
Abstract
Many epidemiological questions concern potential interventions to alter the pathways presumed to mediate an association. For example, we consider a study that investigates the benefit of interventions in young adulthood for ameliorating the poorer mid-life psychosocial outcomes of adolescent self-harmers relative to their healthy peers. Two methodological challenges arise. First, mediation methods have hitherto mostly focused on the elusive task of discovering pathways, rather than on the evaluation of mediator interventions. Second, the complexity of such questions is invariably such that there are no well-defined mediator interventions (i.e. actual treatments, programs, etc.) for which data exist on the relevant populations, outcomes and time-spans of interest. Instead, researchers must rely on exposure (non-intervention) data, that is, on mediator measures such as depression symptoms for which the actual interventions that one might implement to alter them are not well defined. We propose a novel framework that addresses these challenges by defining mediation effects that map to a target trial of hypothetical interventions targeting multiple mediators for which we simulate the effects. Specifically, we specify a target trial addressing three policy-relevant questions, regarding the impacts of hypothetical interventions that would shift the mediators’ distributions (separately under various interdependence assumptions, jointly or sequentially) to user-specified distributions that can be emulated with the observed data. We then define novel interventional effects that map to this trial, simulating shifts by setting mediators to random draws from those distributions. We show that estimation using a g-computation method is possible under an expanded set of causal assumptions relative to inference with well-defined interventions, which reflects the lower level of evidence that is expected with ill-defined interventions. Application to the self-harm example in the Victorian Adolescent Health Cohort Study illustrates the value of our proposal for informing the design and evaluation of actual interventions in the future.
Keywords
1 Introduction
In areas such as life course and social epidemiology, questions arise around potential interventions to alter pathways presumed to mediate an association, such as between an early-life marker of vulnerability and later outcomes. Our motivating example investigated potential interventions to counter the poorer psychosocial outcomes in adulthood of adolescents who self-harm relative to their healthy peers, such as targeting substance use and mental health problems in young adulthood. Addressing such questions raises two key methodological challenges, which this paper aims to tackle.
The first challenge relates to the focus of the mediation literature on the discovery of mechanistic pathways. 1 The prevailing logic is to assume a pre-existing (axiomatic) notion of mediation and then to define “indirect” effects so as to detect and quantify this, with the modern definitions in the potential outcomes framework referred to as “natural” effects.2–5 These effects are not defined in a way that makes them empirically measurable, even hypothetically, in a randomised experiment, 1 , 6 and alternative methods that would explicitly address the issue of mediator intervention evaluation have been lacking. This is striking given that the implied appeal of discovering pathways is often to reveal potential intervention points. It also contrasts with current thinking in the broader epidemiological literature, where the elusive nature of the notion of “causation” 7 , 8 (of which “mediation” is an extension), tied to aspirations for an epidemiology of consequence, 9 has brought a move away from the quest for the discovery of causes. Instead, emphasis is given to the more tangible goal of assessing effects of causes conceptualised as interventions, 7 ,10–12 with analyses designed to emulate a “target trial”, 13 , 14 defined as the ideal randomised trial that one would hypothetically perform to evaluate the intervention in question.
The second challenge is that the endeavour of intervention evaluation presupposes the existence of well-defined interventions. However, the complexity of the questions being asked in many areas, such as the self-harm example, is often such that there are no well-defined interventions for which data have been or could be collected to directly assess impact for the populations, outcomes and time-spans of interest. Instead, to address their questions, researchers have to rely on observational exposure (non-intervention) data, for example from long-term longitudinal cohort studies, and use mediator measures such as depression symptoms for which the actual interventions that one might implement to alter them are not well defined. There has been much criticism of such “exposure epidemiology” for causal inference, yet producing some evidence, even if imperfect, is arguably a key first step to future intervention development and evaluation. 15 This explains a recent push 10 ,15–17 for addressing, rather than shunning, the methodological challenge of ill-defined interventions, and it has been suggested that simulation-based evaluation of hypothetical interventions might be needed. 10
In this work, we reverse the logic that has driven the mediation literature: rather than assuming a pre-existing notion of mediation, we propose to start with specific policy-relevant questions relating to mediator interventions and then define effects to address these in explicit correspondence to a target trial. We show that, within this logic, mediation effects are not required if the question and available data pertain to well-defined mediator interventions, but mediation regains its relevance in the context of ill-defined interventions, in the form of so-called “interventional effects” (a.k.a. “interventional randomised analogues”).18–21
Specifically, recent work shows that interventional mediation effects implicitly emulate effects in target trials that evaluate the impacts of distributional shifts in the mediators. 22 We propose that conceptualising such distributional shifts as arising from hypothetical interventions provides a useful framework for simulating potential effects and thus tackle the issue of ill-defined mediator interventions, in particular as this acknowledges the composite nature of the exposures under consideration. 16 However, given their unintentional (implicit) nature, the target trials emulated by previously proposed interventional effects for the setting with multiple mediators and a time-fixed–exposure 19 , 23 are not necessarily relevant for informing policy (see section “Summary and comparison with previous effects”). Therefore, we define novel interventional effects explicitly in terms of a target trial that addresses three specific policy-relevant questions, regarding the impacts of intervening to shift mediators separately (under various interdependence assumptions), jointly or sequentially.
The paper is structured as follows. First, we introduce the self-harm example. Second, we introduce the issue of ill-defined mediator interventions and propose a novel conceptual framework under a set of principles for tackling it via simulation of hypothetical interventions. Third, we describe the target trial integrating these principles and derive novel definitions of interventional effects that map to that trial, with a description of how these compare with previous proposals. Fourth, we determine identification assumptions and describe a g-computation estimation method, providing example R code. Finally, we illustrate the value of the proposed approach in the self-harm example and conclude with a discussion.
2 Self-harm example
Adolescent self-harm is on the rise24–26 and is associated with substantial disease burden 27 through immediate effects on health and mortality, 28 as well as through persisting associations with poor health and social functioning in later life, including higher rates of substance use, 29 , 30 depression 29 and financial hardship. 31 A question of considerable public health interest is whether policies targeting young adulthood processes may have benefit in reducing these impacts. We focus on the financial hardship outcome, and consider four young adulthood mediators: depression or anxiety, cannabis use, lack of higher education and unemployment. 31 We draw data from the Victorian Adolescent Health Cohort Study, a 10-wave longitudinal population-based cohort study of health across adolescence to the fourth decade of life in the state of Victoria, Australia (1992–2014). Data collection protocols for this study were approved by the Ethics in Human Research Committee of the Royal Children’s Hospital, Melbourne. Informed parental consent was obtained before inclusion in the study. In the adult phase, all participants were informed of the study in writing and gave verbal consent before being interviewed. The Supplementary Materials provide more details on study design, with the key measures of relevance for our illustrative analysis summarised next.
