
Abstract
Recent government initiatives to deploy health information technology in the USA, coupled with a growing body of scholarly evidence linking online heath information and positive health-related behaviors, indicate a widespread belief that access to health information and health information technologies can help reduce healthcare inequalities. However, it is less clear whether the benefits of greater access to online health information and health information technologies is equitably distributed across population groups, particularly to those who are underserved. To examine this issue, this article employs the 2007 Health Information National Trends Survey (HINTS) to investigate relationships between a variety of socio-economic variables and the use of the web-based technologies for health information seeking, personal health information management and patient-provider communication within the context of the USA. This study reveals interesting patterns in technology adoption, some of which are in line with previous studies, while others are less clear. Whether these patterns indicate early evidence of a narrowing divide in eHealth technology use across population groups as a result of the narrowing divide in Internet access and computer ownership warrants further exploration. In particular, the findings emphasize the need to explore differences in the use of eHealth tools by medically underserved and disadvantaged groups. In so doing, it will be important to explore other psychosocial variables, such as health literacy, that may be better predictors of health consumers’ eHealth technology adoption.
Introduction
Fueled by advances in information and communication technologies, government and non-profit organizations in the USA are taking steps to help close gaps in access to healthcare information and communication. In particular, the American Recovery Reinvestment Act of 2009 authorizes government spending of close to $38 billion over the next 10 years to support health information technology deployment and adoption—demonstrating the federal government’s commitment to improving access to healthcare via health information technology. Moreover, the government’s current ‘Healthy People 2020’ proposal emphasizes equitable access to health information and improved health communication as key strategies for bridging health disparities and consequently for improving health outcomes. 1 These initiatives are backed by growing empirical evidence linking increased access to health information via the Internet to overall improved health knowledge, better lifestyle choices, better compliance with physician recommendations and improved patient-provider communication during clinic visits, leading to overall improved therapeutic alliance.2–6 The underlying contention of these initiatives is that ensuring better access to health information and health information technologies can help reduce healthcare disparities.
Despite this push for increased access to health information, it is still unclear whether the benefits of online access will be demonstrated equitably among health consumers in the USA, particularly among the medically underserved and disadvantaged. A recent report released by the Pew Internet and American Life Project reveals that 70% of non-Hispanic Blacks and 64% of Hispanics have access to the Internet, while 52% of non-Hispanic Blacks and 47% of Hispanics have broadband access from their homes. 7 This is encouraging evidence of the shrinking digital divide in web, broadband and mobile technology access. Considering that health disparities are typically drawn along the same lines as socio-demographic inequalities, such as ethnicity, household income, levels of education and place of residence (rural vs urban), it would be reasonable to assume that the shrinking divide in Internet access will result in increased use of online health information sources and other healthcare technologies [i.e. personal health records (PHRs)] by disadvantaged populations.
This article reports on current trends in web use for health information and communication of a nationally representative sample of Americans. In particular, it examines relationships of health consumers’ use of web resources/technologies for health information seeking, personal health information management and patient-provider communication. This article also discusses the implications of these trends on consumer health informatics initiatives in the USA, as well as on the evaluation of health consumers’ eHealth technology adoption.
The following section discusses the importance of online health information seeking, personal health information management and patient-provider communication in relation to health outcomes.
Online health information seeking
Public access to medical and health information has increased exponentially in the last decade, with a variety of health information resources, self-management and risk- assessment tools being made more readily available via the Internet. Nationally representative surveys have illustrated the growing popularity of the Internet as a health resource, with more than three-quarters of the American population going online for health information.8–10
These trends illustrate how health consumers are becoming increasingly pro-active in their healthcare. Research shows that a growing number of patients bring health information resulting from their own searches to their doctor appointments.11–14 Iverson et al. 15 found that online health information searches conducted before consultations with doctors had a reassuring effect on patients and helped ameliorate patient confusion as a result of information overload.
While knowledge alone cannot predict individual behaviors, information-seeking is recognized to be a vital activity toward achieving health behavior change. 16 Shim et al. 2 found a significant relationship between active health information scanning and screening, and cancer knowledge, lifestyle choices and screening behaviors (e.g. colonoscopy, mammography and prostate cancer screening). Kalichman et al. 4 found significant associations between the use of the Internet to search for health-related information and self-efficacy for information-seeking, problem-focused coping and greater social support. Other studies have found significant relationships between information- seeking and improved patient-provider communication 5,6 and medical decision-making.17–19 In particular, Iverson et al. 15 found that seeking health information online increased patients’ interest in their own health, encouraged patients to ask more questions during doctor visits and improved levels of compliance with doctors’ recommendations.
Personal health information management
Advances in computing technologies have also vastly improved patients’ ability to manage their personal health information. Today, health consumers have to manage a wide array of personal medical information, including health histories, medications and treatments, as well as financial information, such as insurance procedures, medical fees and employee health-related benefits. The challenge of managing personal health information is compounded by the complex, often fragmented, system of care patients must increasingly learn to navigate. 20 As a result, medical data is often distributed across different clinicians, specialists and institutions in a variety of formats, most of which are currently paper-based. Keeping accurate medical records and having ready access to these records is especially important for the chronically ill who have to deal with a wide variety of health information from numerous healthcare providers and institutions over time.21,22
A number of web-based tools (i.e. patient health records, patient health portals, etc.) are now readily available to patients for managing their health information, allowing patients to assume greater responsibility for assuring the quality of the healthcare they receive by helping improve the accuracy, completeness, accessibility and portability of their health records. 23 Integration with electronic medical records systems within standardized and secure health information exchanges multiply the benefits of these patient tools, 24 but also increase the complexity of these systems and may consequently affect widespread adoption across different population groups.
