
Abstract
The goal of the current study was to understand ethnic differences in use of online health information sources. Social stratification and social diversification hypotheses were used as study’s theoretical framework. The data were obtained from the 2017 Israel Social Survey (N = 2166). Multinomial and logistic regression techniques were used for the multivariate analysis. The results suggest that Israeli Arab respondents were less likely than Israeli-born Jewish respondents to seek health information using the Health Funds’ call centers or websites, other websites, and to utilize any number of the online health information sources. The findings provide a strong support for the social stratification hypothesis. The findings imply that members of minority population should be more encouraged to use (public) online health information sources as a means of taking greater responsibility for their health as well as for the health of their communities.
Keywords
Introduction
Health-related inequalities exist in multicultural societies. In such societies, members of ethnic minorities tend to have poorer health status and limited opportunities for healthcare compared to members of majority group. For the most part, these disparities stem from the minorities’ residing in localities typically marked by poor socioeconomic situation (Saabneh, 2015). In addition, public healthcare policies of such states are not always directed toward improving the health of ethnic minority group members (Daoud et al., 2018).
Israeli society is comprised of two major groups: Jews and Arabs, which reside mostly separately for historical reasons (Daoud et al., 2018). About 8% of Israel’s Arab population resides in a small number of mixed localities (Shdema and Martin, 2022), whereas there are less than 10 such localities in the entire country (Birenbaum-Carmeli and Chassida, 2020). The overwhelming majority (90%) of the Arab population resides in separate localities (Shdema and Martin, 2022). There are approximately 120 such localities in the country, of which only about 10% are midsize cities—the rest are small towns and villages (Alfasi, 2014). Most of the Arab localities in Israel are marked by low socioeconomic status and poor infrastructure and service quality (Daoud et al., 2018).
The residential disadvantages of Israel’s Arab population are reflected in accessing and obtaining healthcare. The 1995 National Insurance Law was legislated to reduce inequalities in health and healthcare, including those based on ethnicity, yet they still exist (Daoud et al., 2018). Saabneh (2015) found the evidence for higher morbidity in the Arab compared to the Jewish population, and Daoud et al. (2018) found that Arabs rated their health lower than Jews did. Even when members of Arab minority seek to maintain or improve their health, their opportunities in this regard are limited, as advanced healthcare services tend to be located in large urban areas (Popper-Giveon and Keshet, 2016).
For already two decades, various technological solutions, including the Internet, have been used for health purposes. However, studies suggest that health-related Internet/social media use is unequally distributed in the general population (Baumann et al., 2017; Finney Rutten et al., 2016; Mesch, 2016; Rosenberg et al., 2021). Given this and the abovementioned inequalities in accessing and obtaining healthcare, ethnic differences in health-related Internet use, and specifically, in use of online health information sources, are likely to appear. Two theoretical concepts from the sociological research can assist in understanding these differences. Social stratification hypothesis claims that technology is an instrument contributing to the expansion of social inequalities. According to this hypothesis, members of the advantaged group in a given society tend to expand the resources they already possess through using technology, thus contributing to the increase in the extent of inequality between them and members of the minority group(s) (Mesch, 2016). In the context of the current study, this hypothesis will postulate that members of ethnic majority group use of online health information sources to a greater extent than members of minority population. In contrast, social diversification hypothesis posits that technological means represent the tools the use of which assists in diminishing of social inequalities. This hypothesis maintains that disadvantages groups in a given society, such as members of ethnic minorities, due to numerous social obstacles they encounter in everyday life, tend to diversify their ways of accumulating resources in order to improve their position in society, also in terms of health. Their social disadvantage therefore motivates them to increasingly use the Internet to obtain these resources (Mesch, 2016) and diversify their social ties (Gonzales, 2017). In the context of the current study, this hypothesis will postulate that members of ethnic majority group use of online health information sources to a lower extent than members of minority population.
It is worth to mention that these theoretical perspectives are not mutually exclusive. Since health-related Internet use is comprised of numerous activities, such as health information seeking or use of online health services, ethnic differences with respect to these phenomena may appear in different directions, therefore confirming each hypothesis, as demonstrated in the study by Mesch (2016).