The main exposure, denoted
Pre-exposure confounders (
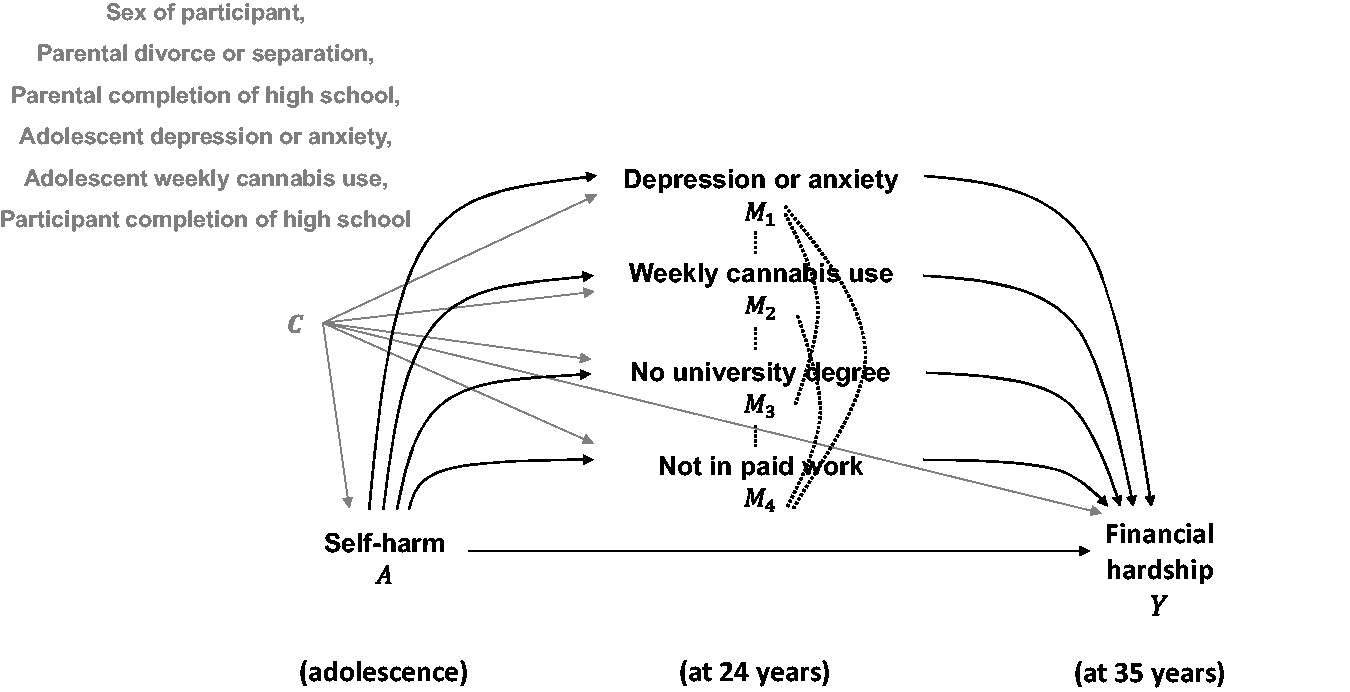
Directed acyclic graph portraying the assumed causal structure for the observed data, conceptualising the pathways from adolescent self-harm to financial hardship, via the four mediators of interest. Dotted undirected arrows indicate where we are agnostic about the directionality of causal influences. Pre-exposure confounders and arrows from these are shown in grey to improve clarity.
3 Proposed framework for tackling ill-defined interventions
We consider the general case of
However, with no well-defined interventions for which data are available, the most common approach is to simply estimate the contrasts
We propose the following principles to tackle these issues:
Explicitly acknowledge that evidence for actual interventions in this context is not possible. Instead, one can address a more modest goal: that of informing “intervention targets”, that is, the constructs that future hypothetical interventions might target, which are what is captured in available data. Although such evidence should be regarded as of lower level than causal inference about well-defined interventions, it might be the only available in the field. Define effects that map to a target trial assessing the impact of the distributional mediator shifts that those hypothetical interventions might achieve; these shifts can be individualised, i.e. conditional on covariates. Similar to effects studied by VanderWeele and Hernan,
33
this amounts to setting mediators to random draws from distributions specified to reflect realistic, user-specified benchmarks, to simulate the potential impacts of hypothetical interventions. The unexposed population (and thus the concept of mediation) regain relevance in specifying these “estimand assumptions”. In addition to these, “identification assumptions” are required to ensure that the estimand can be estimated from available data. An expanded set of assumptions is required for causal inference with ill-defined vs. well-defined interventions, as should be expected.
10
In specifying relevant distributional shifts, consider the joint distribution of the mediators. This enables the mediator interrelatedness to be accounted for even without making causal ordering assumptions. The price to pay for this is a need to make unverifiable assumptions regarding the correlations amongst the mediators (at a population, distributional level) under the hypothetical interventions, as these correlations cannot be expected to remain as in the observed data, i.e. without intervention. For example, mental health in a subpopulation offered widespread provision of psychotherapy might be more or less correlated (on average) with substance use than in one offered widespread provision of antidepressants.
Figure 2 provides a conceptual overview of the proposed framework for evaluating hypothetical interventions. The approach can be seen as an intermediate step between traditional causal inference, which relies predominantly on data, and simulation-based approaches like agent-based modelling, which depend less on data and more on theory and modelling, i.e. assumptions. As Hernán has noted, 34 such approaches to causal inference are needed in disciplines that ask more complex questions, like in our example.
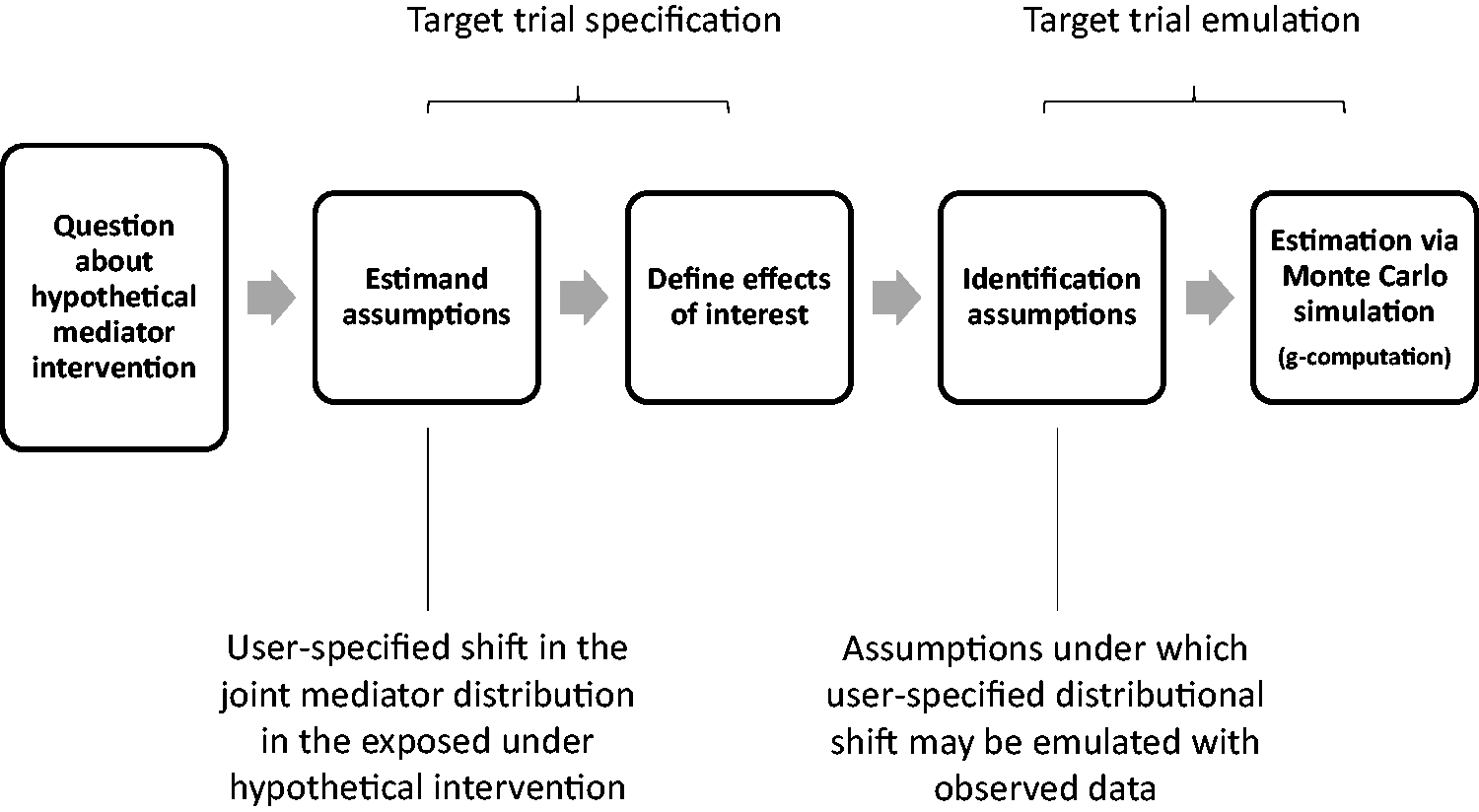
Conceptual overview of the proposed approach for tackling the issue of ill-defined interventions via simulation of hypothetical interventions
4 Target trial
We now describe the target trial that integrates these principles, with focus on three specific policy-relevant questions.
