using 27-gauge needles and a Terumo syringe. A negative control group of C57BL/6 mice that had not been treated with CCl4 was also used. After 20 h, the mice were sacrificed and blood samples were collected. In addition, internal organs such as the liver and lung were collected.
Liver Failure Marker Production
The alanine aminotransferase (ALT), asparate aminotransferase (AST), and lactate dehydrogenase (LDH) levels in plasma were evaluated using the Japan Society of Clinical Chemistry (JSCC) method. These were performed by the SRL Communication for Health Company, Tokyo, Japan.
Statistical Analysis
Statistical analysis was performed using SPSS for windows, version 14.0. For multiple group analysis, homogeneity of variance was assessed by the Leneve test. Parametric comparisons used analysis of variance (ANOVA). If ANOVA was significant, significances of individual differences were evaluated by using the Bonferroni test.
Results
Isolation of ASCs and Model of ASCs Transplantation Into C57BL/6 Mice
ASCs were harvested from adipose tissue in the inguinal region of 7–14-week-old female C57BL/6 mice. Some cells from the adipose tissue adhered to the bottom of the culture flask and exhibited a fibroblastic shape. They proliferated quickly in the culture medium and reached a uniform confluent cell monolayer (Fig. 1A-a) and differentiated into adipocytes and osteocytes (Fig. 1A-b, A-c). These data suggest that the harvested cells were ASCs.
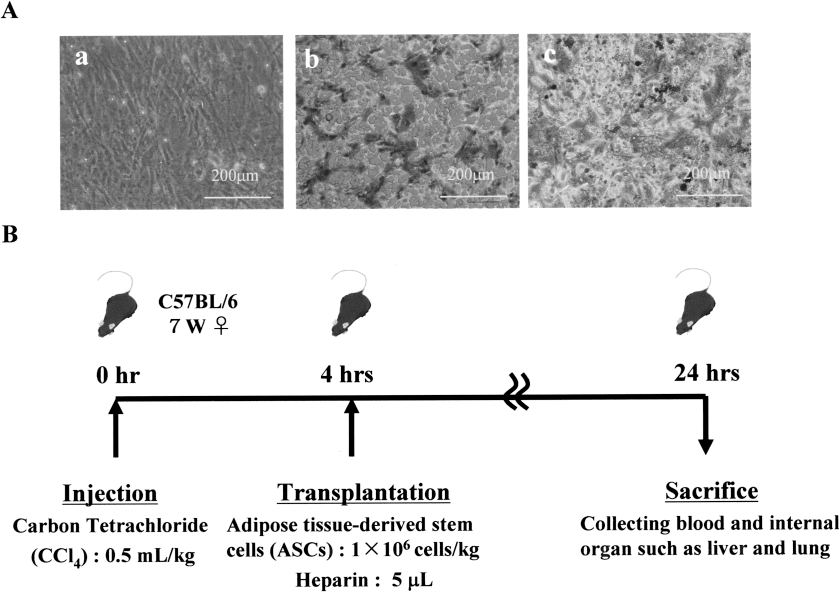
Morphology and staining after differentiation into adipogenic and osteogenic cells by ASCs, and the scheme of the experimental protocol. (A) Morphology of ASCs used in this experiment (a). Adipogenic differentiation of ASCs confirmed by the presence of intracellular lipid vesicles staining for Oil Red O (b). Osteogenic differentiation of ASCs confirmed by Von Kossa's staining (c). (B) Time schedule of the experimental protocol used to induce acute liver failure.
The ASCs (1 × 106 cells) were transplanted into 6-week-old male C57BL/6 mice injured by injection of 0.5 ml/kg of CCl4 4 h before transplantation. After 20 h, the mice were sacrificed and serum samples were collected. In addition, internal organs such as the liver and lung were collected (Fig. 1B).
Cytotoxicity of Heparin in ASCs
The general usage of heparin for humans (in the case of 60 kg of body weight) for 1 day is 10 ml of heparin solution (10,000 U/10 ml). The mice body weights were about 20–30 g, so the use of heparin for a mouse (assuming 25 g of body weight) was estimated to be approximately 5 μl.
To examine the cytotoxicity of heparin in ASCs, the cells were incubated in a 96-well plate with 150 μl of DMEM/F12 containing 2% FBS and 1.25, 2.5, 5.0, and 10.0 μl of heparin for 24 h (Fig. 2) at 37°C and the viability of the ASCs was measured with the method already described. The levels were approximately 100% and nearly identical. There was no significant difference in ASCs incubated for 24 h at all concentrations. Moreover, no differentiation or abnormality was confirmed by the addition of heparin (data not shown). These data suggested that heparin at these concentrations did not affect the viability of ASCs.