The current study
This study will draw on the abovementioned hypotheses to explain ethnic differences in utilization of online health information sources. We refer to ethnic differences in the current study as discrepancies between Israeli-born Jewish and Israeli Arab population with respect to the likelihood of utilizing online health information sources.
Both social stratification and social diversification hypotheses were confirmed in the studies on health and Internet (Mesch, 2016; Neumark et al., 2013; Rosenberg et al., 2021). However, these studies did not intend to investigate the utilization of the particular online information sources. To the author’s best knowledge, only a handful of studies has examined ethnic differences in utilization of online health information sources. Study by LaValley et al. (2017) referred to global categories of online health information sources (for instance, commercial, government, and more) while disallowing understanding differences in utilization of particular sources and in the number of such sources used. Study by Finney Rutten et al. (2016) referred to differences in use of the Internet as opposed to healthcare provider, again without referring to particular sources or their number. The current study will fill this gap. The research questions are:
In the current study, ethnic differences were tested regarding health information seeking on the three types of websites: Israel’s Ministry of Health (MoH), Health Funds (HFs), and other websites. MoH is the country’s main authority responsible for the health of the population as well as for health policy. It operates a website where its visitors can find official public healthcare information (Rosen and Waitzberg, 2018). HFs are organizations devoted to providing primary and secondary healthcare to their members (Shmueli et al., 2017). Their websites provide options for accessing tailored medical information, as well as for checking lab results, consulting doctors, and more (Shahrabani and Mizrachi, 2016). Consequently, other websites refer here to any possible website other than that of MoH and those of HFs.
This study is important because it will inform policy regarding inequalities in the use of publicly accessible health information tools. Public healthcare officials can therefore use the study’s findings to encourage members of disadvantaged social groups, such as ethnic minorities, to make greater use of this information and services. Indeed, acquiring health information on the Internet is crucial in self-management of health (Mesch, 2016) as it can benefit health consumers in a number of domains (Finney Rutten et al., 2016), while the digital divide may undermine the access to the information which is (better) accessible online (Kowalski et al., 2014). The results of the study can also help public health officials improve access to health information for ethnic minority populations. This is of special importance during the current pandemic caused by the COVID-19 outbreak, mainly due to a large spread of the coronavirus-related misinformation (Montagni et al., 2021) and a notable vulnerability of ethnic minorities in the face of the pandemic (Haklai et al., 2021).
Method
Data and sample
The data for the current study were obtained from the 2017 Israel Social Survey (Central Bureau of Statistics, State of Israel, 2018), a large representative sample of the Israeli population (Lewin and Stier, 2018). Social surveys are conducted in Israel from January to December each year (Lissitsa and Chachashvili-Bolotin, 2022) by means of face-to-face interviews conducted in Hebrew, Arabic, and Russian languages. The interviews are computer-assisted and last about 1 hour (Levin, 2013). The data for these surveys is collected each year from approximately 7500 individuals aged 20 and older (Lissitsa and Chachashvili-Bolotin, 2022). The population framework includes non-institutional population and residents of non-custodial institutions, such as students residing in university dormitories, immigrants residing in absorption centers (Lissitsa and Madar, 2018). The sample represents about 4.5 million people in the 20+ age bracket (Lissitsa and Chachashvili-Bolotin, 2022). The survey sample is stratified according to seven age groups (20–24, 25–34, 35–44, 45–54, 55–64, 65–74, and 75 years or older), five population subgroups (Arabs—residents of East Jerusalem, Arabs—residents of other parts of the country, immigrants who came to Israel before 1990, immigrants who came at 1990 and onward, and Israel-born Jews), and two sex groups (male and female). The size of each subgroup in the survey reflects the relative size of each subgroup in the overall population of Israel (Pinchas-Mizrachi et al., 2020). The overall response rate in the Israeli social surveys is about 80% (Lissitsa and Chachashvili-Bolotin, 2022).
Typically, social surveys contain a large number of items, part of which (core) are the same across years, and another part (module) changes every year (Lissitsa and Chachashvili-Bolotin, 2014). The module of the utilized survey referred to health and lifestyle (Central Bureau of Statistics, State of Israel, 2017) and included items which referred to utilization of the online sources through which health information can be found. This is why this database served the current study the best.