Question 1: If targeting only one mediator (“one-policy premise”), which of these separate interventions would provide the “biggest bang for the buck”, in terms of reducing disparities between exposure groups?
This question is of relevance under resource (e.g. financial) constraints implying that the policy maker would implement only one of the
(a) Approach under minimal estimand assumptions
We first consider the following reduced set of estimand assumptions (E1–E3), which allows for less assumption-laden and thus clearer comparisons and is likely to be widely applicable as a starting point:
E1. Intervention
E2. Intervention
E3. Intervention
Formally, we represent E1–E3 as the assumption that the hypothetical intervention

Assumption E1 could be modified if the policy maker intended to personalise treatments conditional on other mediators. However, this would require an expanded set of estimand assumptions, e.g. delineating which mediators, etc. Assumption E2 is justified on the basis that realistically we cannot expect effects beyond bringing levels to those in the unexposed, which can be estimated from the data. Furthermore, this benchmark is meaningful in that it addresses the question of how disparities in the outcome between exposure groups reduce when disparities in the mediator are eliminated. Other benchmarks could be specified by the user if they make sense in the specific context, but again this may require additional unverifiable assumptions. Assumption E3 can be considered a worst case scenario in the sense that it precludes any effects of the hypothetical intervention flowing onto other mediators that may be causal descendants. This seems appropriate for the purpose of comparing potential intervention targets, but it can be relaxed to allow for correlations between
A target trial for the self-harm example under assumptions E1–E3 is depicted in Figure 3. Arms 1 and 2, referred to as the unexposed and exposed groups, correspond to those in a classic two-arm parallel trial design: the intervention is only to set the exposure to
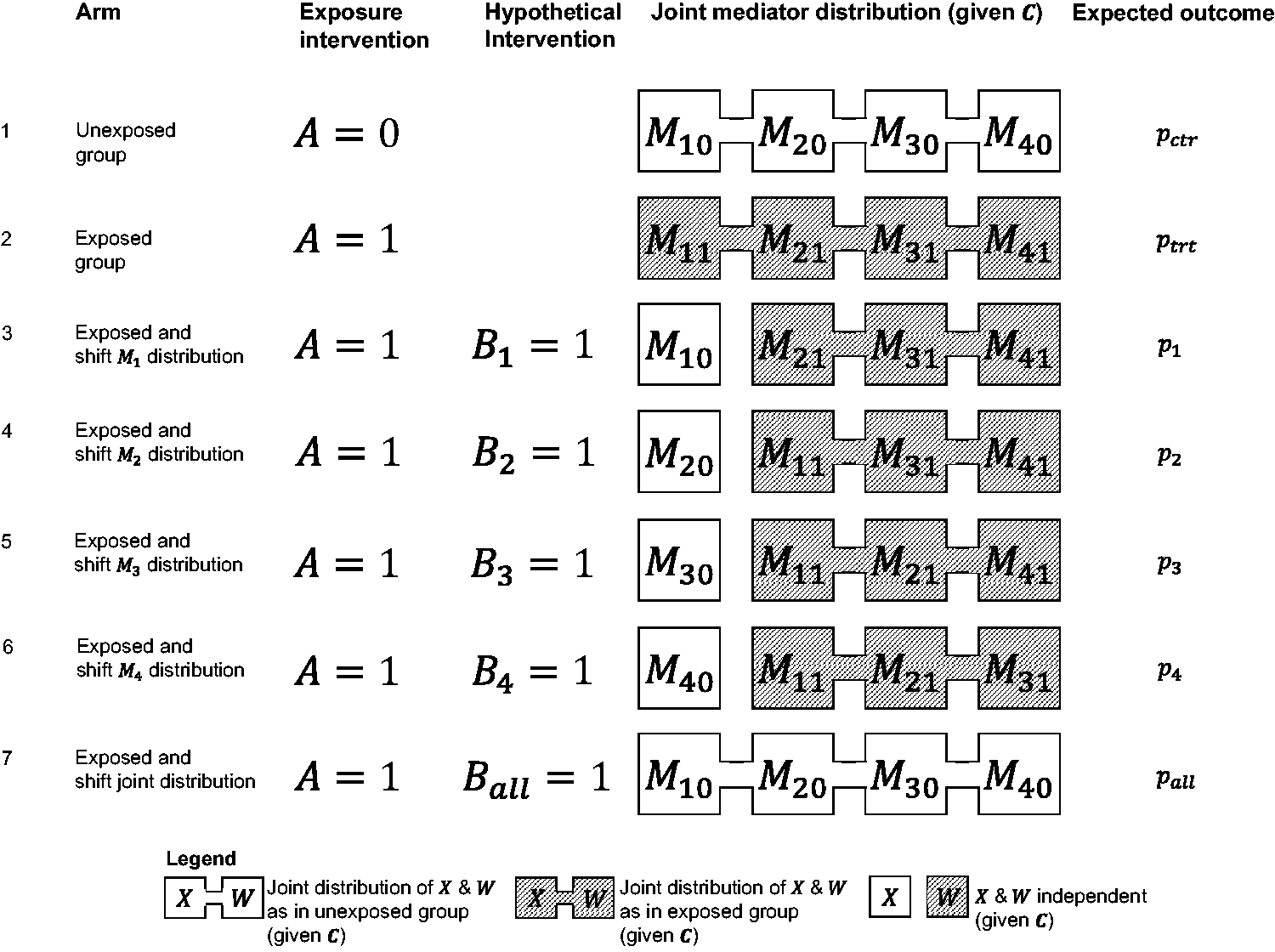
Graphical depiction of arms in the “target trial” designed to examine the effects of hypothetical interventions resulting in individualised shifts in the distributions of four interdependent mediators. This figure shows the arms required to evaluate effects addressing Question 1 (one-policy premise) under approach (a), and Question 2 (remaining disparities).