Use of web technologies for patient-provider communication
The effects of the quality and quantity of patient-provider communication on health outcomes are well documented in the literature.25–27 A systematic review found that effective patient-provider communication helps improve emotional health, symptom resolution, function, physiologic measures (i.e. blood pressure and blood sugar level) and pain control. 28 Moreover, the efficacy of health education and self-management programs have been found to improve when they included tools for supporting communication and careful coordination with healthcare professionals.29,30
The past decade has seen an explosion in the deployment of communication technologies (e.g. e-mail, text messaging, interactive video response, etc.), providing a wider array of synchronous and asynchronous communication modes to support patient-provider communication. While adoption of online communication has been relatively slow in healthcare practices, providers and patients alike generally have positive attitudes towards the use of these technologies.31–38 Moreover, despite persistent concerns about the added burden of supporting online communications, as well as about security and privacy issues, studies have shown that patients rarely communicate via e-mail with their doctors regarding issues requiring immediate attention, or include sensitive information within their messages. 31 Content analyses of e-mail exchanges between patients and providers have revealed that typical e-mail enquiries focus on non-acute issues and are telling of patients’ desire to develop better relationships with their doctors.38–43
Access to and use of eHealth technologies
The previous section highlights growing evidence linking health outcomes with patients’ use of eHealth technologies for information seeking, communicating with their physicians and managing their medical information. However, as exciting as the advancements in eHealth tools are, there have been overly optimistic predictions that greater access will redound to widespread use. Most telling are current initiatives backed by millions of federal dollars to improve access to healthcare information and communication, particularly via increasing Internet access in the home and improving broadband access in under-resourced communities, such as rural areas. Early evidence of progress on these various initiatives is encouraging. A recent report by the National Telecommunications and Information Administration reveals that, in 2010, more than two-thirds (68.2%) of households in the USA enjoyed broadband Internet access at home—an increase of almost five percentage points since 2009 (63.5%) and more than 17 percentage points since 2007. 44 The report also reveals narrowing gaps in usage among users of different education levels and among urban versus rural users. In particular, broadband adoption by users with annual family incomes of between $15,000 and $25,000 grew from 35.2% in October 2009 to 42.6% in 2010. In contrast, the adoption rate for families earning between $100,000 and $149,000 annually increased by only 1% during the same period (from 84.9% to 85.5%). Similarly, rural broadband usage increased from 38.8% in 2007 to 60.2% in 2010. 44
Access has increased, not only in terms of Internet access in the home, but also in public places, such as libraries and schools, as well as in the workplace. However, despite increased access to technology, underserved populations (e.g. minorities, elderly, patients living in rural areas, etc.) continue to face significant barriers to accessing, or using, health information.45–49 Aside from differences in eHealth technology use related to ethnicity, education and income, other aspects of the digital divide have surfaced related to geography, computer and health literacy, disability, availability of eHealth services and local infrastructure requirements, to name but a few.45,50 For example, in a study of cancer patients, Welch Cline et al. 51 concluded that general and health literacy, the ability to evaluate website and information credibility, and Internet search and navigational skills—factors associated with socio-economic status and health disparities—were also associated with greater web use for health information seeking and communication.
Efforts to monitor eHealth use over the years, particularly in the USA, are essential in ensuring that current initiatives to increase access are accompanied by appropriate interventions to ensure that everyone, including underserved populations, are able to obtain, process and understand health information.
This study investigates differences in web technology use for health-related information seeking and communication using a nationally conducted survey of a cross-section of the USA. Population estimates are projected through the analysis of weighted samples, providing a high-level view of patterns in eHealth diffusion among different population groups.
While results of this analysis will have meaningful implications for policy related to health information technology in the USA, it also yields important insights that will be useful in examining eHealth technology adoption in under-resourced, developing countries, where digital divide issues are even more pronounced.
Method
We conducted an analysis of the 2007 Health Information National Trends Survey (HINTS; available at: www.hints.gov). HINTS has been conducted biennially by the Health Communication and Informatics Research Branch of the U.S. National Cancer Institute since 2003. The survey aims to collect representative data to provide updates on the changing patterns, needs and information opportunities in health among adults in the USA. 52 While both telephone and paper-based surveys were conducted, only respondents who completed the mailed questionnaires were included in this analysis. Mail questionnaires included a stratified sample from a list of addresses that over-sampled minorities. While officially recognized as the 2007 HINTS dataset, the data for this survey were actually collected between January and May 2008. Questionnaires, which consisted of three sections, were disseminated in English and Spanish. A total of 3473 complete and 109 partially complete surveys were received, representing 2581 households. A questionnaire was considered complete if at least 80% of each section was filled in. Questionnaires with less than 50% of a section completed were discarded. The response rate was 32.9%. The sampling design for HINTS datasets and design of the HINTS survey instrument are described in more detail elsewhere.53–55 HINTS is one of the most comprehensive national-level datasets currently in existence. Research is conducted and findings published on various areas of health behavior and communication for several years after each successive survey. For example, a recent article by Lathan et al. used data from the 2005 HINTS to examine potential racial differences in the perception of lung cancer. 56
Measures of interest
Socio-economic characteristics
Using PASW 18.0 (SPSS, Chicago, IL, USA), socio-economic variables were either dichotomized or dummy coded in order to calculate odds ratios in logistic regression analysis. Gender was coded simply as either ‘male’ or ‘female’. Originally, the race/ethnicity measurement was Hispanic, White, African-American, American-Indian, Asian, Hawaiian and Other. This variable was recoded to represent self-reported Caucasians and non-Caucasians. For education, there were originally seven discrete possibilities representing education levels from ‘less than 8 years’ to ‘post graduate’. This variable was recoded to account for those who reported attending at least some college, compared to those who had not. Age differences were re-coded to reflect different generational user groups: Generation Y, Generation X, Baby Boomers and the Silent Generation. The ‘Silent Generation’ refers to respondents born between 1925 and 1945 and ‘Baby Boomers’ refers to respondents born between 1946 and 1964. 57 Ortner classified ‘Generation X’ as individuals born between 1965 and 1976. 58 Nineteen sixty-five was the first year that the birthrate began to drop after the baby boom and 1977 was the first year that the birthrate began to rise again. ‘Generation Y’ refers to respondents born after 1976. In turn, the following generational age groups of the respondents were calculated subtracting the noted years of each generation group from 2008: Generation Y, less than or equal to 31 years old; Generation X,32–43 years old; Baby Boomers,44–62 years old; and finally, Silent Generation, 63 years and older.
Rural versus urban residency
Respondents were matched to their counties based on their mailing addresses. Responses were then coded as either urban (>250,000) or rural (<250,000) based on the rural-urban continuum codes suggested by the Economic Research Service and the United States Department of Agriculture. Thus, this was a dichotomous variable.
Numeracy
Health literacy was measured using a proxy variable based on numeracy. Respondents indicated their comfort with, and their ability to understand, medical statistics using a four-point scale, with responses ranging from ‘Easy’ or ‘Very easy’, to ‘Hard’ or ‘Very hard’. The researchers noted that numeracy, as operationalized in the HINTS dataset, only represents one dimension of health literacy. Nevertheless, it was decided to include this in the analysis to explore potential relationships between numeracy and health information technology (HIT) use.
Internet access
Respondents were asked a general question regarding whether they ever went on-line to access the Internet or World Wide Web, or to send and receive e-mail. Respondents that indicated a positive response were asked a follow-up question that focused on the location of their Internet access. Possible locations included: home, work, school, public library, community center, someone else’s house and some other place. This measure of location of access was then recoded into a dichotomous variable to compare respondents who access the Internet from their home to those who did not. As a caveat, the absence of at-home access did not necessarily mean that the respondents were completely without Internet access itself.
