
Abstract
Somatic stem cells can be isolated from a variety of sources. Although some studies have suggested that somatic stem cells may represent a cell population that is very similar to embryonic stem (ES) cells, it remains unclear whether somatic stem cells retain the potential to differentiate into any cell type derived from the three germ layers. In this study, we investigated the transdifferentiation potential of somatic stem cells using adipose tissue-derived stem/progenitor cells (ASCs; mesodermal stem cells) and pancreatic stem cells (endodermal stem cells). Previous reports from other groups describe the protocol that has been used to differentiate ASCs or mesenchymal stem cells (MSCs) in bone marrow into insulin-producing cells. Induction 1: ASCs were cultured for 3 days in ultra-low attachment plates under serum-free conditions. Induction 2: ASCs were cultured for 24 h with L-DMEM, and reinduced with serum-free H-DMEM for another 10 h. Unlike previous reports, we did not get ASCs to express any pancreas-specific genes, including insulin-1 or insulin-2. Pancreatic stem cells were induced to differentiate into adipo/osteogenic by the following protocols. Induction protocol 1: ACSs were cultured for 7 days with medium containing indometacin, dexamethasone, hydrocortisone, and insulin for adipogenic differentiation. Induction protocol 2: The cells were cultured for 7 days with medium containing dexamethasone, ascorbate-2-phosphate, and β-glycerophosphate for osteogenic differentiation. Although these approaches have been widely used for adipo/osteogenic differentiation from MSCs, adipo/osteogenic differentiation from pancreatic stem cells was not observed. These data suggest that it is not easy for somatic stem cells to transdifferentiate into other germ cell types, at least, under these conditions.
Keywords
Introduction
Stem cells are simply defined as cells that have self-renewing ability and the potential to differentiate into a variety of different lineages. These cells have been subdivided into two groups. The first group consists only of embryonic stem (ES) cells, which are derived from the inner cell mass of the blastocyst and are capable of generating all differentiated cell types in the body (13,41). ES cells in turn generate the second group, which are called somatic stem cells. Somatic stem cells can be isolated from a variety of sources including umbilical cord blood (2), as well as many adult mammalian tissues and organs, such as bone marrow (10,26), liver (26), pancreas (26–29,33), and adipose tissue (24,35,48). Unlike ES cells, these cells have traditionally been thought to be restricted in their differentiation and regeneration potential to the tissues in which they reside (7). Mesenchymal stem cells (MSCs) in bone marrow can be induced in vitro and in vivo to differentiate into various functional cell types of mesodermal tissues including bone, skeletal muscle, cartilage, tendon, fat, and bone marrow stroma (4,10,14,26,37,38). However, recent studies have suggested the possibility that MSCs can differentiate into other germ cell types, such as liver (20) and central nervous system cells (9). It also has been reported that the central nervous system contains stem cells that can differentiate into hematopoietic cells (5) and skeletal muscle cells (15).
The possibility of using stem cells and their more differentiated progenitors to treat numerous degenerative disorders has stimulated great interest in developing safe transplantable sources of stem cells that are unable to form teratomas but able to repopulate damaged tissues (22). Recent investigations have provided interesting clinical findings about the possibility of using MSCs in bone marrow as well as other adult tissue-specific stem cells in genetic and cellular therapies for a wide variety of pathological processes, including degenerative, autoimmune, and genetic diseases (16,36). However, it is not clear, a priori, why bone marrow transplantation should work. This could be due to the presence of multipotential or several types of adult stem cells in donor tissues or, alternatively, to fusion of donor and recipient cells (6). It has been proposed that the bone marrow MSCs transdifferentiate (acquiring broader developmental potential). If true, this is enormously important. It implies that tissue-specific adult stem cells harbor much, if not all, of the potential of ES cells. This would remove the need to collect stem cells from human embryos for clinical purposes, thus overcoming many of the political and ethical barriers to stem cell therapy (45). Several studies, however, raise doubts about whether transdifferentiation actually occurs (40,47). Their data demonstrate that bone marrow cells can fuse spontaneously with other cells and subsequently adopt the phenotype of the recipient cells (3,34,42,43). This finding should be particularly significant when considering recent reports of transplanted bone marrow cells turning into unexpected cell types in vivo. However, it remains unclear whether somatic stem cells retain the ability to transdifferentiate. These attempts have produced controversy.