(b) Approach under causal ordering and mediator interdependence estimand assumptions
To relax E3, we need to make additional assumptions about the order of the mediators as well as the correlations between the mediators after the hypothetical intervention. For instance, we can consider alternative interventions
E3′. Assume that:
The order of the mediators is Under intervention Under intervention
Formally, E1, E2 and E3′ can be expressed as the assumption that the hypothetical intervention

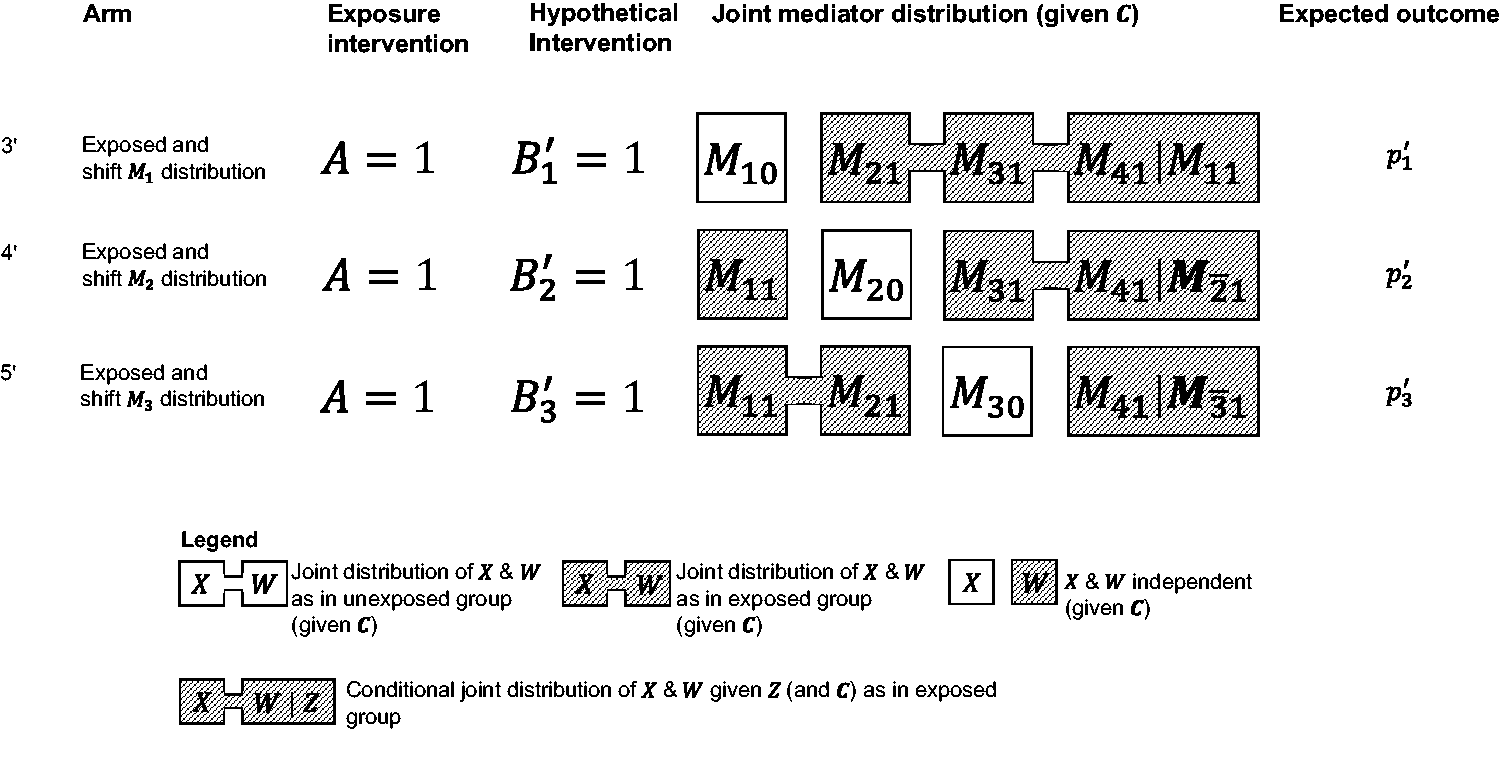
Extension of target trial of Figure 3, including arms required to evaluate effects addressing Question 1 (one-policy premise) under approach (b).
Question 2: What would be the remaining disparities between exposure groups if it were possible to jointly target all the mediators?
We can address this question by considering a hypothetical intervention
E4. The hypothetical intervention
Formally, assumption E4 states that the hypothetical intervention
Arm 7 in Figure 3 shows what this translates to in the target trial: in this arm,
Question 3: What would be the benefit of sequential policies, applying the separate mediator interventions under Question 1 approach (a) sequentially?
Let
Formally, E1–E3 in this setting can be expressed as the assumption that

To evaluate the impact of the sequential interventions, we can add more arms to the trial, as depicted in Figure 5 for the case of four mediators. Only three arms are added as
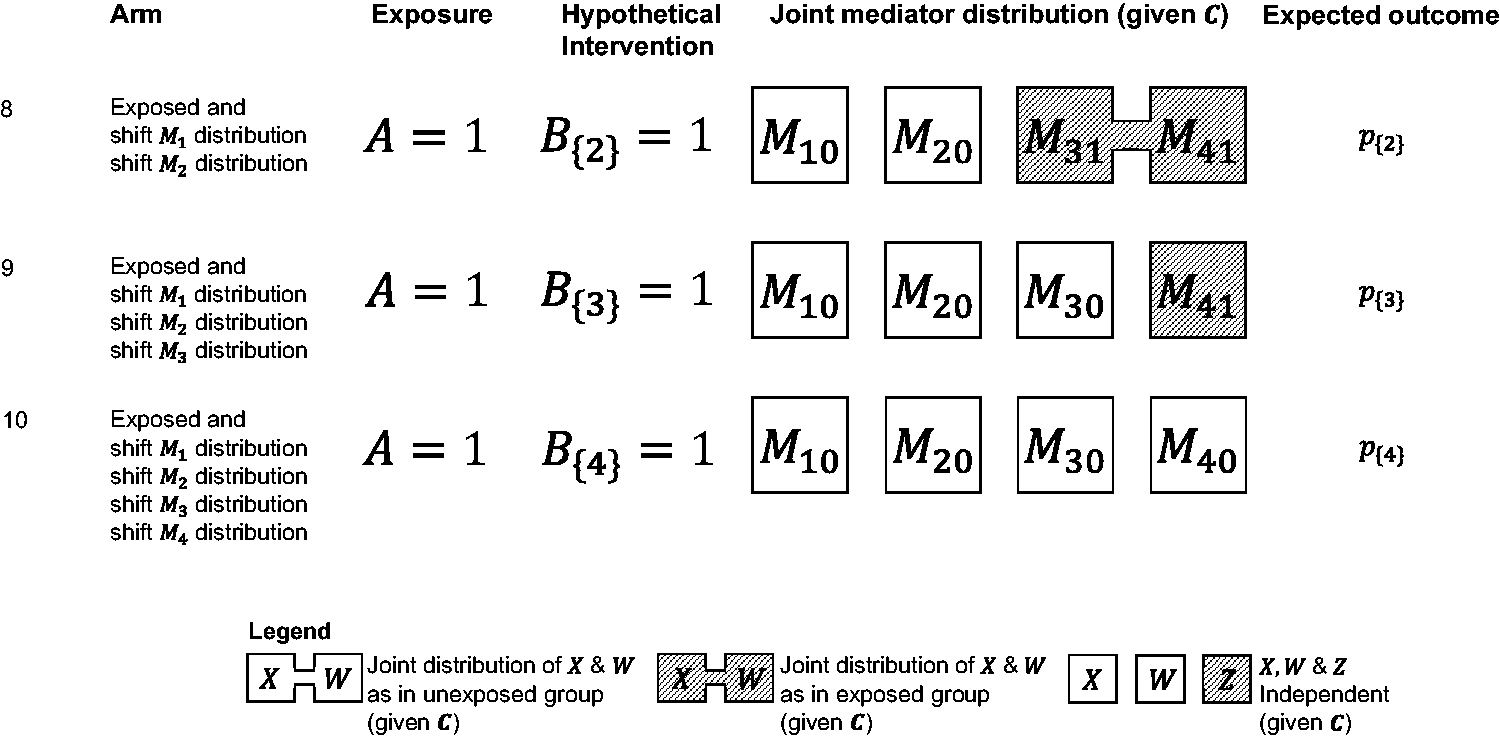
The target trial in Figures 3 to 5 extends in the natural way to the case of
5 Mediation effect definitions
We define interventional effects addressing each question by contrasting the outcome expectation between relevant trial arms. Following the notation in the last column of Figures 3 to 5, but considering the general case of
The total causal effect (
5.1 Effects for Question 1: one-policy premise
(a) Effects under minimal estimand assumptions
We define a type of interventional indirect effect via the

This quantifies the impact of an intervention targeting
In a previous section, we mentioned that in the context of well-defined interventions, i.e. if we had data on an intervention
(b) Effects under causal ordering and mediator interdependence estimand assumptions
Similarly, we define an alternative type of interventional indirect effect via the

This quantifies the impact of an intervention targeting
Effects under both (a) and (b) differ from those proposed by Vansteelandt and Daniel, 19 which implicitly emulate other distributional shifts (see section “Summary and comparison with previous effects” below). 22
5.2 Effects for Question 2: Remaining disparities
We consider the following interventional direct effect not via any mediator (

The

5.3 Effects for Question 3: Sequential policies
We define the interventional indirect effect of the