Dependent variables
Internet exposure
Previous exposure to the Internet from any location was assessed using a single dichotomous item: “Do you ever go on-line to access the Internet or World Wide Web, or to send and receive e-mail?”
Health information seeking
Health information seeking from any source was also measured with a single dichotomous item: “Have you ever looked for information about health or medical topics from any source?”
Online health information seeking
Respondents were asked to indicate what source they consulted first in their most recent search for health-related information. They were given 13 different options including books, family, friends, healthcare provider, newspaper, magazine, the Internet and other sources. To facilitate logistic regression, this variable was dichotomized into those who used the Internet first vs all other non-Internet sources.
Personal health information management
Personal health information management was assessed using a single dichotomous item: “In the past 12 months, have you used the Internet to keep track of personal health information, such as care received, test results, or upcoming medical appointments?”
Patient-provider communication via the Internet
Finally, patient-provider communication was measured using a single dichotomous item: “In the past 12 months, have you used e-mail or the Internet to communicate with a doctor or a doctor’s office?”
Data analysis
Data was coded in PASW 18.0, saved and imported into SAS 9.2 (SAS, Cary, NC, USA) to facilitate analysis of the weighted data. Multivariable logistic regression was utilized to examine the characteristics of respondents associated with five different behaviors: (1) experience with the Internet; (2) searching for health information from any source; (3) using the Internet first to find health information; (4) personal health information management using the Internet; and, (5) use of the Internet to communicate with a healthcare provider. Logistic regression has been previously used to analyze earlier HINTS datasets that used the same weighting scheme. 56 In all analyses, post-stratification weights were used to account for the survey design and sampling using the PROC SURVEYLOGISTIC procedure in SAS 9.2. The HINTS 2007 dataset provides weighted samples calculated from a set of 50 replicate sampling weights specifically for mailed surveys. Jack-knife weights allow for more accurate estimations of variance which, in turn, affect standard errors, p values and confidence levels when doing inferential statistical analysis. This statistical technique has been used in various analyses of HINTS as a method of approximating a general population from the sample data and lower the variance of the data.55,59,60
Independent dichotomous variables were created for generation variables as it was a categorical measure. Therefore, ‘Generation Y’ was left out of the regressions as it was considered the baseline category for generational use group.
To check for multi-collinearity, each case was weighted by its final weight (MWGTO) and the five logistic regressions were modeled as linear regressions computing collinearity diagnostics including variance inflation factor and tolerance statistics in PASW 18. Out of the five regressions, the lowest tolerance calculated was approximately 0.645. Furthermore, the highest tolerance statistic was approximately 1.544. Multi-collinearity, which may attenuate p values and adversely affect confidence intervals,61,62 is most likely present when VIF statistics are greater than 10 and tolerance statistics are less than 0.1. Therefore, the collinearity statistics of these five models suggest that the regression results are sound.
Results
The 2007 HINTS dataset includes 3473 completed mailed surveys and 109 partially completed surveys. Table 1 summarizes the independent socio-economic variables of the sample population. Table 2 summarizes the dependent variables used in the logistic regressions. The weighted percentages demonstrate the appropriate estimations of the sample population.
Summary of Socio-Economic Characteristics of Respondents
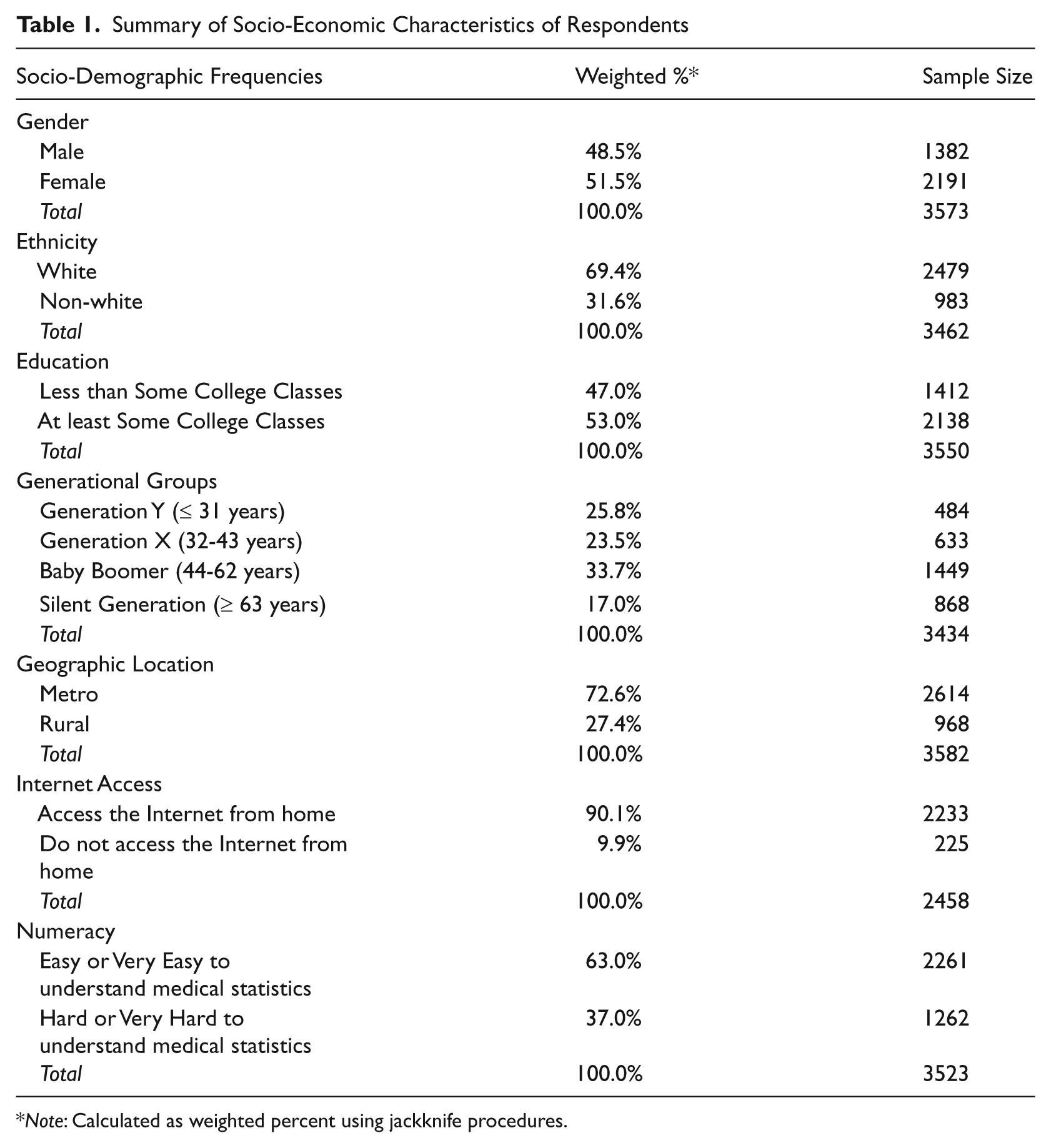
Note: Calculated as weighted percent using jackknife procedures.