The overall study sample, that is, 7230 participants (Pinchas-Mizrachi et al., 2020), was further restricted to 2203 respondents who reported engaging in health information seeking during the 12 months prior to survey (item “In the last year, did you search for information about health on your own initiative?”). However, 37 respondents did not belong to any ethnic/immigrant background category used in the current study, so their respondents were discarded. Therefore, the final sample consisted on 2166 Israeli adult health information seekers. It was decided not to further filter the sample by Internet use or any other characteristic as the relevant item asked about its utilization only during the 3 months prior to survey.
Measures
Dependent variables
Number of website types used variable was based on the following multiple response item: “In what ways have you tried to get the necessary information?” This question was asked only among those who reported engaging in health information seeking during the year prior to survey. As mentioned, the study referred only to the online health information sources: MoH website, HF call centers or websites, and other websites. The sum of the used sources was calculated for each respondent. Then the calculated scale was recoded into a nominal variable. The answers of the respondents who looked for health information on any two or all three types of the abovementioned sources were included in the “multiple source” category. The answers of the respondents who mentioned seeking health information on any one of the three abovementioned online sources formed the “single source” category. Consequently, respondents who did not mention utilizing any of the studied sources represented the reference category.
Search on particular sources was measured by three dichotomous variables, which correspond to use of each one of the abovementioned online sources. In each variable, respondents who did not mention that they utilize the respective source represented the reference category.
Independent variable
Ethnic/immigrant background
A series of dummy variables was computed based on the ethnicity variable, which included the main origin groups of Israeli residents: Israeli-born Jews (reference), Israeli Arabs (excluding residents of East Jerusalem), post-1990 immigrants from the former Soviet Union (FSU), post-1990 immigrants who arrived to Israel from other countries (defined in this study as non-FSU-born immigrants), and longtime immigrants who arrived to Israel (from any country) up until 1989. By separating multiple immigrant groups from Israeli-born Jewish group, a more nuanced differences between the Jewish and the Arab groups with respect to the studied phenomena were possible to discover.
Covariates
Gender was defined as a dichotomous variable, with women as the reference category. Age was measured continuously (in years). Level of education was measured as a binary variable, with individuals with non-tertiary (postsecondary or lower) education as the reference category. Marital status was assessed as a binary variable, with unmarried (single, separated, divorced, widowed) as the reference category. Presence of health problem (a binary item “Do you have any health or physical problem, of any kind that has lasted six months or more?”) was assessed dichotomously, with respondents who reported no physical or health problem as the reference category.
Data analysis
Multinomial regression model was utilized to estimate the likelihood of using any number of sources since the dependent variable here consisted of three categories. Logistic regression models were used to estimate the likelihood of using each one of the three particular sources as each dependent variable appeared in a dichotomous form. The findings on the covariates are shown but not discussed. In each model, missing cases were handled by list wise deletion. Each one of the examined models was statistically significant and fitted well to the data. All the analyses were performed in Stata 13 statistical package (StataCorp LP, 2014).
Results
Descriptive statistics
Table 1 describes the study sample.
Sample statistics by ethnic/immigrant background.