Although several studies report the ability of bone marrow MSCs to transdifferentiate (11,25), few studies report this ability in other somatic stem cells. In this study, we investigated the ability of somatic stem cells to transdifferentiate using adipose tissue-derived stem cells (ASCs; mesodermal stem cells) (35,48) and pancreatic stem cells (endodermal stem cells) (26,33).
Materials and Methods
Isolation and Culture of Mouse Adipose Tissue-Derived Stem/Progenitor Cells
Subcutaneous adipose tissue was obtained from 8-week-old adult mice (CLEA Japan, Inc. Meguro, Tokyo). Mouse studies were approved by the review committee of Nagoya University Graduate School of Medicine. Adipose tissue (0.5 g) was washed three times with Hank's balanced salt solution, cut finely, and digested with 1 ml of 1 mg/ml type I collagenase (Collagenase Type I, 274 U/mg, Koken Co., Ltd., Tokyo, Japan) for 1 h at 37°C in a water bath with reciprocal shaking. Cells obtained after filtering the digested tissue through 250-μm meshes were suspended in Dulbecco's modified Eagle's medium (DMEM)/F12 containing 20% fetal bovine serum (FBS: Trace Scientific Ltd., Melbourne, Australia, Uin: 53141 Lot: B01249-500) and centrifuged at 1200 rpm for 5 min at room temperature. The sedimentary cell layer was collected. Suspension and centrifugation of the sedimentary cells were repeated three times before culturing.
For the attached culture, 1 × 105 adipocytes (sedimentary cells) were seeded into a T-25 flask (NUNC) with DMEM/F12 containing 20% FBS, 100 U/ml penicillin, and 100 μg/ml streptomycin at 37°C in a humidified atmosphere of 5% CO2. Cells were allowed to attach and spread, and were passaged two to three times.
Adipogenic Differentiation
Adipogenic differentiation was induced by culturing the cells for 1 week in DMEM (high glucose) containing 100 μM indometacin, 1 μM dexamethasone, 1 μM hydrocortisone, 10 μg/ml insulin, and 10% FBS. The cells were cultured further in DMEM (high glucose) containing 10% FBS for 1 week. Differentiation was confirmed by Oil Red O staining of intracellular lipid droplets. For Oil Red O staining, the cells were fixed in a 10% solution of formaldehyde in PBS for at least 10 min, washed with 60% isopropanol, and stained with Oil Red O solution for 10 min followed by repeated washing with water. They were then destained in 100% isopropanol for 1 min.
Osteogenic Differentiation
Osteogenic differentiation was induced by culturing the cells for 1 week in DMEM containing 200 μM dexamethasone, 50 μM ascorbate-2-phosphate, 10 mM β-glycerophosphate, and 10% FBS (17). The differentiation was examined by staining extracellular matrix calcification by von Kossa's method. For von Kossa staining, the cells were stained with a solution containing naphthol AS MX-PO4, N,N-dimethylformamide, Red Violet LB salt, and Tris-HCl (pH 8.3) for 45 min. Von Kossa staining was carried out with 2.5% silver nitrate solution for 30 min.
Induction of ASC Differentiation Into Insulin-Producing Cells (Induction 1)
For induction of differentiation, the cells were seeded at a cell density of 2–3 × 105/well in a six-well plate and cultured for 3 days in ultra-low attachment plates (Vitaris AG, Baar, Switzerland). Differentiation medium consisted of serum-free DMEM/F12 medium with 17.5 mM glucose in the presence of nicotinamide 10 mM, activin-A 2 nM, exendin-4 10 nM, hepatocyte growth factor 100 pM, and pentagastrin 10 nM (all from Sigma, Basel, Switzerland) as well as B-27 serum-free supplement, N-2 Supplement, and 1% penicillin/streptomycin 5000 U/L (all from Invitrogen) (18).
Induction of ASC Differentiation Into Insulin-Producing Cells (Induction 2)
For induction of differentiation, the cells were seeded at a cell density of 2–3 × 105/well of a six-well plate. Cells were cultured for 24 h with predifferentiation medium and reinduced with differentiation medium for another 10 h. Predifferentiation medium consisted of L-DMEM with 10 mmol/L nicotinamide and 1 mmol/L 2-mercaptoethanol (all from Sigma), 1% penicillin/streptomycin 5000 U/L (Invitrogen), and 20% FBS. Differentiation medium consisted of serum-free H-DMEM with 10 mmol/L nicotinamide and 1 mmol/L 2-mercaptoethanol (all from Sigma), as well as B-27 serum-free supplement, 1% penicillin/streptomycin 5000 U/L (all from Invitrogen) (12).