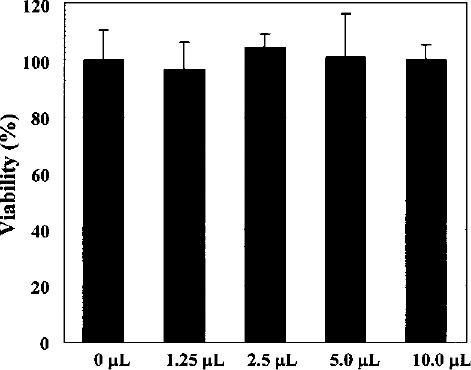
Cytotoxicity of heparin in ASCs. This graph shows that the viability of ASCs (1.5 × 104 cells) incubated with 150 μl of DMEM/F12 containing 2% FBS and 0, 1.25, 2.5, 5.0, and 10.0 μl of heparin for 24 h. The level of 0 μl of heparin was converted to 100%, and other levels were obtained. The data show the average of the results from three assays. Bars indicate standard deviation.
Comparison of Liver Failure Marker Production After Transplantation
CCl4 is a well-known hepatotoxin and induces hepatic necrosis. As shown in Figure 3, after CCl4 injection for 24 h, the activities of plasma ALT, AST, and LDH were increased, in comparison to the negative control group. The injection into the caudal tail vein of heparin slightly decreased the activities of all markers, but no significant reduction was confirmed. Next, in the injection of ASCs (1 × 106 cells) group, there was a trend toward the activities of all markers. However, four out of six mice died within 20 h (Fig. 4). In the injection of ASCs (1 × 106 cells) in combination with heparin group, there was also a trend towards the decreased activities of all markers. In addition, all mice injected ASCs in combination with heparin survived for at least the duration of the study period (Fig. 4). The data were analyzed for statistical significance using the Bonferroni test.

Levels of production of liver failure markers such as ALT, AST, and LDH after transplantation. (A) The plasma alanine aminotransferase (ALT) activity after transplantation [heparin, ASCs (1 × 106 cells), and ASCs in combination with heparin, respectively] after intoxication with carbon tetrachloride (CCl4). (B) The plasma asparate aminotransferase (AST) activity. (C) The plasma lactate dehydrogenase (LDH) activity. Blood samples were evaluated using the Japan Society of Clinical Chemistry (JSCC) method. Bars indicate standard deviation.

Comparison of the survival rate between ASCs and ASCs in combination with heparin transplantation. The dashed line shows the survival rate of ASCs only transplantation and indicates that approximately 66% of mice were dead by the end of the study period. Continuous line shows the survival rate of ASCs in combination with heparin transplantation, and indicates that all mice survived during the study period.
Injury of Lung and Liver Tissue After ASCs Transplantation
Four out of six mice died following the injection of only ASCs (1 × 106 cells) and some died vomiting blood. To investigate the cause of death, the mice were sacrificed and their tissue specimens were compared to normal tissue specimens. As shown in Figure 5C and D, infarction of the lung tissue was observed and, in some mice, deterioration of the liver tissue was also observed. On the other hand, in the group treated with ASCs (1 × 106 cells) in combination with heparin, all of the mice survived and no change in the lung or liver was observed (Fig. 5E, F).
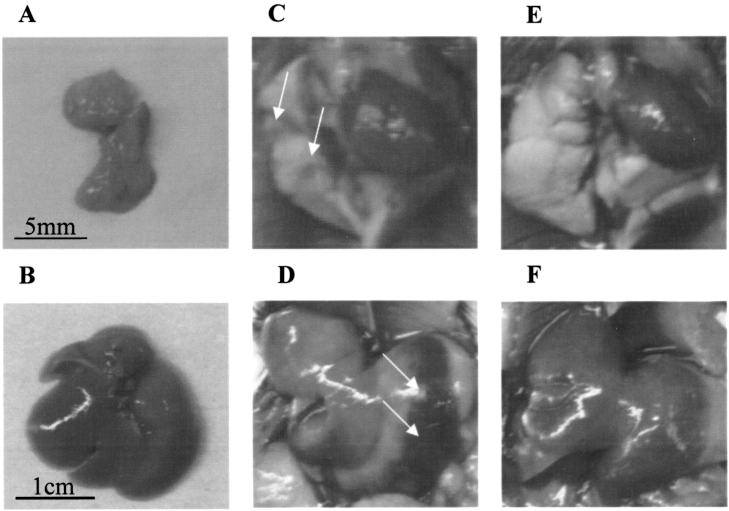
Lung and liver alterations after transplantation of ASCs and ASCs in combination with heparin. (A, B) Normal lung (A) and liver (B) in 6-week-old male C57BL/6 mice. (C, D) The lung (C) and liver (D) in C57BL/6 mice injected with ASCs (1 × 106 cells) only suspended in 150 μl saline. The positions of the alterations are indicated by arrows. (E, F) The lung (E) and liver (F) in C57BL/6 mice injected with ASCs (1 × 106 cells) suspended in 150 μl saline containing 5 μl of heparin. No alterations were observed in all areas.