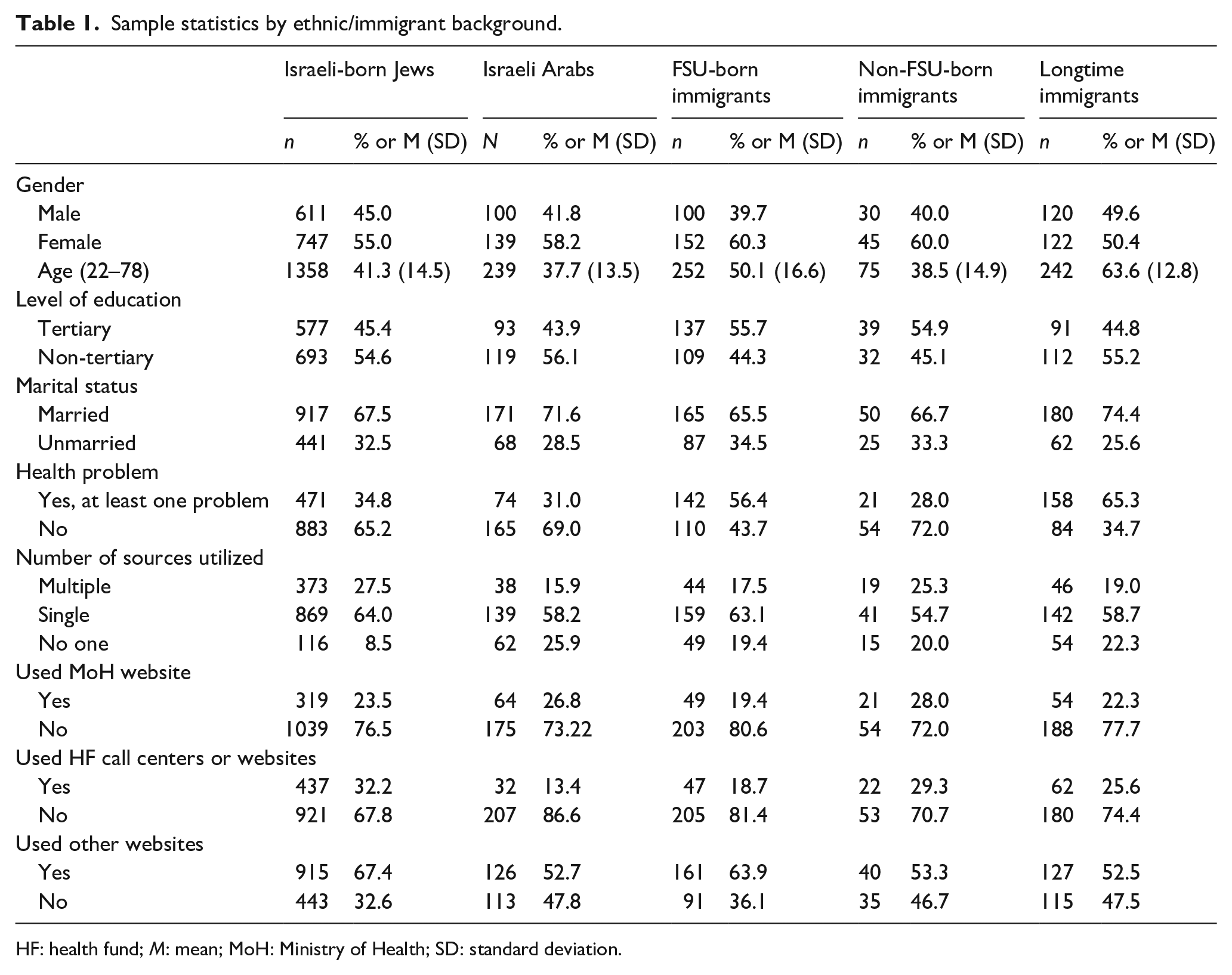
HF: health fund; M: mean; MoH: Ministry of Health; SD: standard deviation.
As the table indicates, among all the groups, the share of men was lower than of women, whereas the lowest figure was observed in the FSU-born immigrant group (39.7%) and the highest—in longtime immigrant group (49.6%). The Israeli Arab group was the youngest (M = 37.7, SD = 13.5), and the longtime immigrant group was the oldest (M = 63.6, SD = 12.8) group among the six. The share of respondents with tertiary education was the lowest in the Israeli Arab group (43.9%) and the highest—in the FSU-born immigrant group (55.7%). In all the groups, most participants were married, but the relevant figure was the highest in longtime immigrant group (74.4%). With respect to health status, the non-FSU immigrant group had the lowest (28%) and the longtime immigrant group had the highest (65.3%) share of individuals with at least one physical or health problem.
With respect to the study outcomes, 15.9% of the Israeli Arab respondents indicated using more than one of the mentioned source types. This is the lowest share of respondents with respect to this category of the variable, whereas the highest share was observed in the Israeli-born Jewish group (27.5%). Israeli Arab respondents were also among the groups with the lowest share of any single source to obtain health information (58.2%), whereas, again, the highest share in this regard was observed in the Israeli-born Jewish group (64%). About 27% of the Israeli Arab respondents searched for health information on the MoH website, whereas the figures for other groups, except for the non-FSU immigrant group, were lower. In contrast, respondents in the Israeli Arab group were characterized by the lowest share of users of the HF websites or call centers (13.4%) among the studied groups.