The sum of these effects provides an interventional indirect effect quantifying the overall impact of the sequential intervention (

5.4 Decompositions of the TCE and other interesting effects
There are many possible decompositions of the
The decomposition that focusses on sequential policies is:
Other contrasts that could be of interest are
5.5 Summary and comparison with previous effects
Table 1 summarises the proposed effects in terms of the assumed mediator distribution shifts under hypothetical interventions and the contrasting (pre-intervention) state. Next to each intervention effect, defined as the contrast between pre- and post-intervention states, we show in brackets the estimand expressing the remaining between-exposure-group differences after the intervention, i.e. the difference remaining between unexposed and exposed after the intervention. Whether it is the intervention effect or the remaining difference that is of most interest depends on the question, e.g. Question 1 is focused on intervention effects while Question 2 is framed around remaining differences. The table also shows the estimand assumptions underlying other effects that have been proposed in the literature for the setting with multiple mediators and a time-fixed–exposure, 19 , 23 viewing them through the lens of our proposed framework for evaluating the effects of hypothetical interventions on mediator distributions (Figure 2).
Comparison of proposed and previously published interventional effects for multiple mediators with a point exposure, in terms of their interpretation as effects of hypothetical interventions shifting mediator distributions.
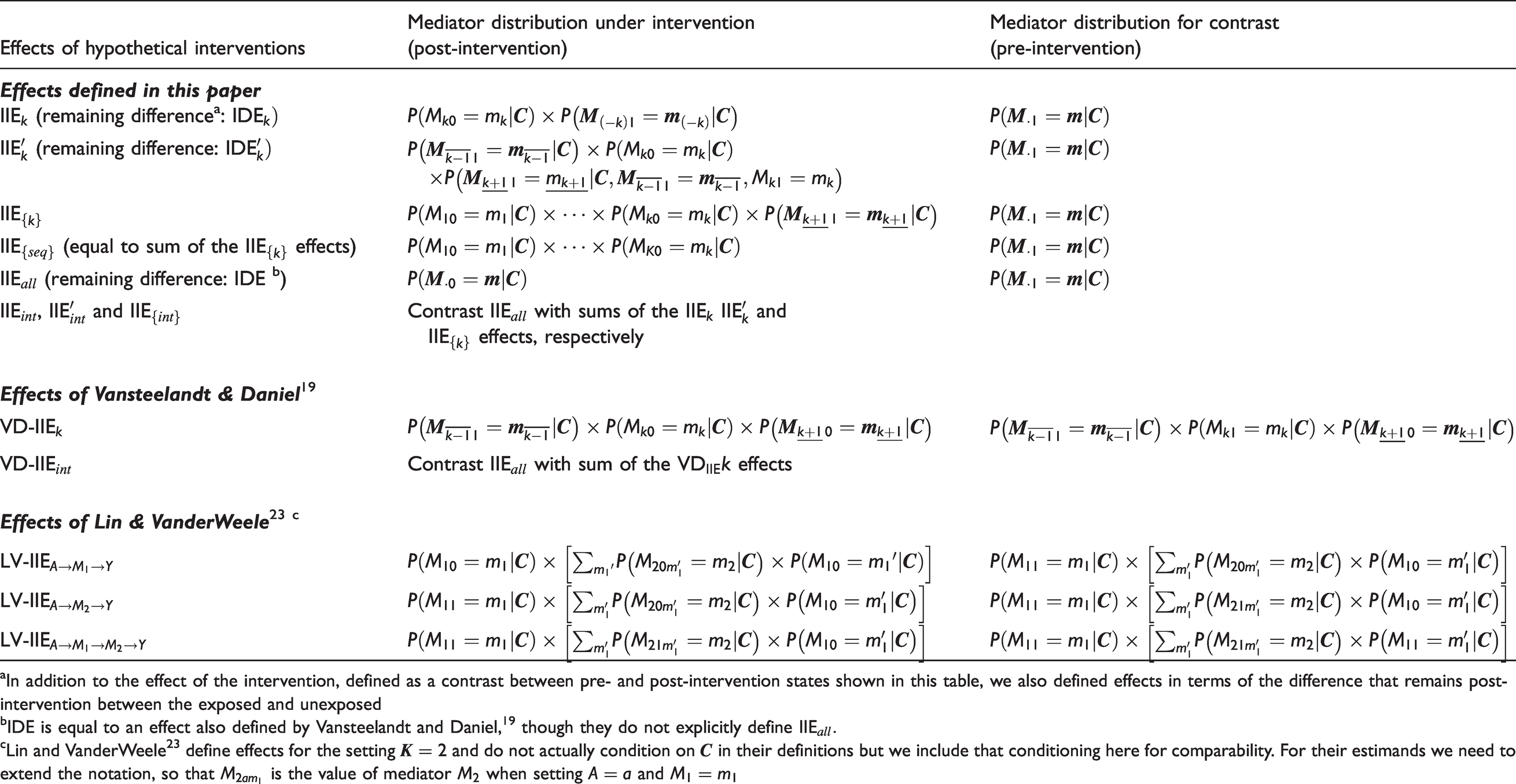
aIn addition to the effect of the intervention, defined as a contrast between pre- and post-intervention states shown in this table, we also defined effects in terms of the difference that remains post-intervention between the exposed and unexposed
bIDE is equal to an effect also defined by Vansteelandt and Daniel,
19
though they do not explicitly define
cLin and VanderWeele23 define effects for the setting
It is seen that previous effects are different from the proposed effects and their interpretability in answering policy-relevant questions about hypothetical interventions requires consideration. For example, the mediator-specific effects of Vansteelandt and Daniel,
19
denoted in Table 1 by VD-
Of note, other previously proposed estimands that can be considered to fall under the “interventional effects” umbrella either focus on the setting where only a single mediator is of substantive interest 18 , 20 , 21 ,35–37 or when the exposure is time-varying 38 , 39 so are not directly comparable with our proposal. Other related effects are those that correspond to shifting confounder40–42 or exposure 43 , 44 distributions (see section 8).