Summary of dependent variables in regression analyses
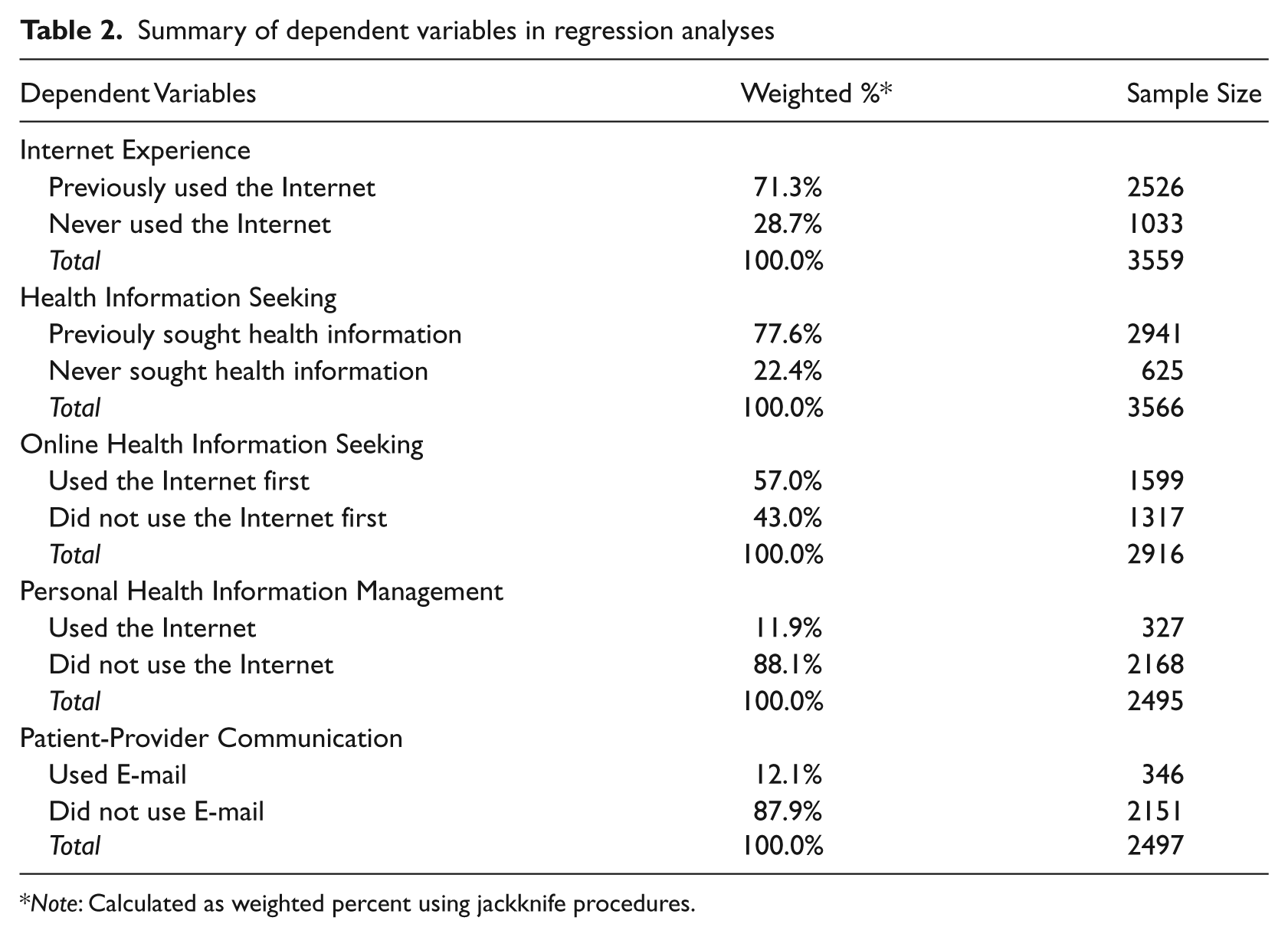
Note: Calculated as weighted percent using jackknife procedures.
Internet Exposure: Do you ever go on-line to access the Internet or World Wide Web, or to send and receive e-mail? (Yes = 2422, No = 873)
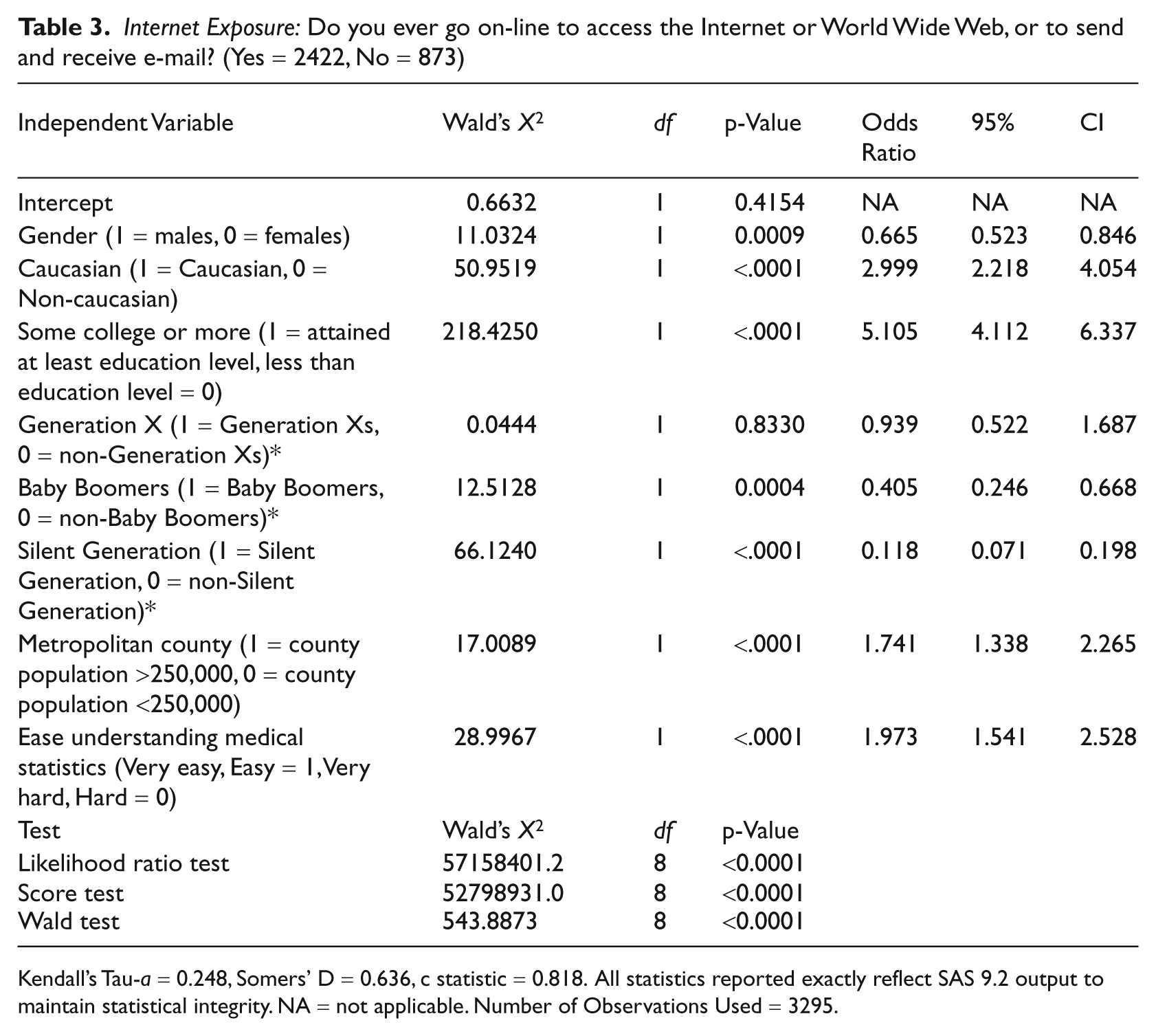
Kendall’s Tau-a = 0.248, Somers’ D = 0.636, c statistic = 0.818. All statistics reported exactly reflect SAS 9.2 output to maintain statistical integrity. NA = not applicable. Number of Observations Used = 3295.