Discussion
This report investigated the effect of ASCs transplantation on acute liver failure in mice. Although some studies have shown that MSCs including ASCs transplantation are effective in chronic liver failure, the effect on acute liver failure is not well known. In acute liver failure, numerous fresh stem cells are immediately required for transplantation therapy. Therefore, ASCs are thought to be appropriate therapy for acute liver failure, because the cells are easer to obtain in abundance through minimally invasive harvest procedures such as lipoaspiration with local anesthesia (38).
In the ASCs (1 × 106 cells) injection group, there was a trend toward decreased the activity of all markers. These data suggested that ASCs might have therapeutic potential for the treatment of acute liver failure. However, the injection of ASCs only led to the infarction of the lung, and four out of the six mice died. These results may have been caused by the low mobility of ASCs, because no death caused by BMSCs transplantation has been previously reported. Therefore, a combination of ASCs and heparin was used.
Heparin is generally used as an anticoagulant agent. Recently, some studies have shown that heparin forms a hetetodimer and induces a significant increase in serum HGF levels, thus resulting in accelerated hepatocyte proliferation and regeneration (15–18,20,23,28). Besides, heparin also participates in the regulation of many cellular processes, such as cell growth and differentiation, by stimulating the production and increasing the concentration of several growth factors in the blood. Moreover, dalteparin sodium, a low molecular weight heparin, enhances hepatic regeneration and minimizes hepatic fibrogenesis caused by CCl4 treatment (1).
In this study, the injection of 5 μl of heparin (0.2 U/kg) into the caudal tail vein decreased slightly the activity of all liver failure markers, but no significant reduction was observed. The heparin dose necessary to achieve this effect is variable, but generally a single dose of 300–1000 U/kg of body weight suffices (20). In comparison, this study used a smaller amount of heparin. The smaller amount is good for clinical application and the general usage of heparin for human (in the case of 60 kg of body weight) at 1 day was 10 ml of heparin solution (10,000 U/10 ml). However, in the injection of ASCs (1 × 106 cells) in combination with heparin group, there was a trend toward decreased the activity of all liver failure markers. In addition, all mice injected with ASCs and heparin survived for at least the duration of the study period (Fig. 4) and no change was confirmed in the lung and liver tissues of these mice (Fig. 5). These data suggest that the mobility of ASCs is improved by the addition of heparin. On the other hand, the ALT level was increased in comparison to the level obtained with ASCs only injection. This observation also may be due to the mobility of ASCs.
BMSCs and ASCs are multipotent cells and can be induced to differentiate into various cell types of mesodermal tissues including bone, cartilage, fat, tendon, and bone marrow stroma (22). Moreover, these cells have also been reported to differentiate into ectodermal cells, such as neural cells (29,42) and into endodermal cells, such as hepatocyte-like cells (31,33). On the other hand, other studies have shown that cellular fusion occurred in the presence of a proliferation stimulus in conjunction with impaired intrinsic liver regeneration capacity (3,39,40). It was reported that mice with BMSCs transplants with continuous CCl4 injection had reduced liver fibrosis and a significantly improved survival rate in comparison to mice treated with CCl4 alone (27). In this study, the mechanism of improved liver functions may be due to cytokine production such as hepatocyte growth factor (HGF) from transplanted ASCs and/or cell fusion rather than transdifferentiation from ASCs into hepatocytes, because the transplanted ASCs are unlikely to differentiate into hepatocytes within 24 h and a large amount of ASCs had migrated into the lung tissue, whereas few ASCs had migrated into the liver (data not shown). Therefore, the alteration of lung tissue was due to infarction, while that of the liver tissue may be a secondary change (due to lung failure) rather than infarction (Fig. 5). It is necessary to verify the mechanism of this treatment and the adequate dose of heparin in further studies.
Footnotes
Acknowledgment
We thank the Kobayashi Pharmaceutical Co., Ltd and Rina Yokota (Nagoya University) for their assistance.