
Abstract
Evaluation of engrafted islets mass is important for clinical care of patients after islet transplantation. Recently, we developed the secretory unit of islet transplant objects (SUITO) index, which reflected engrafted islet mass. In this study, we evaluated the SUITO index for the prediction of clinical outcome after single islet transplantation. Single islet transplantations were performed into six type 1 diabetic patients. Isolated islets were quantitatively assessed at the time of transplantation. The SUITO index was calculated as follows: fasting C-peptide (ng/dl)/[fasting blood glucose (mg/dl) – 63] × 1500. Islet yield/recipient's body weight and SUITO index were evaluated, along with HbA1C, relative insulin dose (insulin dose posttransplant/pretransplant), and M-values. HbA1C improved in all cases, irrespective of the SUITO index score or islet yield/body weight. The average SUITO index from postoperative days 3 to 30 (R2 = 0.728, p < 0.04), but not islet yield/body weight (R2 = 0.259, p = 0.303), correlated with relative insulin dose. The daily SUITO index strongly correlated with the daily relative insulin dose (R2 = 0.558, p < 0.0001) and weakly correlated with the daily M-values (R2 = 0.207, p < 0.02). A SUITO index score of less than 10 was associated with increasing insulin dose even after islet transplantation. The SUITO index seems to be a better predictor of success of islet transplantations than islet yield/body weight. SUITO index is recommended to assess clinical outcome of islet transplantation.
Introduction
Pancreatic islet transplantation is a promising treatment for type 1 diabetes (5,15). However, poor long-term insulin independence is currently one of the issues for islet transplantation. After 5 years of islet transplantation less than 10% of patients could maintain insulin independence but more than 70% patients maintained islet function (14,16). The patients with functioning islets could maintain excellent glycemia and, importantly, those patients could have substantial improvement of hypoglycemic episodes, even though insulin injection is necessary. Therefore, the current goal of islet transplantation has shifted from insulin independence to maintaining excellent glycemic control without hypoglycemic unawareness (16).
Recently, we demonstrated that single donor islet transplantation significantly improved glycemic control and reduced the basal insulin requirement (12). Those patients also had substantial improvement in their hypoglycemic episodes (3). In some countries, like Japan, organ donors for islets are extremely low and donor shortage is a serious issue. Therefore, we consider single donor islet transplantation to be an option for the treatment of type 1 diabetes with hypoglycemic unawareness.
Evaluation of the efficacy of islet transplantation is important to follow up the clinical course. Recently, we and others demonstrated that the ratio between fasting C-peptide levels and glucose levels correlated with insulin requirement after islet transplantation (1,4,10,17). We developed a secretory unit of islet transplant objects (SUITO) index, which reflects engrafted islet mass compared to β-cell function in a normal healthy person (4,10). The formula of the SUITO index is as follows: fasting C-peptide (ng/dl)/[fasting blood glucose (mg/dl) −63] × 1500. A SUITO index of 100 reflects 100% pancreatic β-cell function in a healthy person. For example, if the fasting C-peptide level is 0.8 ng/dl and blood glucose is 103, the SUITO index will be 0.8/(103 – 63) × 1500 = 30. The average SUITO index after islet transplantation from postoperative days 3 to 30 was shown to be correlated with insulin reduction (10).
In this study, we examined whether the SUITO index reflected the clinical outcome after single islet transplantation.
Materials and Methods
Pancreas Procurement, Islet Isolation, and Transplantation
Single islet transplantations were performed between March, 2005 and March, 2007 at Baylor University Medical Center (Dallas, TX, USA). The procurement and allocation process of donated pancreata is governed by the United Network for Organ Sharing (UNOS) guidelines and managed locally by the Southwest Transplant Alliance or LifeGift, local organ procurement organizations. In four cases, pancreata were shipped to a remote center and islets were isolated at the remote center (2). In two cases, islets were isolated at our center (Baylor Institute for Immunology Research). In all cases, pancreases were preserved oxygen charged static two-layer method (9) and islets were isolated according to the Edmonton protocol (8,15). Islet yield was determined with dithizone staining ((2 mg/ml; Sigma Chemical Co., St. Louis, MO, USA) under optical graticule and converted into a standard number of islet equivalents (IE, diameter standardizing to 150 μm) (8,11). At least 4,000 IE/kg body weight islets were transplanted into type 1 diabetic patients. Patients were sedated and a percutaneous transhepatic approach was used to gain access to the portal vein for all patients. Once access was confirmed, the Seldinger technique was used to place the Kumpe catheter within the main portal vein. Islets were infused by gravity using the bag technique.