Health Information Seeking Have you ever looked for information about health or medical topics from any source? (Yes = 2133, No = 216)
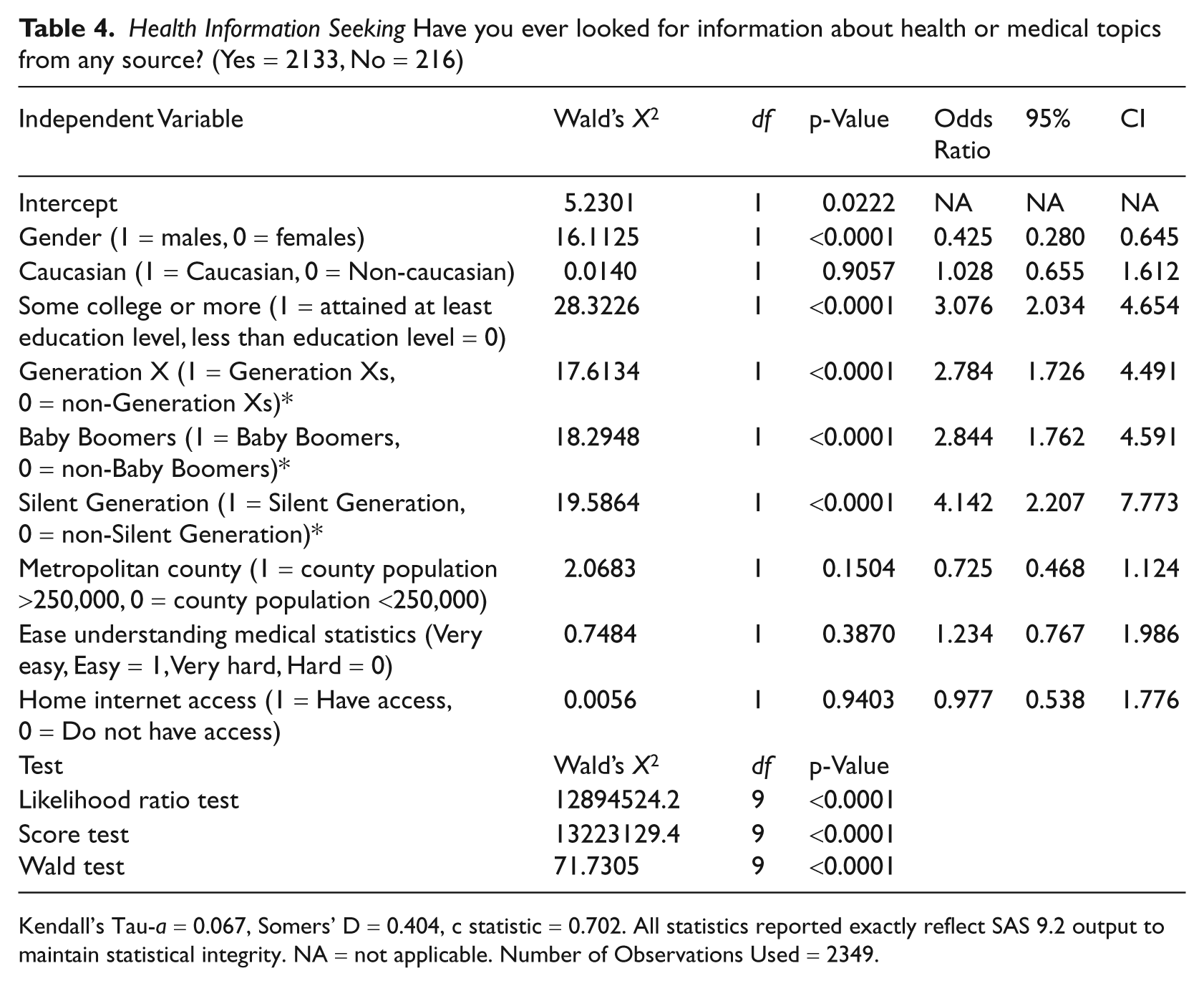
Kendall’s Tau-a = 0.067, Somers’ D = 0.404, c statistic = 0.702. All statistics reported exactly reflect SAS 9.2 output to maintain statistical integrity. NA = not applicable. Number of Observations Used = 2349.
Notably, when this data was collected, approximately 71% of respondents had previously used the Internet. Furthermore, 90% of those with Internet experience had access from home.