Multivariable analysis
Table 2 shows the findings of the multinomial regression analysis assessing the likelihood of employing any single as well as multiple sources to obtain health information online.
Results of the multinomial regression analysis estimating the likelihood of utilizing a number of online health information sources.
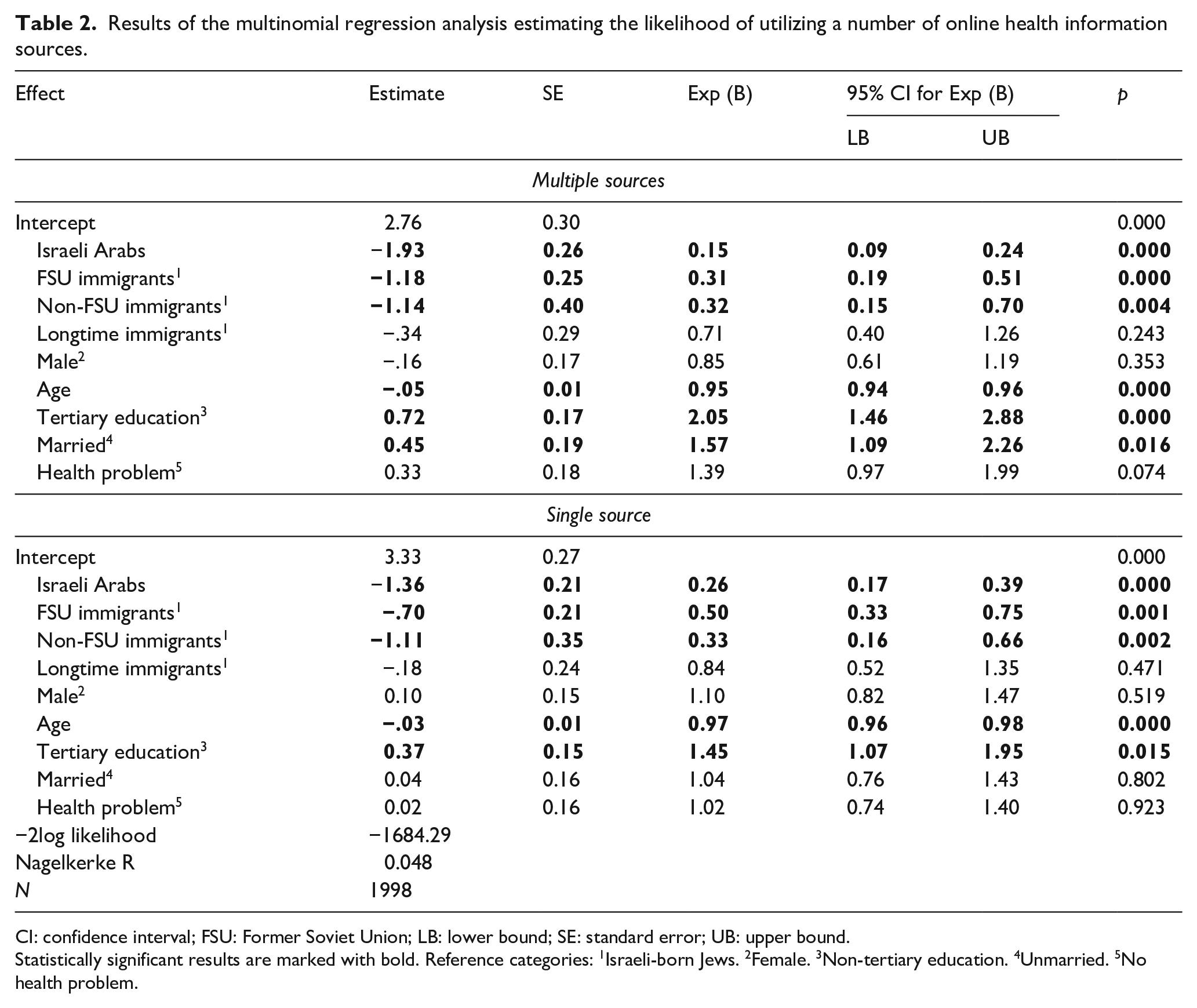
CI: confidence interval; FSU: Former Soviet Union; LB: lower bound; SE: standard error; UB: upper bound.