Immunosuppression consisted of maintenance with tacrolimus (Prograf®, Fujisawa, Japan), at a target trough level of 4–6 ng/ml and sirolimus (Rapamune®, Wyeth Pharmaceuticals, Inc., Madison, NJ, USA), at a target trough level of 12–15 ng/ml (15).
Assessment of Islet Transplantation Efficacy
In this study, we assessed islet transplantation efficacy using the SUITO index or islet yields per body weight after a single infusion of islets from brain-dead donors into six type 1 diabetic patients. Transplantation efficacy was evaluated by HbA1C, relative insulin dose, and M-values. We avoided using the SUITO index from postoperative days (POD) 0 to 2, because broken islets release high levels of C-peptide during the first 24 h after transplantation (4,10).
The values of HbA1C pretransplantation and 3 months after islet transplantation were compared.
Relative insulin dose was calculated as follows: daily insulin dose/insulin dose immediately prior to islet transplantation. When insulin independence is achieved, the relative insulin dose is 0% and when the insulin dose is the same as just before transplantation, the relative insulin dose is 100%.
M-values were calculated using blood glucose levels from six time points (before and after breakfast, before and after lunch, before and after dinner). M-values were calculated as follows: M-value = average of six measurements of absolute value of log10[blood glucose (mg/dl)/100]3 (13).
We analyzed the relationships of HbA1C with the average SUITO index (from POD 3 to 30) and the islet equivalent per body weight. We also analyzed the relationships of the relative insulin dose with the average SUITO index (from POD 3 to 30) and islet equivalent per body weight. The relationships of the average (from POD 3 to 30) M-value with the average SUITO index (from POD 3 to 30) and islet equivalent per body weight were also analyzed.
Then we analyzed the daily SUITO index, the daily relative insulin dose, and daily M value to examine whether the daily SUITO index is useful to predict clinical outcome. For this purpose, we plotted all daily SUITO index measurements against relative insulin dose and M-values of the six recipients.
Statistical Analysis
Values were expressed as mean ± SE. Correlations between two factors were analyzed by simple regression tests. Statistical analyses were performed with Stat View 4.0. A value of p < 0.05 was considered significant.
Results
Recipient and Clinical Characteristics
Recipient characteristics are shown in Table 1. Islets were isolated at a remote center for the initial four cases and switched to a local center for the last two cases. Islets from case #5 were transplanted without culture and for the other cases islets were transplanted after culture. All isolated islets were qualified for transplantation based on the Edmonton protocol (15).
Recipient Characteristics
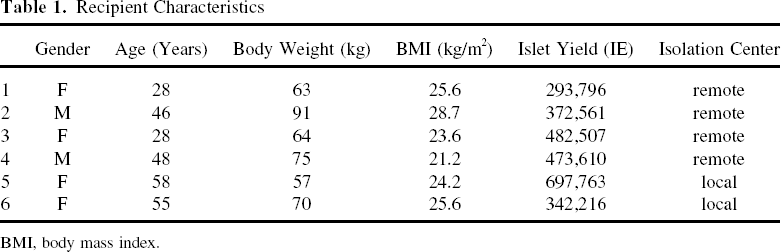
BMI, body mass index.
Islet yield per body weight, average SUITO index, and clinical characteristics are shown in Table 2. Ranges of islet yield per body weight were from 4,063 to 12,241 IE/kg. The averages (POD 3 to 30) of the SUITO index were from 6.1 to 24.6. The ranges of relative insulin dose were from 22.2% to 92.2%; therefore, even the most effective case still required 22.2% of pretransplant amount of insulin.