6 Identification and estimation
To identify and emulate these effects, it suffices to consider the identifiability and estimation of the outcome expectation in a given target trial arm subject to a mediator distribution shift (arms 3–10 and 3′–5′). Let
In addition to standard positivity assumptions, 45 we make the following identification assumptions:
A1. There is no causal effect of
A2. The following conditional independence assumptions hold


A3.
A1–A3 are similar to those considered by VanderWeele and Hernán.
33
With the intervention
Under A1–A3, the outcome expectation in the given arm can be emulated using observational data. Complete identification formulae and proofs are given in the Supplementary Materials. For illustration, consider the arm where intervention 
Estimation can be performed using the Monte Carlo simulation-based g-computation approach described by Vansteelandt and Daniel 19 (see Supplementary Materials). To reduce the risk of misspecification bias, it is recommended to use rich parametric models, including various interaction terms and higher-order terms (for continuous variables). 46 Example code in R47 for implementing the method, including a function and a worked example on simulated data, can be accessed at the first author’s GitHub repository (https://github.com/moreno-betancur/medRCT).
7 Results for self-harm example
Table 2 shows descriptive statistics based on the 1786 participants (out of 1943 in the cohort study) with the adolescent self-harm exposure available. As all other analysis variables had missing data, subsequent analyses were based on multiple imputation using 40 imputations (details in Supplementary Materials). Table 3 shows preliminary estimates of unadjusted and regression-adjusted exposure-outcome, exposure-mediator and mediator-outcome associations, which were obtained using main-effects multivariable logistic regression models. These provide an idea of the strength of some of the hypothesised pathways in Figure 1.
Descriptive statistics by exposure group in the self-harm example.
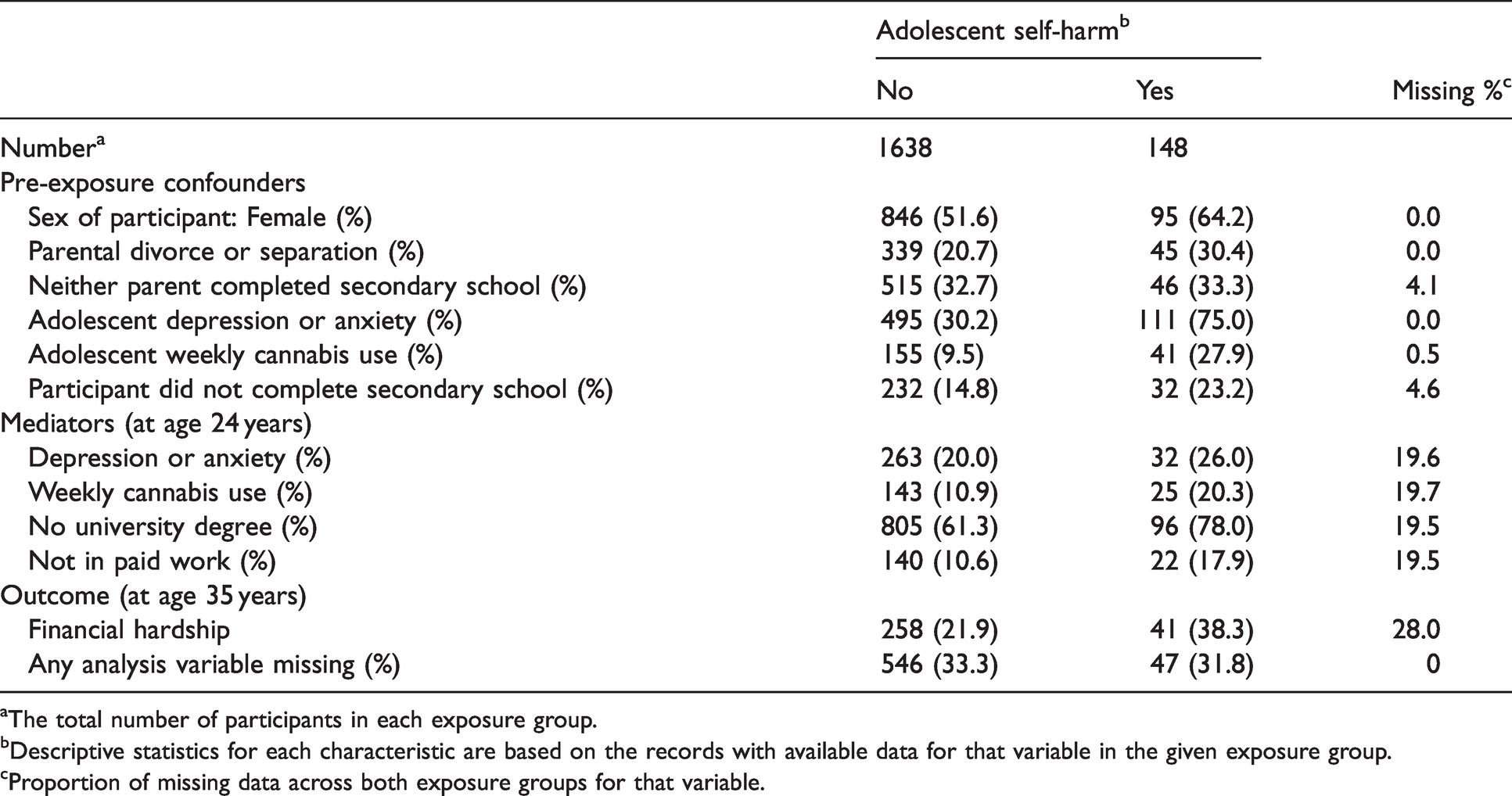
aThe total number of participants in each exposure group.
bDescriptive statistics for each characteristic are based on the records with available data for that variable in the given exposure group.
cProportion of missing data across both exposure groups for that variable.