Internet exposure
Several of the socio-economic status (SES) variables in the model were significant predictors of individuals’ experience with the Internet. Males were less likely (OR = 0.665; CI = 0.523-0.846) than females to have ever used the Internet. Caucasians were three times more likely (OR = 2.999; CI = 2.218-4.054) than non-Caucasians to have accessed the World Wide Web. Baby Boomers were less likely (OR = 0.405; CI = 0.246-0.668) than Generation Y users to have ever accessed the Internet. Furthermore, the confidence intervals for each dichotomous variable are centered on an odds ratio. If confidence intervals of odds ratios do not overlap in regression analysis, then it is assumed that the independent variables have statistically significant odds ratios. Therefore, the confidence intervals suggest that Silent Generation users (OR = 0.118; CI = 0.071-0.198) were less likely than Baby Boomers to access the Internet. After calculating the inverse of the Silent Generation odds ratio, we determined that Generation Y individuals were eight times (OR = 8.475) more likely to access the Internet than the oldest generation. Urban residents (e.g. individuals living in metropolitan counties with populations larger than 250,000) were significantly more likely to have accessed the Internet than individuals residing in rural counties (OR = 1.741; CI = 1.338-2.265). Lastly, individuals who reported that it was ‘Easy’ or ‘Very easy’ to understand medical statistics (OR = 1.973; CI:1.541-2.528) were almost twice as likely to have accessed the Internet compared to those who reported that it was ‘Hard’ or ‘Very hard’.
Health information seeking
Similar to Internet exposure, numerous demographic variables were predictors of health information seeking behavior from any source. Compared to females, males were significantly less likely (OR = 0.425; CI = 0.280-0.645) to have searched about health or medical topics from any source. Individuals who had attended some college classes (OR = 3.076; CI = 2.034-4.654) were three times more likely to have sought health information than individuals who did not attend college. Not surprisingly, Generation X individuals (OR = 2.784; CI = 1.726-4.491), Baby Boomers (OR = 2.844; CI = 1.762-4.591) and Silent Generation individuals (OR = 4.142; CI = 2.207-7.773) were all significantly more likely to have sought health information than Generation Y individuals.
Online health information seeking
Education, age and home Internet access were significant factors associated with using the Internet first during their most recent search for health information. Individuals with some college background (OR = 1.668; CI = 1.218-2.285) were more likely than those who had not attended college to have first used the Internet to search for health information (Table 5). Members of the Silent Generation were less likely (OR = 0.291; CI = 0.187-0.452) than Generation Y individuals to first use the Internet for health information. Additionally, the confidence intervals suggest that Silent Generation users were also less likely than Generation X users (OR = 0.715; CI = 0.471-1.086) to use the Internet as their first source of health information. The data also indicate that individuals with home Internet access were significantly more likely (OR = 1.683; CI = 1.064-2.661) to have first used the Internet to search for health information.
Online Health Information Seeking Did you use the Internet first during your most recent search for health information? (Yes = 1459, No = 658)
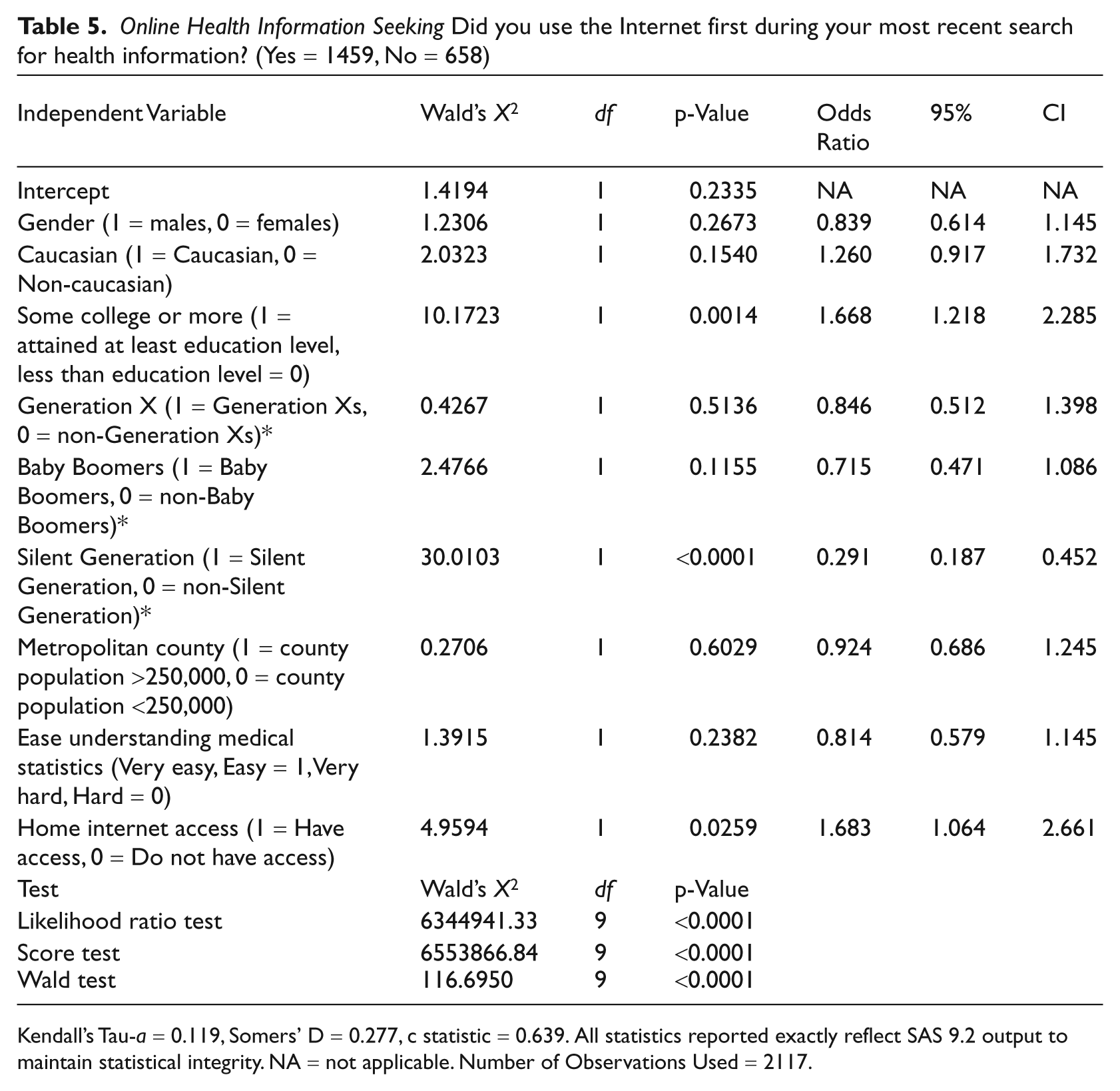
Kendall’s Tau-a = 0.119, Somers’ D = 0.277, c statistic = 0.639. All statistics reported exactly reflect SAS 9.2 output to maintain statistical integrity. NA = not applicable. Number of Observations Used = 2117.