Isolation and Culture of Mouse Pancreatic Islets and Duct Cells
Islets and pancreatic stem cells were isolated from the pancreata of 8-week-old mice (CLEA Japan, Inc.). Mouse studies were approved by the review committee of Kyoto University Graduate School of Medicine and Nagoya University Graduate School of Medicine. For islet isolation, the common bile duct was cannulated and injected with 2 ml cold M199 medium containing 1.5 mg/ml collagenase (30,31). The islets were separated on a density gradient, hand-picked under a dissecting microscope to ensure a pure islet preparation and used immediately afterward.
Pancreatic stem cells (ductal cell morphology) were isolated using a modified islet isolation method. A previous study showed that, after purification on a Ficoll gradient, the top interface (1.062–1.096 density range) was 50–95% islet cells with varying amounts of duct and degranulated acinar tissue; the middle interface (1.096–1.11 density range) contained 1–15% islets, duct, and degranulated acini; and the pellet was mostly well-granulated acinar tissue with less than 1% islets (8). Therefore, the cells in the top and middle layers were used in this study. After hand-picking islets from the top and middle layers under a dissecting microscope, the remaining cells were stained by dithizone, and the remnant islets were deleted. The duct-rich population after islet isolation was then cultured in DMEM with 10% FBS (BIO-WEST, Inc., Logan, UT, S1560 Lot #SO5094S1560). After cells attached and spread, nonductal cells (fibroblast morphology) were removed mechanically with a rubber scrapper. The “duct-like” cells were then inoculated into 96-well plates, cloned by limiting dilution, and cultured in DMEM with 20% FBS.
Induction for Differentiation From Pancreatic Stem Cells Into Insulin-Producing Cells
For inducing cell differentiation into insulin-producing cells, the cells were cultured in DMEM with 10% FBS, 10 nM exendin-4, 10 mM nicotinamide, 10 ng/ml KGF, 100 nM PDX-1 protein, and 100 nM BETA2/NeuroD protein for 7–10 days. For PDX-1 and BETA2/NeuroD protein, the cDNAs were amplified by PCR using appropriate linker-primers and then subcloned into the NdeI and XhoI sites of pET21b(+) (Novagen, Madison, WI) using a ligation kit (TaKaRa, Tokyo, Japan). BL21 (DE3) cells containing the expression plasmids were grown at 37°C to an OD600 of 0.8. Isopropyl-β-D-thiogalactopyranoside was added to a 0.1 mmol/L final concentration, and the cells were then incubated for 12 h at 24°C. Cells were sonicated and the supernatants were recovered and applied to a column of Ni-nitrilotriacetic acid agarose (Invitrogen, San Diego, CA) (28,29,32).
Semiquantitative RT-PCR
Total RNA was extracted from cells using RNeasy Mini Kit (QIAGEN, Tokyo, Japan). After quantifying RNA by spectrophotometry, 2.5 μg of RNA was heated at 85°C for 3 min and then reverse-transcribed into cDNA in a 25-μl solution containing 200 units of Superscript II RNase H-RT (Invitrogen), 50 ng random hexamers (Invitrogen), 160 μmol/L dNTP, and 10 nmol/L dithiothreitol. The reaction consisted of 10 min at 25°C, 60 min at 42°C, and 10 min at 95°C. Polymerization reactions were performed in a Perkin-Elmer 9700 Thermocycler with 3 μl cDNA (20 ng RNA equivalents), 160 μmol/L cold dNTPs, 10 pmol appropriate oligonucleotide primers, 1.5 mmol/l MgCl2, and 5 units AmpliTaq Gold DNA polymerase (Perkin-Elmer, Norwalk, CT). The oligonucleotide primers and cycle number used for semiquantitative PCR are shown in Table 1. The thermal cycle profile used a 10-min denaturing step at 94°C followed by amplification cycles (1 min denaturation at 94°C, 1 min annealing at 57°C, and 1 min extension at 72°C) with a final extension step of 10 min at 72°C. The steps taken to validate these measurements were previously reported (29).