Characteristics of Transplant
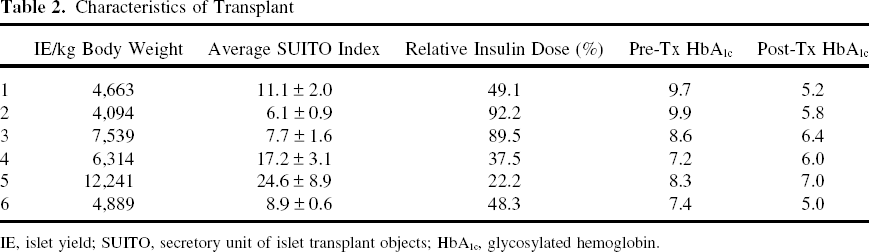
IE, islet yield; SUITO, secretory unit of islet transplant objects; HbA1c, glycosylated hemoglobin.
HbA1C data showed that all cases improved glycemic control irrespective of SUITO index or islet yield/body weight (Table 2).
Comparison of Islet Yield/Body Weight and Average SUITO Index for Prediction of Clinical Outcome
The relationship between islet yield/body weight and relative insulin dose is shown in Fig. 1, left panel. There was no significant correlation between islet yield per body weight and relative insulin dose. The relationship between the average (POD 3 to 30) SUITO index and relative insulin dose is shown in Figure 1, right panel. There was significant correlation (p = 0.031) between average SUITO index and relative insulin dose.

Relationships between relative insulin dose versus islet yield/body weight (left) and average SUITO index (right). The average SUITO index correlated with relative insulin dose.
The relationship between islet yield/body weight and the average M-values is shown in Figure 2, left panel. There was no significant correlation between islet yield per body weight and the average M-values. The relationship between the average (POD 3 to 30) SUITO index and the M-values is shown in Figure 2, right panel. There was no significant correlation between the average SUITO index and the average M-values.

Relationships between M-values versus islet yield/body weight (left) and average SUITO index (right). Neither islet yield/body weight nor the average SUITO index correlated with the M-values.
Daily SUITO Index Correlated with Daily Insulin Dose and M-Value
Then we examined the relationship between the individual SUITO index versus daily relative insulin dose and daily M-values. The daily SUITO index strongly correlated with the daily relative insulin doses (Fig. 3, left) and weakly but significantly correlated with daily M-values.
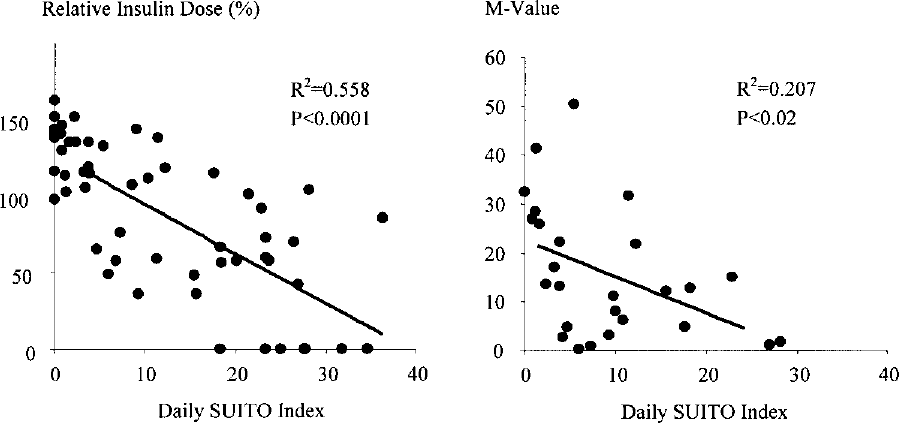
Relationships between the daily SUITO index versus the relative insulin dose (left) and M-values (right). The daily SUITO index strongly correlated with the relative insulin dose and weakly correlated with M-values.
When the SUITO index was less than 10, the average relative insulin dose was 117.1 ± 5.9% and when the SUITO index was equal or more than 10 the average relative insulin dose was 55.4 ± 8.4% (Table 3). The relative insulin dose was substantially lower when the SUITO index was equal to or more than 10 (p < 0.0000001).