Personal health information management
About 12% of respondents indicated that they had used the Internet for personal health information management (Table 6). While none of the socio-economic variables were found to be significant predictors of this dependent variable, researchers may wish to investigate the differences in usage by ethnicity in future studies. In the current study, Caucasians were found to be marginally more likely (at p < 0.10) than non-Caucasians to use web-based technologies for personal health information (OR = .709; CI = 0.499-1.006; p = 0.0542).
Personal Health Information Management Have you ever used the Internet to keep track of personal health information? (Yes = 302, No = 2034)

Kendall’s Tau-a = 0.030, Somers’ D = 0.135, c statistic = 0.567. All statistics reported exactly reflect SAS 9.2 output to maintain statistical integrity. NA = not applicable. Number of Observations Used = 2336.
Patient-provider communication via the Internet
Gender, education and geographic location were all significant predictors of Internet use to communicate with a doctor or doctor’s office in the past 12 months (Table 7). Males were less likely (OR = 0.648; CI = 0.459-0.913) than females to have used e-mail to communicate with their doctors. Additionally, individuals who had previously attended some college classes (OR = 1.453; CI = 1.005-2.101), or who lived in urban counties (OR = 1.835; CI = 1.175-2.866), were significantly more likely than individuals who had no college background, or who lived in rural counties, to communicate with their primary care provider via e-mail. Notably, home Internet access was not a significant predictor of patient-provider communication via the Internet.
Patient-Provider Communication via the Internet In the past 12 months, have you used e-mail or the Internet to communicate with a doctor or doctor’s office? (Yes = 328, No = 2010)
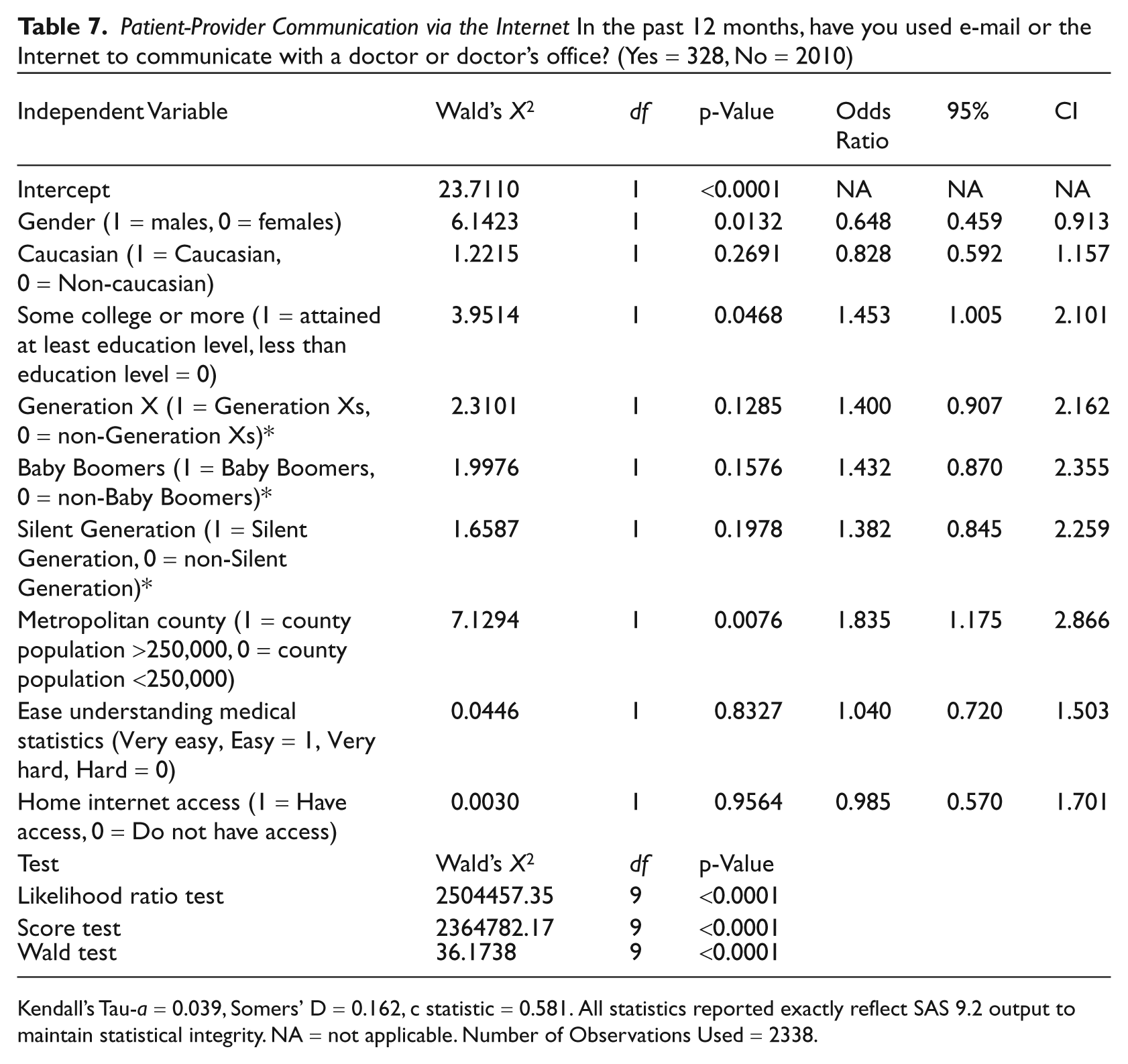
Kendall’s Tau-a = 0.039, Somers’ D = 0.162, c statistic = 0.581. All statistics reported exactly reflect SAS 9.2 output to maintain statistical integrity. NA = not applicable. Number of Observations Used = 2338.
Discussion
In recent years, significant attention has been paid to making financial investments in developing a more robust strategy for increasing usage of HIT within the USA. One foundational component for expanding the adoption and use of HIT was supported by the American Recovery and Reinvestment Act of 2009 (ARRA) through its funding to expand broadband services to previously underserved populations, such as those in rural and inner-city areas. ARRA provided programs in the National Telecommunications and Information Administration (NTIA) and Rural Utilities Service (RUS) with $7.2 billion to expand access to broadband service in the USA. 63 The NTIA’s Broadband Technology Opportunities Program (BTOP) was provided $4.7 billion to support: 1) the expansion of community infrastructures to connect so-called anchor institutions, such as healthcare providers, schools, libraries and public safety facilities; 2) the development, or enhancement, of public computer centers to provide access to low-income individuals, the unemployed, seniors, minorities and people with disabilities; and, 3) sustainable broadband use and adoption through the use of digital literacy training and outreach programs to these same target populations. 64 Such investments show an overt attempt to facilitate bridging of the so-called digital divide by providing the availability of broadband services where previously unavailable.