Associations amongst exposure, outcome and mediators estimated using multivariable logistic regression models and multiple imputation (40 imputations).
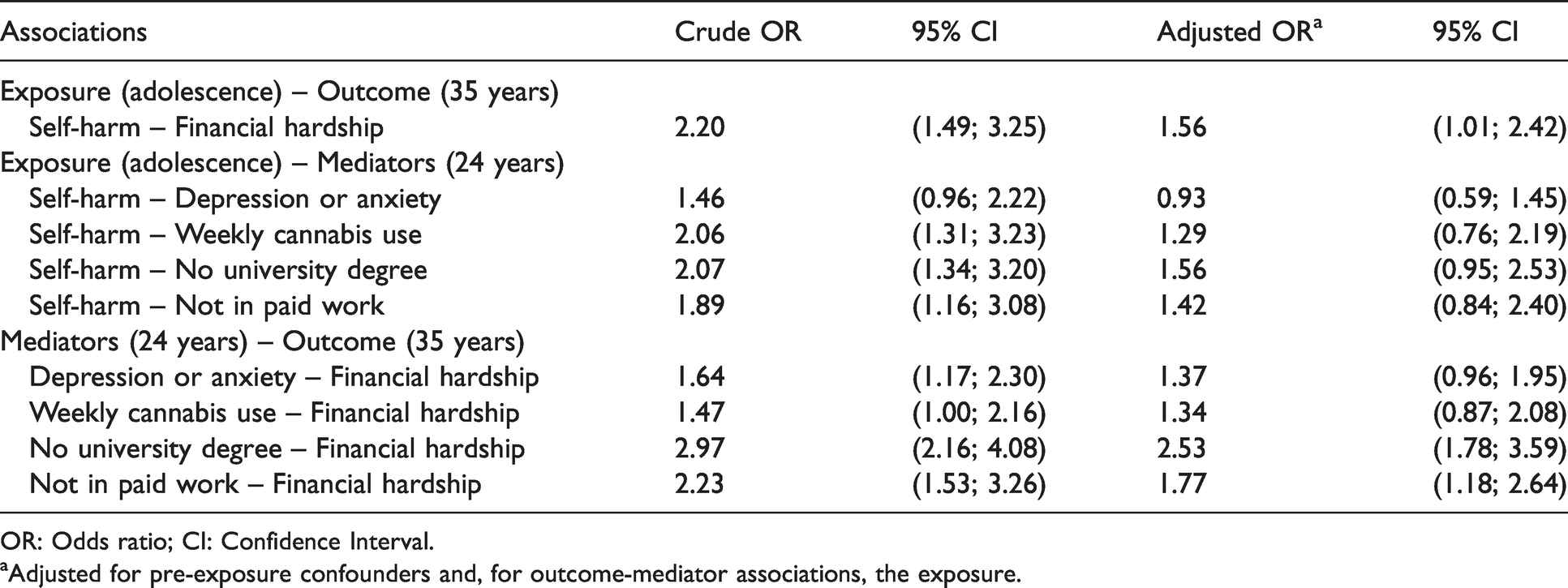
OR: Odds ratio; CI: Confidence Interval.
aAdjusted for pre-exposure confounders and, for outcome-mediator associations, the exposure.
We estimated the proposed effects using the g-computation method with multivariable logistic regressions including all two-way interactions (see Supplementary Materials); see Table 4 for results. Adolescent self-harmers had an increased risk of financial hardship in adulthood compared to non-self-harmers in our study:
Estimates of proposed interventional mediation effects to address each policy-relevant question, obtained using the Monte Carlo simulation-based g-computation approach (200 replications), along with the bootstrap (1000 runs) and multiple imputation (40 imputations).
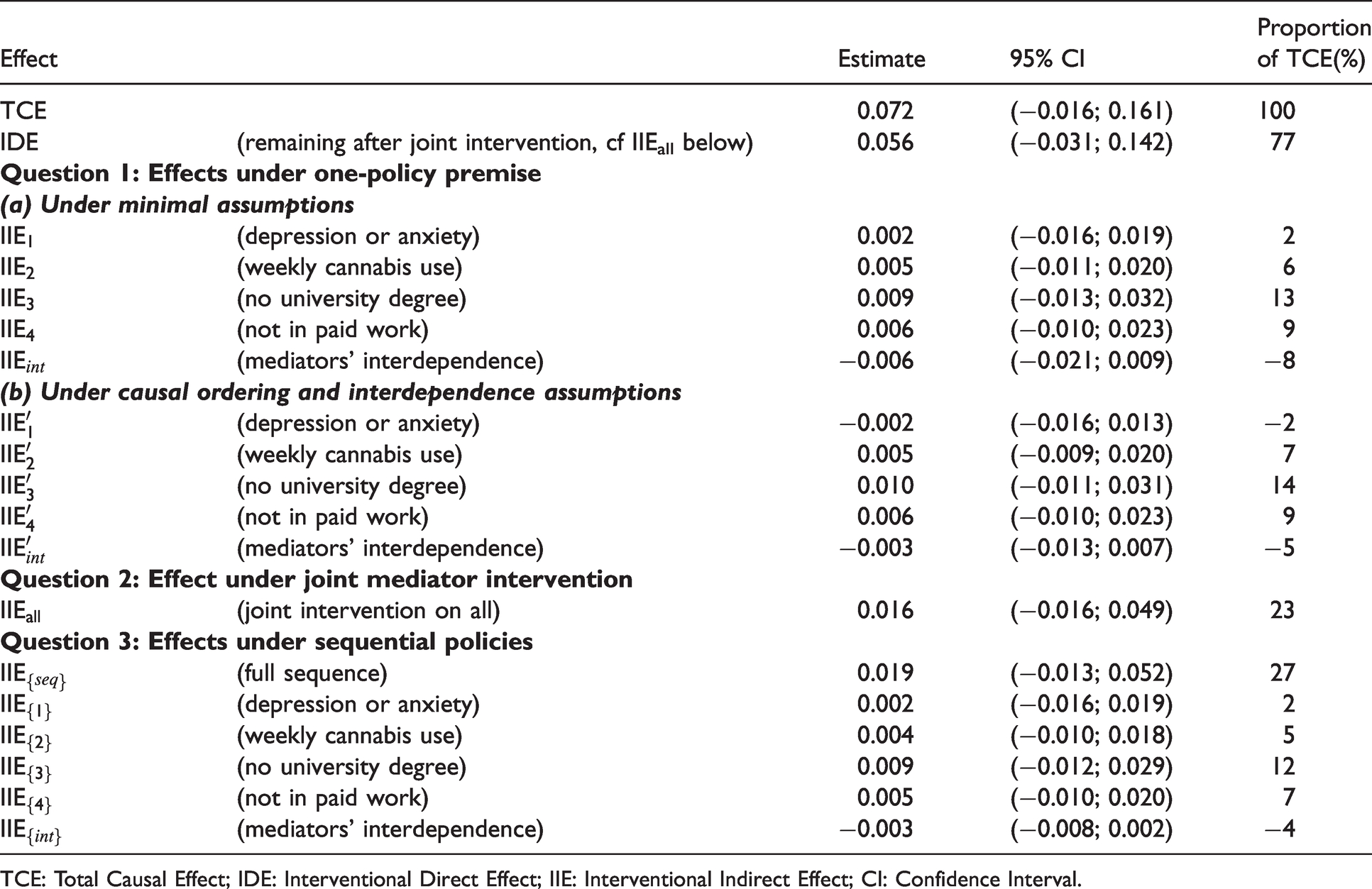
The overall sequential policy could, in principle, achieve a reduction of 27% of the total effect (
8 Discussion
While avoiding previous “axiomatic” definitions of mediation, this paper proposed a novel framework that uses interventional mediation effects for tackling the issue of ill-defined interventions that abounds in various areas of epidemiology. 10 ,15–17 Building on previous work, 22 novel interventional effects are defined that explicitly emulate target trials of hypothetical interventions that result in individualised (covariate-specific) mediator distributional shifts. Simulating the effects of hypothetical interventions in this way addresses the realistic if relatively modest goal of informing intervention targets and requires an expanded set of assumptions both to define the estimand and to identify it with observational data. This is commensurate with the lower-level evidence and increased subtlety in interpretation that is to be expected with ill-defined interventions, towards the left-hand end of the Galea-Hernán causal spectrum, for which one must simulate “in silico hypothetical experiments”. 10 , 34 Although uncertainty of estimation precludes any strong conclusions being drawn, the self-harm example illustrated the value of our proposal for addressing policy-relevant questions.