SUITO Index Correlates With Insulin Dose and M-Value
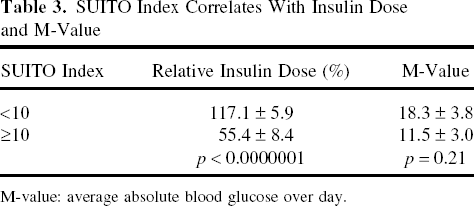
M-value: average absolute blood glucose over day.
When the SUITO index was less than 10, the average M-value was 18.3 ± 3.8 and when the SUITO index was equal to or more than 10 the average relative insulin dose was 11.5 ± 3.0 (Table 3). There was no significant difference in the average M-values between the group with a SUITO index less than 10 and the group whose index was equal to or more than 10 (p = 0.21).
Discussion
Monitoring of transplanted islet mass and function is important to evaluate clinical outcome. Previously, we have shown that single donor islet transplantation from non-heart-beating donors could improve glycemic control without hypoglycemic unawareness (12). The concept of single donor islet transplantation is important for a country that has a limited number of donor pancreata, like Japan (6,7). We evaluated islet transplantation with non-heart-beating donors and living donors using the SUITO index (4,10). In that study, an average SUITO index (from POD 3 to 30) of more than 26 was associated with insulin independence (10).
In this study, the average SUITO index but not islet yield/body weight correlated with relative insulin dose. An islet yield/body weight ratio of more than 10,000 IE/kg is associated with insulin independence according to the Edmonton protocol (15). In this study, we found that the average SUITO index was a better indicator of clinical outcome than islet yield/body weight. This is reasonable because islet yield did not reflect viability or engraftment of transplanted islets. On the contrary, the SUITO index was calculated based on secreted C-peptide stimulated by glucose, which should reflect islet mass and function. The average SUITO index of approximately 30 was associated with insulin independence after islet transplantation from brain-dead donors when we extrapolated the data. This result is similar to the results of islet transplantation from non-heart-beating and living donors.
HbA1C were all improved, irrespective of islet mass or SUITO index. This is most likely because islets can meticulously regulate blood glucose, irrespective of the amount of external insulin injected. Even small amounts of engrafted islets were helpful for improving glycemic control and this fact is important to support the concept of single donor islet transplantation for brittle type 1 diabetes. The average M-value did not correlate with either the SUITO index or islet yield/body weight. This also indicated that even a small amount of engrafted islets could maintain excellent glycemic control, irrespective of the amount of external insulin injected.
Next, we compared the daily SUITO index with the daily relative insulin dose and daily M-values. We selected M-values instead of MAGE. MAGE requires 2-day blood glucose measurements (15) and therefore cannot be used as a daily indicator. The daily SUITO index strongly correlated with the daily relative insulin dose and weakly correlated with M-values. Because the SUITO index reflected engrafted islet mass, it seems reasonable that it correlates with the daily relative insulin dose.
Interestingly, the average relative insulin dose was more than 100% when the SUITO index was less than 10. This means the patients needed more insulin compared to the dose of insulin before transplantation. In such cases, patients still improved glycemic control after islet transplantation even though more insulin was required, evaluated by improved HbA1C and fewer events of hypoglycemic unawareness. A possible explanation is that after islet transplantation, alpha cells in the transplanted islets may secrete glucagon to counteract the overdose of the insulin injection that can stabilize glucose levels. In addition, use of tacrolimus might increase glucose levels, which might result in high insulin dosage.
The daily SUITO index weakly correlated with M-values. This suggested that even small amounts of engrafted islets help to maintain excellent glycemic control. Consequently, larger amounts of engrafted islets might maintain glycemic control more efficiently. However, there was no significant difference in the M-values between the group with a SUITO index of less than 10 and the group with a SUITO index equal to or more than 10. This also indicated that a relatively small number of islets can work to stabilize glycemic control.
In conclusion, the SUITO index was an excellent predictor of clinical outcomes, especially to predict the necessary insulin dose. We recommend using this simple index for assessing engrafted islet mass and function.
Footnotes
Acknowledgments
We thank Dr. Carson Harrod and Yoshiko Tamura for their careful review of this manuscript. This research is partly supported by All Saints Health Foundation and Otsuka Pharmaceutical Factory Inc. This research was partially presented at the 34th annual meeting of The Japan Society for Organ Preservation and Medical Biology.