The analysis presented here is a useful starting point for evaluating progress on these government initiatives. Analysis of the 2007 HINTS dataset summarizes trends on a number of variables of interest given specific targets of HIT use by health consumers as outlined in the abovementioned initiatives. Like most datasets studying eHealth trends in the USA, HINTS includes a wide array of items measuring technology use for health information seeking, but also has a number of variables (albeit still limited) exploring eHealth technology use for personal health information management and patient-provider communication. So, while there is a number of datasets available that explores characteristics of online health information seekers, there are still limited datasets that touch on other uses of eHealth, such as health information management and communication with health providers. Therefore, analysis of this nationally-representative dataset reveals important implications for developing patient-oriented interventions, as well as for developing more comprehensive instruments for tracking progress.
As a start, this analysis confirms growing evidence of a narrowing divide in general computer ownership and Internet access in the USA, with approximately 71% of the respondents indicating experience using the Internet, 90% of whom reported having accessed the Internet from their homes. This is interesting in light of the fact that these overall trends were already in place before the implementation of aggressive strategies currently being pursued in the United States to help narrow access gaps to underserved populations.
While there are widespread assumptions about how closing gaps in broadband access will result in greater HIT use, the literature reveals that this is not necessarily the case, particularly for groups that already experience the greatest disparities in healthcare. 7 Numerous studies confirm prevailing patterns in health information seeking, with white, younger and better-educated individuals in urban areas being more likely to use web resources than non-white, older and less educated users in rural areas.46,51,65–67
Our analysis shows less clear patterns in disparities in online health information seeking and reveals a preliminary analysis of disparities regarding eHealth use for communication and patient health information management. Internet access was found to be a significant predictor of online health information seeking, but was not significantly related to e-mail communication with providers or HIT use for personal health information management. This finding is not necessarily surprising given the limited availability of institutional support for, and infrastructure to support, e-mail communication or PHRs management at the time these data were collected. Over time, it will be interesting to track health consumers’ use of these tools, particularly as resources for supporting these services become more widely available in the USA.
As with previous studies, age and education were found to be significant predictors of online health information seeking in that younger respondents with some college education were significantly more likely to use the Internet for seeking health information. However, neither of these variables significantly influenced technology use for personal health information management. Education and gender were found to be significant predictors of web-based communication, with female and more educated respondents being more likely to communicate with their providers via e-mail.
Perhaps most notable among our findings is the lack of consistent evidence regarding disparities in eHealth use, particularly in relation to rural vs urban, Caucasian vs non-Caucasian and health-literate vs less health-literate differences. These findings are interesting given consistent evidence in the literature citing significant differences in eHealth use along these divides that closely mirror disparities in health status, healthcare, and, consequently, health outcomes.22,68–71 Significant racial disparities in health IT use, however, were not observed in this dataset except for marginal differences in the use of web-based technologies for personal health information management.
Rural communities have been shown to disproportionately demonstrate greater disparities in access to healthcare facilities and medical specialists, which is why the initiative to improve broadband connections in such areas is high on the USA government’s priority list. A previous study based on an analysis of the 2005 HINTS dataset found that rural residents conducted significantly less health-related activities online compared to urban residents—a trend that was exacerbated by differences in socio-economic status within these communities. 32 However, the current analysis of data from the 2007 HINTS survey presents a less clear picture of rural vs urban differences in the use of online technologies for health information seeking and communication. Rural-urban differences were only found to be significantly more noticeable in the use of web-based communication with providers. Specifically, urban residents were significantly more likely than rural residents to communicate with their physicians via e-mail. Rural vs urban residents, however, did not significantly differ in their use of web-based resources for health information or the use of patient health information management tools.
The lack of statistically significant predictors for the use of eHealth tools for personal health information management is a finding that may in itself prove to be worth examining in future studies. The relatively small percentage (11.9%) of respondents who indicated using online PHRs at the time of this study, coupled with how the multivariate model was operationalized, may make isolating such relationships difficult. Further examination of trends in patient use of such tools is a primary area of concern given the current push by the USA to develop large-scale health information exchange networks, particularly in under-resourced settings. Clearly, this emphasis on improving access to high-speed broadband by rural, economically less well-off segments of the population must be accompanied by interventions to encourage the exchange of health records, not only by healthcare providers such as hospitals, clinics, and physician practices, but also by patients.
Implications
These findings emphasize two primary observations and insights for future investigations. First, as gaps in computer ownership and Internet access in the USA continue to narrow, it will be increasingly important to track disparities in adoption on a wider range of variables beyond the usual subjects (e.g. race, rural-urban differences). This analysis presents interesting results that show patterns in disparities not completely in line with findings from the literature. Whether this represents a tipping point in eHealth technology use across different population groups as a result of broadening access, or a revelation that, as these gaps narrow, other, more salient, underlying factors affecting adoption may become more prominent, needs further exploration. Certainly, there is a need for more comprehensive measures for tracking use that take into account not only other eHealth activities such as personal health information management, but also potential predictor variables such as health literacy and other psychosocial variables. For example, in a previous survey of a low-income, elderly population, Kim 72 found that use of PHRs was significantly associated with the availability of assistance and technical support, while limited or non-use of PHR systems was highly associated with poor computer and Internet skills, technophobia, low health literacy and limited physical/cognitive abilities.
A second observation relates to the need for further public education to facilitate health consumers’ ability to effectively find health information on the Internet and to make use of such information in an effective manner. Results of this analysis reveal interesting patterns of technology adoption across three basic health-related activities (i.e. information seeking, communication and personal health information management). While these trends may seem preliminary for some activities (e.g. given the limited infrastructure in place to support activities such as personal health information management), the results highlight population differences in the use of eHealth and health information. For example, this study indicated that one dimension of health literacy—the ability to easily use health statistics—was significantly related to whether respondents accessed the Internet. The numeracy measure is an incomplete measure of health literacy but it does emphasize the role of education or literacy in influencing basic online behavior. While recent federal programs in the USA related to the ARRA call for institutional mechanisms, such as regional extension centers (RECs) to train and disseminate knowledge related to the adoption and use of HIT by healthcare providers (e.g. physicians, hospitals, etc.), recurring differences among health consumers’ eHealth technology adoption signals a persistent need to provide both basic educational programs for information technology and health information technology to traditionally underserved groups in the USA.
Footnotes
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.