Statistically significant results are marked with bold. Reference categories: 1Israeli-born Jews. 2Female. 3Non-tertiary education. 4Unmarried. 5No health problem.
It can be seen that after controlling for the covariates, differences between the Israeli Arab and Israeli-born Jewish respondents appeared to be significant. This way, belonging to the Israeli Arab group was negatively associated with utilization of multiple sources for health information seeking (OR = 0.15, p < 0.001). Association to the same direction was found with respect to utilization of any single source (OR = 0.26, p < 0.001).
Other ethnic/immigrant background dummy variables also exhibited associations with the outcome variable. Belonging to the FSU immigrant group was negatively associated with utilization of both multiple (OR = 0.31, p < 0.001) and any single (OR = 0.5, p = 0.001) online health information sources. Belonging to the non-FSU immigrant group was also negatively associated with utilization of both multiple (OR = 0.32, p = 0.004) and any single (OR = 0.33, p = 0.002) online health information sources.
Covariates have also demonstrated several associations with the outcome variable. Age was negatively associated with utilization of both multiple (OR = 0.95, p < 0.001) and any single (OR = 0.97, p < 0.001) sources of online health information. In contrast, having tertiary education was positively associated with utilization of both multiple (OR = 2.5, p < 0.001) and any single (OR = 1.45, p = 0.015) online health information sources. Finally, being married was positively associating with seeking health information using multiple sources only (OR = 1.57, p = 0.016).
Table 3 shows the findings of the logistic regression analysis assessing the likelihood of employing each one of the studied online sources to obtain health information.
Results of the logistic regression analysis estimating the likelihood of using particular online health information sources (N = 1998).
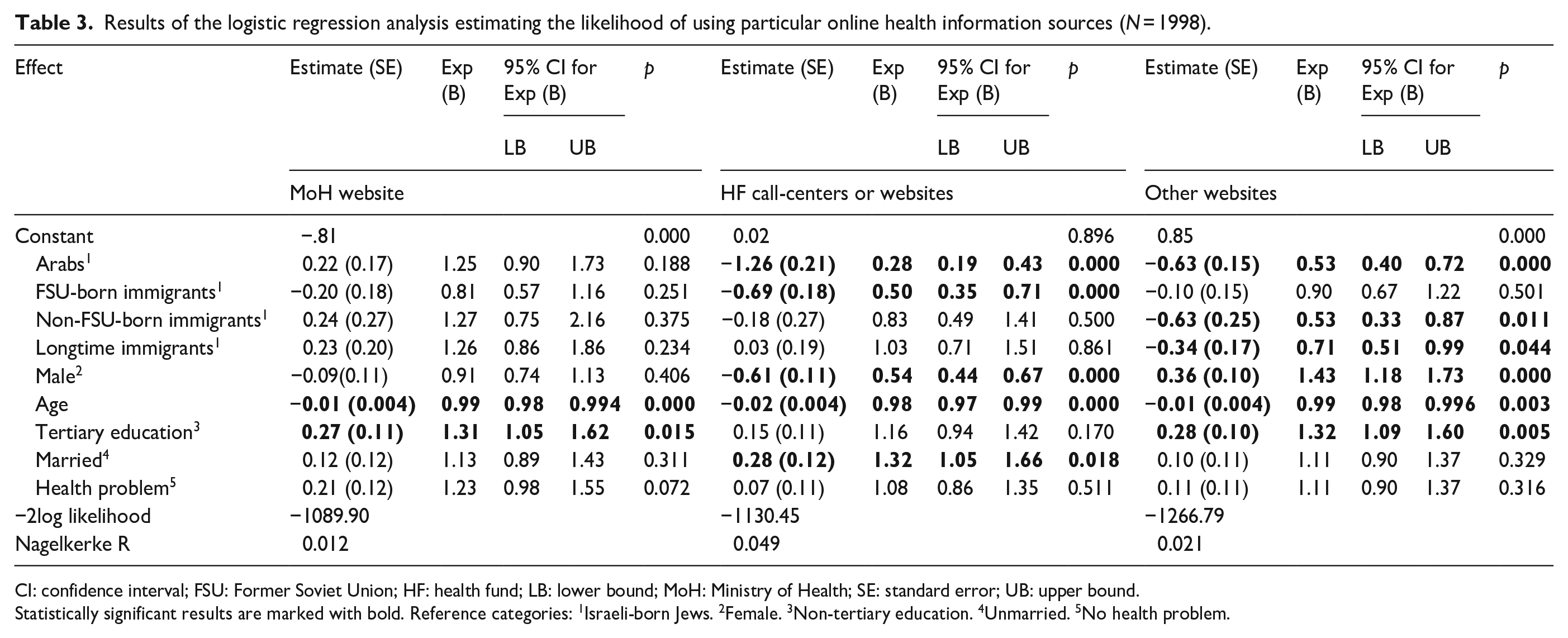
CI: confidence interval; FSU: Former Soviet Union; HF: health fund; LB: lower bound; MoH: Ministry of Health; SE: standard error; UB: upper bound.