List of Gene-Specific Primers

TaqMan Real-Time PCR
Quantification of insulin mRNA levels was carried using the TaqMan real-time PCR system according to the manufacturer's instructions (Applied Biosystems, Foster City, CA, USA). PCR was performed for 40 cycles, preceded by 2 min at 50°C and 10 min at 95°C as initial steps. In each cycle, denaturation was achieved for 15 s at 95°C and annealing/extension was achieved for 1 min at 60°C. PCR was carried out in 20 μ l of solution using cDNAs synthesized from 1.11 ng of total RNA. Standard curves were obtained using cDNAs generated from total RNA isolated from primary mouse islets. For each sample, the expression of insulin was normalized by dividing by the β-actin expression level. Mouse insulin-2 and β-actin primers are commercially available (Assays-on-Demand Gene Expression Products; Applied Biosystems).
Results
Adipose Tissue-Derived Stem/Progenitor Cells
ASCs were isolated from 8-week-old mice (Fig. 1A). To test whether harvested cells had adipogenic differentiation capabilities, the cells were treated with adipogenic induction media for 1 week and then Oil Red O staining was performed. The cells were positive for Oil Red O staining, suggesting that the cells had adipogenic differentiation capabilities (Fig. 1B). To examine whether the harvested cells had osteogenic differentiation capabilities, the cells were treated with osteogenic induction media for 1 week and then von Kossa staining was performed. The cells were positive for von Kossa staining, suggesting that the cell had osteogenic differentiation capabilities (Fig. 1C). These data suggest that the harvested cells included adipose tissue-derived stem/progenitor cells.
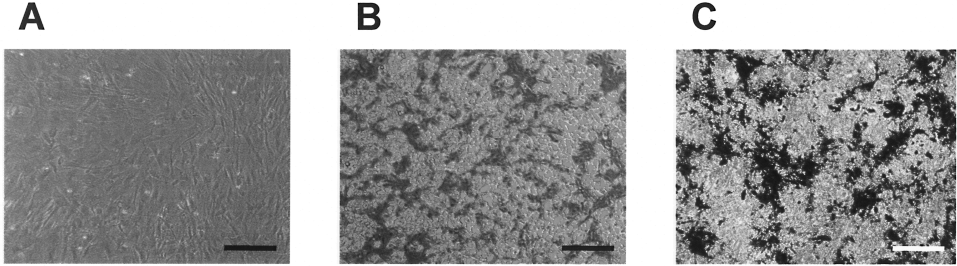
Adipo/osteogenic differentiation of ASCs. (A) Morphology of adipose tissue-derived stem/progenitor cells. (B) Adipogenic differentiation of ASCs. The cell populations were obtained from 8-week-old adult mice. The cells were stained with Oil Red O 1 week after adipogenic induction. (C) Osteogenic differentiation of ASCs. The cell populations were obtained from 8-week-old adult mice. The cells were stained with Von Kossa 1 week after osteogenic induction. Scale bar: 200 μm.
Induction of ASC Differentiation Into Pancreatic β-Cells
To test whether ASCs had the capacity to differentiate into pancreatic β-cells, two different induction protocols that have previously been reported to induce the differentiation into insulin-producing cells from human ASCs (18) or from bone marrow MSCs (12) were performed (Fig. 2B). ASCs formed islet-like clusters after culturing in ultra-low attachment plates using induction protocol 1 (Fig. 2B, left). However, ASCs formed fibroblast-like monolayer that was similar to noninduced ASCs when induction protocol 2 was used (Fig 2B, right). Using semiquantitative RT-PCR, ASCs did not express insulin mRNA using induction protocol 1. Similarly, ASCs did not express insulin mRNA with induction protocol 2. In addition, pancreatic developmental transcriptional factors (such as PDX-1, BETA2/NeuroD, Pax4, Pax6, and Nkx6.1) were not observed in ASCs after either induction method (Fig. 2C). These data suggest that these culture conditions did not induce the differentiation from mouse ASCs into pancreatic β-cells.

Characterization of ASCs after induction into pancreatic β-cells. (A) ASCs were induced using two separate protocols (induction 1 and nduction 2) to facilitate the differentiation of stem/progenitor cells into insulin-producing cells. (B) Morphology of ASCs after induction 1 and induction 2. Scale bar: 200 μm. (C) Expression of pancreas-related genes in ASCs before and after incubation in induction media. The oligonucleotide primers and cycle numbers used for semiquantitative PCR are shown in Table 1. MIN6 cells were used as a positive control.