We retained mediation terminology (“direct”, “indirect”, etc.) for the proposed effects, consistent with the view that there is no clear definition of these notions beyond these and so-called “separable” effects (see below). Although we suggest that it is more realistic to focus on the benchmark of our proposed direct effects, which is the distribution in the unexposed given covariates, it is straightforward to apply the same methodology to evaluate hypothetical interventions that set the mediators to another user-specified distribution, even a degenerate (constant-valued) distribution; for example, one could even assess the extreme case where mediators are eliminated. In this sense, interventional direct effects generalise “controlled direct effects”, which can be seen as setting the mediator to a draw from a degenerate distribution. Others have also considered more realistic benchmarks in the definition of direct effects.
37
,
48
More broadly, although the estimand assumptions outlined here are likely to be of relevance in a range of settings, alternative assumptions might well be warranted in other contexts. In particular, further work could consider estimand assumptions that individualise mediator shifts by conditioning on a set of baseline covariates that may overlap with but is not necessarily equal to the minimal confounding adjustment set
The identification assumptions that concern hypothetical interventions are not assessable without considering a concrete intervention. As has been noted, 10 , 32 , 33 confounder selection is complex in this context: considering common causes of the intervention and its target is difficult with no concrete intervention in mind. Nonetheless, the mapping to a target trial makes it clear that all identification assumptions underlying interventional effects would be assessable in randomised experiments of the hypothetical interventions. This contrasts with natural effects, which require “cross-world independence” assumptions that are not empirically verifiable, even in hypothetical experiments, 1 , 6 as well as further untestable assumptions in the context of multiple mediators. 18 , 22 , 49 , 50 This difference is due to interventional effects being population-level quantities, like the total causal effect, whilst natural effects are individual-level effects. 22 An exception for natural effects is when the exposure is separable into components acting through distinct pathways, 6 , 51 , 52 with the resulting separable effects emulating hypothetical trials of intervention regimes on the exposure components.
Assumptions about the causal ordering of the mediators are not needed for defining and identifying the proposed effects except those under approach (b) to Question 1. This is facilitated by the fact that estimand assumptions pertain to the joint distribution and, for sequential policies, the choice of question for the policy-maker (e.g. which sequence of policies is of interest?). As previously mentioned, the price to pay for considering the joint distribution in the estimand assumptions, even under approach (b) to Question 1, is the need for unverifiable assumptions about the dependence between the mediators under the hypothetical interventions, which, as the shifts themselves, would not be identifiable from the data. It was interesting to note, however, that results under approaches (a) and (b) to Question 1 were very similar, which is consistent with the expectation that effects via interdependence are small, following Vansteelandt and Daniel. 19 It may therefore be that assumptions about mediator interdependencies do not have much impact on estimates.
It is important to make a connection with the literature on estimation of causal effects under distributional interventions on an exposure 43 , 44 – called “population intervention effects of stochastic interventions”. In the context of one mediator, interventional mediation effects are equivalent to population intervention effects of stochastic interventions in the mediator within the exposed group. With multiple mediators, as mentioned previously, our approach focusing on stochastic interventions on the joint mediator distribution provides a way of identifying those effects in the context of unknown causal ordering of the mediators, which would otherwise be needed for appropriate confounding control. This connection will be important when extending this approach to continuous mediators because the scenario of continuous exposures has been considered in depth in the literature on population intervention effects of stochastic interventions. Indeed, careful thought would be needed regarding sensible estimand assumptions for, say, a two-parameter distribution, e.g. to specify how the hypothetical intervention affects the mean and the variance of the target mediator. As such, this would be best investigated in the context of a real example, as we did here.
A (non-causal) ordering needs to be chosen for estimating the joint mediator distribution if a sequential regression approach is used. We implemented g-computation using highly flexible regression models, but parametric misspecification bias is still a possibility. Development of doubly or multiply robust methods for estimation with machine learning, building on recent work, 53 would be desirable to counter parametric misspecification bias.
Importantly, our goal in this work was to define the contrasts of interest in the context of questions regarding ill-defined mediator interventions, acknowledging that this is only one step of a full “target trial approach,” which must also consider further protocol components of the target trial. 14 Further applications and future extensions of our proposal, e.g. to time-varying mediators and dynamic policies, should consider the broader set of target trial principles. Nonetheless, our proposal opens new avenues for causal inference about policy-relevant effects with ill-defined interventions.
Supplemental Material
sj-pdf-1-smm-10.1177_0962280221998409 - Supplemental material for Mediation effects that emulate a target randomised trial: Simulation-based evaluation of ill-defined interventions on multiple mediators
Supplemental material, sj-pdf-1-smm-10.1177_0962280221998409 for Mediation effects that emulate a target randomised trial: Simulation-based evaluation of ill-defined interventions on multiple mediators by Margarita Moreno-Betancur, Paul Moran, Denise Becker, George C Patton and John B Carlin in Statistical Methods in Medical Research
Footnotes
Acknowledgements
We thank the reviewers for invaluable feedback and Carolyn Coffey for sharing her knowledge of the Victorian Adolescent Health Cohort Study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a Discovery Early Career Researcher Award fellowship to MMB from the Australian Research Council [DE190101326]. This work was also supported by The University of Melbourne (MMB) and the NIHR Biomedical Research Centre at University Hospitals Bristol NHS Foundation Trust and the University of Bristol, England (PM). The views expressed in this publication are those of the authors and not necessarily those of the NHS, the National Institute for Health Research or the Department of Health and Social Care. The Murdoch Children’s Research Institute is supported by the Victorian Government’s Operational Infrastructure Support Program.
Availability of data and code for replication
Example R code for implementing the method, including a worked example on simulated data, can be accessed at the first author′s GitHub repository (![]() ). Data from the Victorian Adolescent Health Cohort Study are not publicly available but those interested in replicating these findings are welcome to contact the study team.
). Data from the Victorian Adolescent Health Cohort Study are not publicly available but those interested in replicating these findings are welcome to contact the study team.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.