Statistically significant results are marked with bold. Reference categories: 1Israeli-born Jews. 2Female. 3Non-tertiary education. 4Unmarried. 5No health problem.
The findings in the table show that belonging to the Israeli Arab group was negatively associated with the use of the HF call-centers or websites (OR = 0.28, p < 0.001) and of other websites (OR = 0.53, p < 0.001).
Only few associations were found between immigrant groups and Israel-born Jewish group in the current analysis. Belonging to the FSU immigrant group was negatively associated with the use of HF call centers and websites (OR = 0.5, p < 0.001). Belonging to the non-FSU (OR = 0.53, p = 0.011) and longtime (OR = 0.71, p = 0.044) immigrant group was negatively associated with using other websites to seek health information.
Covariates also exhibited several associations with the discussed outcome variables. Male gender was negatively associated with the use of HF call-centers or websites (OR = 0.54, p < 0.001), but was positively associated with the use of other websites (OR = 1.43, p < 0.001). Age was negatively associated with the use of each one of the three studied online health information sources. Having tertiary education was positively associated with the use of the MoH website (OR = 1.31, p = 0.015) and of other websites (OR = 1.32, p = 0.005). Finally, being married was positively associated with the use of HF call-centers or websites (OR = 1.32, p = 0.018).
Discussion
The purpose of this study was to examine ethnic differences in utilization of online health information sources through the lens of the social inequality hypotheses. This study was important to conduct in light of scarcity of research investigating these differences in the current context as well as the fact that the existing studies did not investigate phenomena similar to the current research, that is, number of sources used and the identity of the particular sources utilized.
The results of the study provide major support for the social stratification perspective. Israeli Arab respondents were found being less likely than Israeli-born Jewish users to utilize HF call centers and websites and other websites. These findings corroborate those of the study by Mesch (2016), who found that Israeli Arabs use online health services to a lower extent than Israeli-born Jews. These findings may correspond to general underuse of public health services by the Arab population of Israel (Daoud et al., 2018; Saabneh, 2015). The results may suggest that inequalities in the utilization of these services are translated into the online disadvantage. This may also signal digital divide between members of minority and majority groups (Campos-Castillo, 2015) which is translated into inequality in health-related Internet use, as was found in the recent U.S. study (Fareed et al., 2021). It can also be suggested that these factors simultaneously contribute to the found differences to a varying proportion for various individuals belonging to minority group. However, understanding this is beyond the scope of the current study and may serve as a direction for future research.
To further demonstrate the support for stratification perspective, also differences in number of sources used should be referred to. Respondents from the Israeli Arab group were found less likely to utilize both multiple sources as well as any single source of the online health information. This may correspond to lower health literacy of the Israeli Arab population which was confirmed by the previous research (Levin-Zamir et al., 2016). Health literacy, defined as “the cognitive and social skills which determine the motivation and ability of individuals to gain access to, understand and use information in ways which promote and maintain good health” (World Health Organization, 1998: 10), can assist in navigation between numerous online health information sources, cross-checking, and validation of the information. To better understand the factors behind these discrepancies, future quantitative research should employ digital skills and health literacy inventories, whereas qualitative research should provide deeper insights into the reasons for the lower use of the studied sources by Israeli Arab population, also in terms of the health literacy and digital skill discrepancies.