Pancreatic Stem Cells
Pancreatic stem cells were isolated as previously reported (33). They formed a flat “cobblestone” monolayer (Fig. 3A) that is characteristic of cultured duct cells. To evaluate whether these cells have the same potential as endodermal stem cells (namely, to differentiate into β-islet cells), pancreatic stem cells were cultured with exendin-4, PDX-1 protein, and BETA2/NeuroD protein for 7–10 days. The treated cells induced the expression of the insulin gene (Fig. 3B) and pancreas-related genes (data not shown), suggesting that the cells could differentiate into pancreatic β-cells.

Pancreatic stem cells. (A) Morphology of pancreatic stem cells. Scale bar: 100 μm. (B) Insulin mRNA levels from pancreatic stem cells before and after treatment with induction media. Pancreatic stem/progenitor cells were cultured in DMEM with 10% FBS, 10 nM exendin-4, 10 mM nicotinamide, 10 ng/ml KGF, 100 nM PDX-1 protein, and 100 nM BETA2/NeuroD protein for 7–10 days. The expression of insulin-2 mRNA was measured by real-time PCR. Mouse islets were used as a positive control.
Adipo/Osteogenic Differentiation Capabilities of Pancreatic Stem Cells
To test whether pancreatic stem cells had adipogenic differentiation capabilities, the cells were treated with adipogenic induction media for 1 week and then Oil Red O stained. Pancreatic stem cells were negative for Oil Red O staining, suggesting that the cells did not have adipogenic differentiation capabilities (Fig. 4A). To test whether pancreatic stem cells had osteogenic differentiation capabilities, the cells were treated with osteogenic induction media for 1 week and then von Kossa stained. Pancreatic stem cells did not have osteogenic differentiation capabilities (Fig. 4D). These data suggest that pancreatic stem cells are unlikely to differentiate into mesodermal cell type.

Characterization of pancreatic stem cells after adipo/osteogenic induction. (A, B, C) Adipogenic induction. Pancreatic stem cells (A), ASCs (B; positive control), or MIN 6 cells (C; negative control) were stained with Oil Red O 1 week after adipogenic induction. (D, E, F) Osteogenic induction. Pancreatic stem cells (D), ASCs (E; positive control), or MIN6 cells (F; negative control) were stained with Von Kossa 1 week after osteogenic induction. Scale bar: 200 μm.
Discussion
Somatic stem cells have traditionally been thought to be restricted in their differentiation and regeneration potential to the tissues in which they reside (7). Several studies have suggested that somatic stem cells may represent cell populations very similar to ES cells (44). MSCs have capabilities to differentiate into various functional cell types of mesodermal tissues (10). Several studies indicate the usefulness of multipotential MSCs for tissue engineering purposes in regenerative medicine (22,37). Bone marrow cells have been utilized as a source of MSCs (19). ASCs have bone marrow-like characters (21). Although it has been reported that ASCs differentiate in vitro into not only a mesenchymal lineage to produce adipocytes and osteoblasts (as shown in this study) but also chondrocytes and myocytes (24), hepatocytes (23), insulin-producing cells (18), and neuronal lineage cells (1), our study showed that ASCs do not have the capacity to differentiate into endodermal-derived insulin-producing cells.
We recently established a mouse pancreatic stem cell line (33). The cells could be maintained by repeated passages for more than 1 year without growth inhibition. Moreover, the cells have a potential to differentiate into not only pancreatic β-cells but also α-cells and hepatocytes. Other groups have also shown that pancreatic stem/progenitor cells could differentiate into hepatocytes (39,46). These cells are all derived from the endoderm. As shown in this study, although the induction methods for adipo/osteogenic differentiation are well established, the cells rarely differentiated into adipocytes or osteoblasts. Therefore, pancreatic stem cells have the ability to differentiate into an endodermal cell lineage, although it is hard to get them to transdifferentiate into mesodermal-derived cells, such as adipocytes or osteoblasts.
Recent investigations showed the multipotency of somatic stem cells (6). Other studies have raised doubts about whether transdifferentiation actually occurs (40,47). It is impossible to eliminate multipotency of somatic stem cells for our data. However, these data clearly suggests that transdifferentiation of somatic stem cells is not easy, at least, in these conditions.
Footnotes
Acknowledgments
The authors wish to thank Dr. Carson Harrod for his careful reading and editing of this manuscript and Rina Yokota (Nagoya University) for assistance. This work was supported in part by the Juvenile Diabetes Research Foundation International (JDRFI); the Ministry of Education, Science and Culture, the Ministry of Health, Labour and Welfare; and Baylor All Saints Health Foundation.