Strengths and limitations
The study has some strengths. First, it has used a large sample allowing a nuanced examination of differences in the use of the online health information sources between the two major ethnic groups in the Israeli society. Second, it has allowed understanding the use of the very particular online health information sources which is typically not the case of the studies in the field (Finney Rutten et al., 2016; LaValley et al., 2017). Third, the coefficients of the differences examined did not reach the 0.001 level thus making the findings reliable and generalizable for the entire population.
With that being said, there are several limitations in the study. First, the study is cross-sectional. Therefore, it cannot be concluded that the study participants utilized particular online sources because of their ethnic background. Second, the study was conducted in Israel. Therefore, generalization of the findings to other settings should be done with care. This is important to note because, for instance, the U.S. study, which investigated the use of several types of online health information sources, found limited ethnic and racial differences in their use (LaValley et al., 2017). Third, the conceptualization of other websites was too general, as they could include hospitals’ official websites, social networking sites (Zhang et al., 2017) as well as commercial and academic websites and search engines (LaValley et al., 2017). The extent of each website use could vary. Therefore, future studies should break down this category into its parts in order to deeper understand the utilization of each source, also compared to other online health information sources. Fourth, due to the relatively small subsample of the Arab population, it was impossible to decouple it by size of locality in order to better understand the disadvantages of this population, as was performed in another study (Rosenberg et al., 2021). Fifth, the use of the health information sources was examined regardless of topics of the information sought. People could extensively seek health information on a particular topic on one source and less on another. Sixth, self-selection and nonresponse biases could have affected the results of the study. Chi-square analysis was performed in order to compare between Arab and non-Arab respondents with respect to the two variables that served for defining the final sample. The difference was significant with respect to both health information seeking during the year prior to participation in the survey (χ2 (3) = 145.93, p < 0.001) and to number of online channels used for that purpose (χ2 (3) = 85.56, p < 0.001). Specifically, more Arab (62.4%) than non-Arab (42.8%) respondents reported not being engaged in health information seeking. In a similar vein, more Arab (84.2%) than non-Arab (71.1%) respondents did not use any online source for health information seeking. However, the prevalence of “unknown” and “irrelevant” options was greater in non-Arab respondents in both examinations. Seven, the explained variance was relatively low, suggesting that other variables, for instance, attitudes toward the studied sources (i.e. quality of information provided by them or its comprehendability), may better explain the variance in the examined outcomes. Finally, the results may reflect the studied period only and therefore may not accurately reflect the current trends, especially in light of the fact that the entire world has been living under the pandemic condition for already more than 2 years about 3 years.
Conclusion
Notwithstanding the limitations, this study has managed to provide a structure of ethnic differences in utilization of online health information sources. From the theoretical point of view, it can be concluded that social stratification hypothesis is a good framework for studying online health-related inequalities. The results of the study provide an evidence for an uneven distribution of the likelihood of health-related Internet use by members of various ethnic groups in a given society, whereas ethnic minority appears to be disadvantaged in the studied regards. From the practical point of view, the findings may serve as a call for action for healthcare professionals, authorities and other specialists in public healthcare domain. Increasing awareness of the public health information websites, better explanation of their features and advantages, better language and cultural adaptation, as well as underscoring the importance of using numerous health information sources, could assist in minimization of these discrepancies. This is of special importance with respect to the HF websites. Since HFs are responsible for provision of primary and secondary healthcare to their members (Shmueli et al., 2017), their lower use by Israeli Arab residents, which is generally disadvantaged in terms of obtaining healthcare (Daoud et al., 2018; Saabneh, 2015), may prevent them from getting necessary information and services in order to maintain or improve their health.
Health information professionals have a responsibility to participate in preparation of the abovementioned campaigns. They should ensure that only verified and up-to-date information about the MoH and the HF websites is included in these campaigns. They should also ensure that all possible features, as well as all advantages of the website use, are listed. In addition, they can support medical staff, research teams and decision makers by drawing attention to the latest developments of these websites.
Footnotes
Acknowledgements
Thanks is provided to Mrs. Donna Bossin for a proof reading of the article.
Declaration of conflicting interests
The author declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Ethics approval statement
This study used the secondary data. Therefore, no ethnical approval needed.